
Abstract
Objective
Dizziness is a symptom of acute mountain sickness (AMS). This study tested whether immediate fall in systolic blood pressure (BP) on standing was more severe at altitude and whether this was associated with symptoms of dizziness.
Methods
Eighty-five lowlanders flew into La Paz, Bolivia (3650 m), and after 4 to 5 days of acclimatization ascended in 90 minutes to the Chacaltaya Laboratory (5200 m) by road. Blood pressure was measured on 5 occasions, 3 times at 5200 m and twice at sea level, before and after the expedition using a mercury sphygmomanometer. Both a supine and an erect (within 15 seconds of standing) BP measurement were recorded. Participants recorded whether they felt dizzy on standing. A mixed-effect model was used to test for a difference in the change in BP for time and altitude.
Results
The immediate fall in systolic BP observed on standing was significantly greater (P < .001) on all 3 altitude study days (18.2, 23.4, and 20.7 mm Hg) than at sea level (12.2 and 12.4 mm Hg). There was no significant difference in the change in diastolic BP or change in mean arterial BP between sea level and altitude.
Conclusions
The immediate drop in systolic BP observed on standing was greater at altitude. However, mean arterial pressure was maintained, and we found no association between the degree of immediate fall in BP and dizziness or AMS.
Introduction
Dizziness is traditionally thought to be part of acute mountain sickness (AMS) and is a component of the Lake Louise AMS scoring system. The Lake Louise questionnaire does not specify that this dizziness must be associated with any particular activity, such as lying, sitting, or changing posture. 1 Indeed, from our experience patients typically complain of “dizziness” but only on direct questioning make the connection between these symptoms and a change in posture. Conceivably if there was a greater fall in blood pressure (BP) on standing at altitude, suggested by the poorer orthostatic control observed on tilt-table tests, 2 –5 this could account for the greater incidence of dizziness reported using the Lake Louise scoring system or if particularly severe could cause syncope. Syncope, a sudden transient loss of consciousness that resolves spontaneously, has been reported to occur more frequently on arrival at altitude. 6
The widely used consensus definition for orthostatic hypotension proposed by the American Autonomic Society and the American Academy of Neurology Consensus Committee refers to a systolic BP drop of at least 20 mm Hg or in diastolic BP of at least 10 mm Hg, within 3 minutes of standing. 7 Wieling et al, however, use the term “initial orthostatic hypotension,” or IOH (defined as systolic BP fall of >40 mm Hg and/or diastolic BP fall of >20 mm Hg, together with symptoms of cerebral hypoperfusion), to define the initial fall in BP and distinguish this from “typical orthostatic hypotension,” a fall in systolic BP of >20 mm Hg or diastolic BP of >10 mm Hg occurring after 3 minutes of standing. 8
Previous studies including a total of 47 participants have measured BP changes in response to head up tilt (HUT) at high altitude. 2 –4,9 This procedure eliminates the contraction of the calf muscles, which promotes venous return, and so may be less relevant in terms of dizziness occurring during normal activities. These studies did not measure BP immediately after a change in posture. We wished to assess dizziness that occurred immediately on standing while at altitude and therefore chose to manually measure the immediate orthostatic changes in BP.
Methods
The study was part of the Apex 2 (Altitude Physiology Expeditions) high-altitude research expedition to Bolivia during August and September 2003. The study protocol was approved in advance by the Lothian Research Ethics Committee. Participants of the Apex 2 expedition were recruited by poster advertisement and word of mouth from the general student population of the University of Edinburgh, Scotland. A number of other students volunteered from other universities. Volunteers were excluded from the expedition if they 1) had significant cardiorespiratory disease; 2) took cardiovascular medications; 3) had an admission to hospital with acute asthma; 4) were pregnant; 5) were allergic to sildenafil, ascorbic acid, tocopherol acetate, or α-lipoic acid; or 6) smoked. Each volunteer provided written informed consent before participating.
Volunteers flew to La Paz from the UK and after 4 or 5 days ascended by road to the Chacaltaya Laboratory. The ascent profile, together with the sample days, is shown in Figure 1. There were 5 sample days (2 at sea level [1 before departure {SL1} and 1 after return to the UK {SL2}] and 3 at an altitude of 5200 m at the Chacaltaya Laboratory [on day 1 {CH1}, day 3 {CH3}, and day 7 {CH7}]). Volunteers were included in the analysis if they had both a sea level BP reading and a reading at altitude. Volunteers who had gastroenteritis (potential dehydration) were excluded, and volunteers taking salbutamol (a vasoactive drug) were excluded.
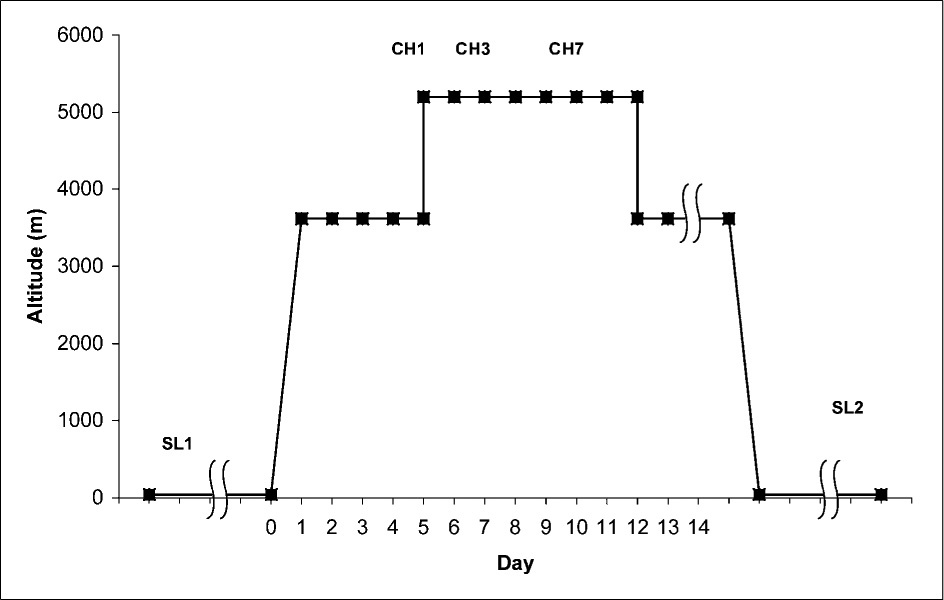
Diagram of the ascent profile and sample days. SL1 and SL2 occurred 1 to 2 months before and after altitude, respectively; SL1 = pre-expedition sea level sample day, Edinburgh (no drugs taken); CH1 = day 1 at Chacaltaya Laboratory (5200 m); CH3 = day 3 at Chacaltaya; CH7 = day 7 at Chacaltaya; SL2 = postexpedition sea level sample day, Edinburgh.
Participants were involved in other experiments as part of the expedition, including a randomized placebo-controlled drug trial investigating the effect of sildenafil (50 mg 3 times daily orally) on pulmonary artery pressure and of an antioxidant supplement (1 g
We measured BP by auscultation using a mercury sphygmomanometer, following British Hypertension Society guidelines, 10 on the 5 sample days. Supine BP was measured after a period of at least 2 minutes in a supine position. Erect BP was measured within 15 seconds of standing; the cuff was preinflated before standing to enable a rapid measurement. Due to constraints with other experiments, BP measurements were made throughout the day. Volunteers were asked to report if they experienced symptoms on standing upright using the following faint scale: no symptoms (1); mild dizziness (2); light headed, vision affected (3); nearly fainted, sat down (4); fainted (5). The hematocrit of venous blood was measured at each sample point. Blood was drawn into a 2.7-mL EDTA tube using an 18-gauge needle with participants in the supine position. Blood was transported, within 24 hours, for analysis at a hematological laboratory in La Paz. Acute mountain sickness was assessed daily using Lake Louise self-assessment score sheets. 1
We analyzed results in Stata (version 8. 2: StataCorp, Texas, USA). A mixed effect model, which made allowance for missing data, equivalent to a multilevel repeated measures analysis, 11 was used to test for a difference in the change in BP on standing (systolic and diastolic) with time (and altitude), gender, and drug treatment group. This method includes data that occurred at any time point, avoiding the bias that could be introduced by excluding participants with missing values.
We performed the following secondary analyses. The initial analysis was repeated using mean arterial BP (


Results
One hundred and three volunteers were recruited to take part in the expedition. Eighteen volunteers were excluded (4 had incomplete sea level control data, 9 were evacuated from the high-altitude laboratory with altitude illness before data were collected, 3 had gastroenteritis at altitude, and 2 used daily salbutamol) from the analysis. Eighty-five participants (45 male, 40 female) were included in the analysis. The eighty-five participants over 5 sample days gave a maximum of 425 paired BP measurements; of this maximum, a total of 41 were missing for the following reasons: SL1, 1 participant absent; SL2, 2 participants absent; CH1, 8 logistical problems; CH3, 9 evacuations; 5 data missing; CH7, 14 evacuations; 1 data missing; 1 withdrew. The change in diastolic BP was difficult to measure because 1) the change in Korotkoff sounds (IV or V) at diastolic BP were less distinct than the changes at systolic (Korotkoff I) and 2) for some individuals Korotkoff IV and V were absent (Korotkoff III persisting to pressure 0 mm Hg); an additional 27 measurements for the change in diastolic BP were missing. These were distributed as follows: SL1, none; SL2, 6; CH1, 5; CH3, 8; CH7, 8.
Blood pressure measurements were made between 10
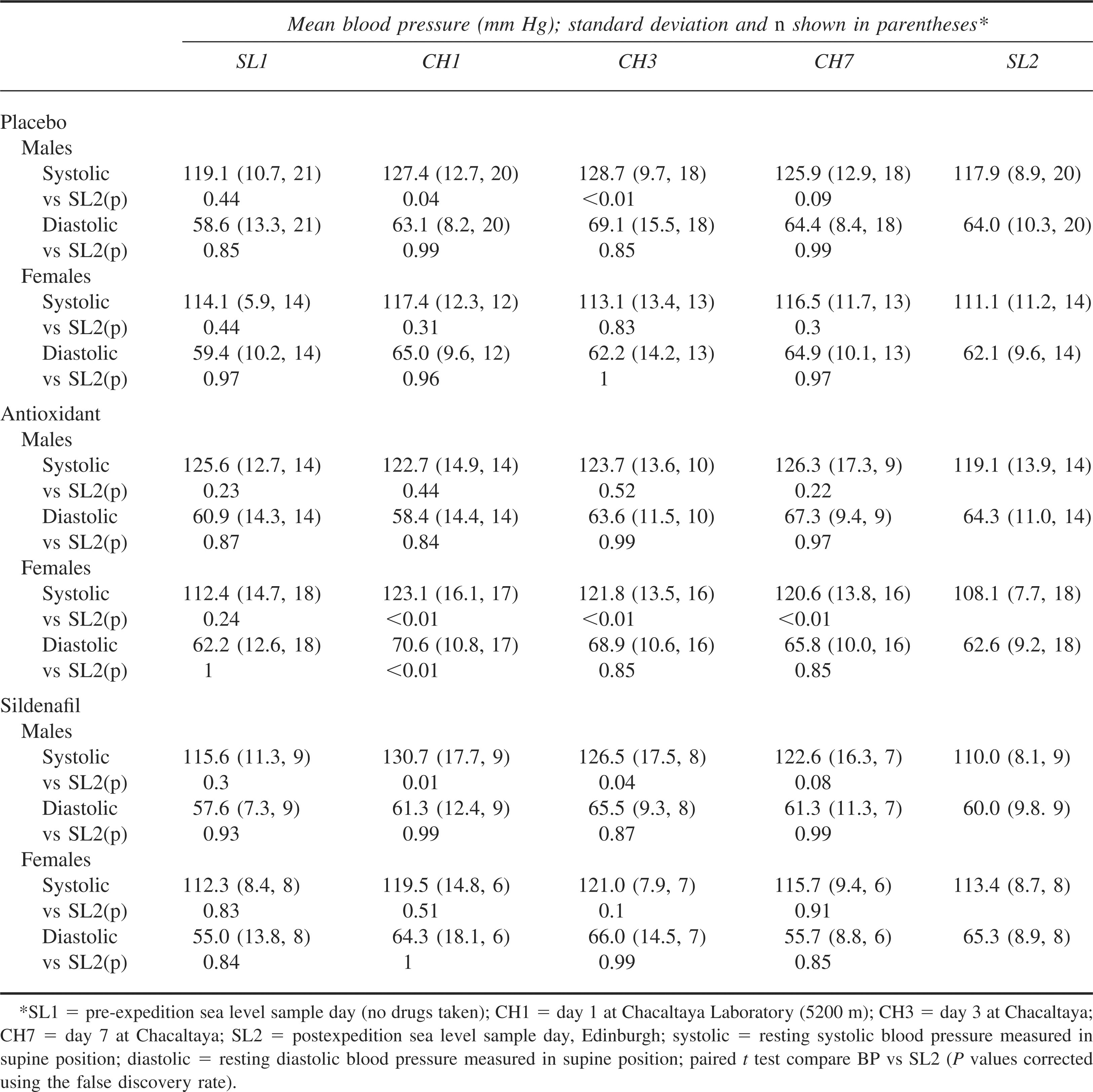
The resting supine BP values are shown in Table 1. Supine BP was higher at altitude, although the only significant differences were for female participants taking antioxidants (CH1, CH3, and CH7), male participants taking sildenafil (CH1 and CH3), and male participants taking placebo (CH1 and CH3).
Supine blood pressure measurements for the 3 different drug groups split by gender
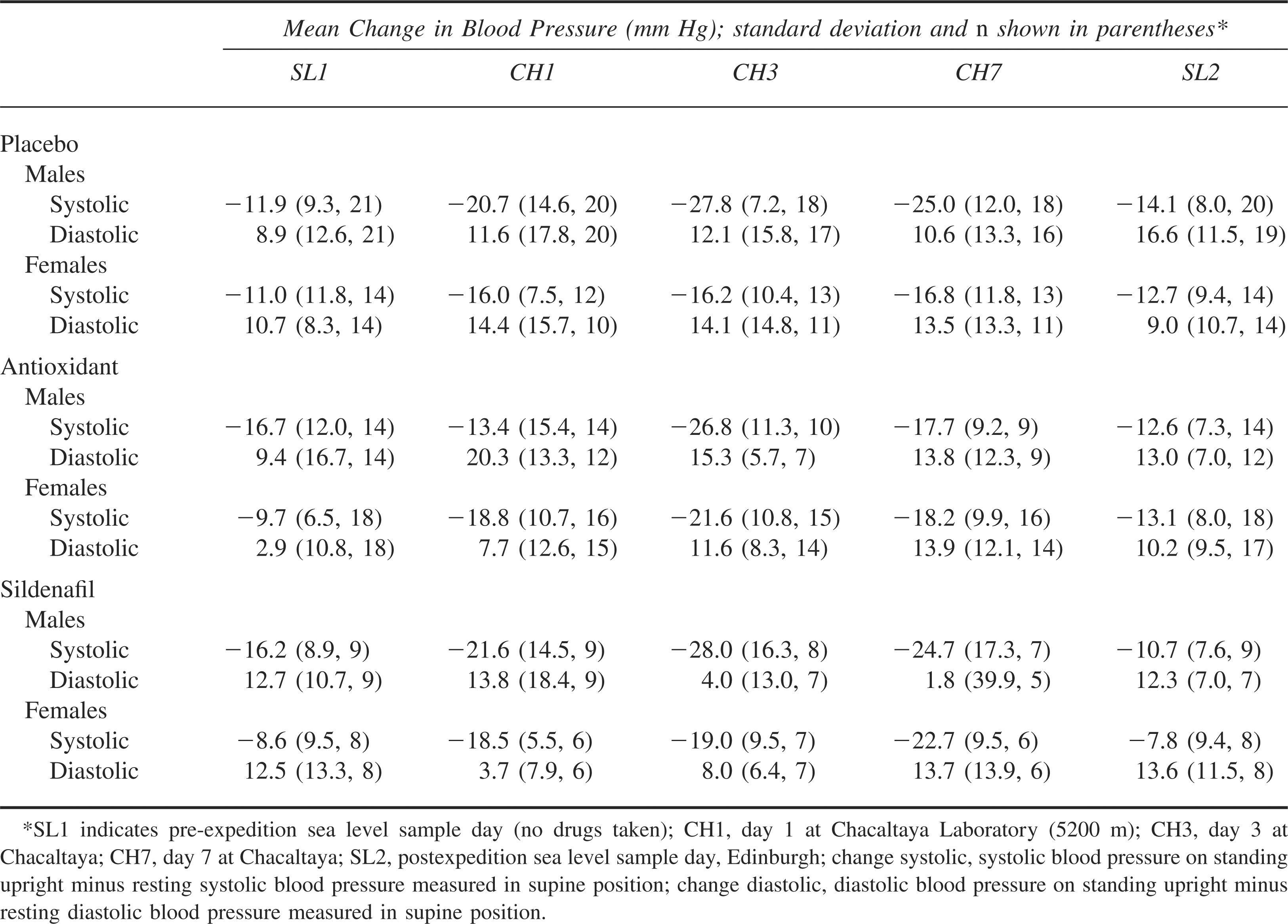
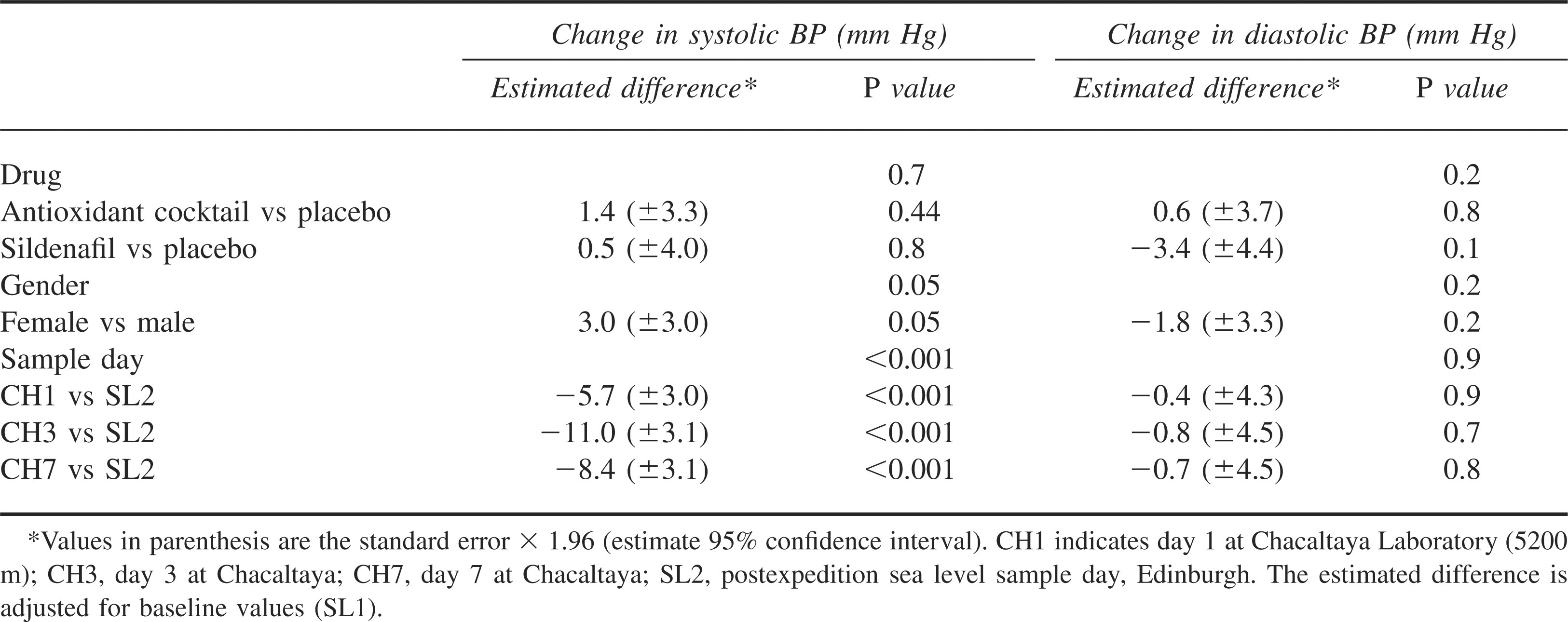
The mean systolic BP fell and the mean diastolic BP rose on standing up from a supine position, both at sea level and at altitude, as shown in Table 2. The results of the mixed effect model are shown in Table 3. The fall in systolic BP on standing was significantly greater on all of the 3 altitude sample days, in comparison with the second sea level sample day (P < .001). There was no significant difference in the rise in diastolic BP between sea level and altitude. Gender or drug (placebo, antioxidant, sildenafil) did not have any significant effect on the orthostatic BP. The prevalence of initial orthostatic hypotension (defined as systolic fall >40 mm Hg or diastolic fall >20 mm Hg with a faint score of 2 or greater) was not significantly different between sea level and altitude (SL1 2.3% [2/84] vs CH1 6.5% [5/77], χ2paired = 0.25, P = .62; CH3 4.3% [3/71], χ2paired = 0.25, P = .62; CH7 5.7% [4/69], χ2paired = 0.17, P = .68; SL2 0% [0/83] vs CH1, χ2paired = 3.20, P = .07; CH3 χ2paired = 0.50, P = .48; CH7 χ2paired = 0.50, P = .48).
. Mean change in blood pressure on standing for the 3 different drug groups split by gender
. Mixed effect model estimates for the effect of drug, gender, and sample day on the change in blood pressure (BP) on standing*
Changes in mean arterial BP (MABP) on standing upright at altitude in comparison with sea level (orthostatic MABP; 2.0 mm Hg to 0.2 mm Hg, 1.0 mm Hg for CH1, CH3, and CH7, compared with 1.7 mm Hg and 4.3 mm Hg for SL1 and SL2) were not significant (mixed effect model, P = .07).
No participant experienced symptoms graded 4 or 5 (nearly fainting or fainting). The prevalence of symptoms of dizziness (either mild dizziness or feeling lightheaded with vision affected) was significantly greater on the first altitude sample day in comparison with SL2 (SL2 = 45.0%, n = 80, χ2paired = 4.36, P = .04) and second altitude sample day (CH3 = 67.1%, n = 70 vs SL1 χ2paired = 6.50, P = .01; SL2 χ2paired = 4.00, P = .046). Differences on the third sample day (CH7 = 54.3%, n = 70 vs SL1 χ2paired = 1.75, P = .19; SL2 χ2paired = 0.56, P = .46) and the first sample day in comparison with SL1 (CH1 = 62.7%, n = 75 vs SL1 = 48.3%, n = 60, χ2paired = 1.89, P = .16) were not significant. The prevalence of grade 3 symptoms (feeling light headed, vision affected) at altitude was 12.0%, 8.6%, and 5.7%, for CH1, CH3, and CH7 respectively, compared with sea level, 1.7% and 2.5% for SL1 and SL2. These differences were not significant (SL1 vs CH1 χ2paired = 2.29, P = .13; CH3 χ2paired = 4.17, P = .04; CH7 χ2paired = 0.25, P = .62; SL2 vs CH1 χ2paired = 3.27, P = .07; CH3 χ2paired = 1.13, P = .29; CH7 χ2paired = 0.57, P = .45).
The fall in systolic BP of participants who experienced symptoms of dizziness compared with those participants not experiencing symptoms of dizziness is shown in Figure 2. The fall in systolic BP experienced by participants who reported dizziness in their Lake Louise AMS questionnaire compared with those who experienced no dizziness was not significantly different (CH1 17.5 mm Hg [n = 33] vs 18.6 mm Hg [n = 44], P = .70; CH3 23.9 mm Hg [n = 15] vs 23.3 mm Hg [n = 56], P = .84; CH7 21.6 mm Hg [n = 4] vs 20.0 mm Hg [n = 60], P = .78; SL2 11.6 mm Hg [n = 7] vs 12.4 mm Hg [n = 79], P = .78). Only 1 participant reported dizziness on the Lake Louise AMS questionnaire on SL1. The fall in systolic BP for participants who had AMS (Lake Louise score ≥3) was not significantly different from those participants who did not have AMS (CH1 17.1 mm Hg [n = 56] vs 21.0 mm Hg [n = 21], P = .26; CH3 22.4 mm Hg [n = 40] vs 24.7 [n = 31], P = .38; CH7 24.1 mm Hg [n = 15] vs 21.0 mm Hg [n = 47], P = .21).
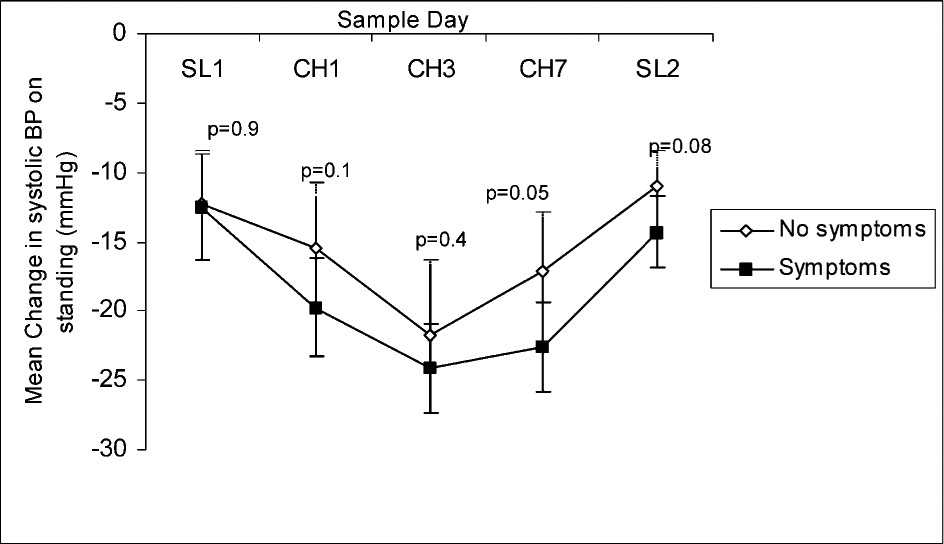
The change in systolic blood pressure on standing comparing those volunteers who felt faint on standing with those who did not. SL1 = pre-expedition sea level sample day (no drugs taken); CH1 = day 1 at Chacaltaya Laboratory (5200 m); CH3 = day 3 at Chacaltaya; CH7 = day 7 at Chacaltaya; SL2 = postexpedition sea level sample day, Edinburgh; P values shown above line, unpaired t test symptoms vs no symptoms, with Bonferroni's correction; Error bars represent the standard error.
The mean hematocrit was greater at altitude than sea level (SL1 44.0 [n = 67] vs CH1 46.8 [n = 78], P < .01; vs CH3 48.6 [n =74], P < .01; vs CH7 48.9 [n = 72], P < .01): SL2 40.5 [n = 85] vs CH1, P < .01; vs CH3, P < .01, vs CH7, P < .01). However, we did not find a significant correlation between the change in systolic BP on standing and the change in hematocrit from sea level (CH1, r = −0.21, n = 72, P = .08; CH3 r = −0.21, n = 66, P = .08; CH7 r = −0.13, n = 68, P = .26).
Discussion
We observed a greater initial fall in systolic BP at altitude in response to a normal physiological challenge, standing upright from a supine position. The nadir in BP occurs approximately 7 seconds after standing (observed at sea level). 8 Therefore, it is likely that our technique for measuring BP (approximately 15 seconds after standing) would have missed this nadir. The observed increased fall in systolic BP could be due to a fall in BP to a greater nadir or may reflect a different time course in the immediate BP fall at altitude. For example, if at altitude the BP nadir occurs after 7 seconds or the rise in BP after the nadir occurs more slowly (in comparison with sea level), the measured BP at 15 seconds would be lower at altitude than sea level. However, missing the nadir would have led to an underestimate of the true prevalence of “initial orthostatic hypotension” in this study. Mean arterial BP was well preserved in response to orthostatic challenge at both sea level and altitude, the rise in diastolic BP compensating for a fall in the systolic BP.
It is difficult to compare our experiment, using active standing, to previous work using HUT. It is unclear how the 2 measurements compare at sea level. Wieling et al reported no initial fall in BP in response to HUT and a corresponding large fall on active standing. 8 The mechanisms for the fall in BP in response to active standing, compared with passive HUT, are unclear but may relate to the action of the calf muscle pump. However, the absence of an initial postural fall on HUT has not always been observed. Gabett et al found a significant fall in BP in both young and old participants on HUT within 30 seconds. 13 The fall was particularly marked among the younger participants on initial HUT.
Comparisons are further complicated because previous experiments comparing altitude and sea level 2 –5 not only used tilt tables but also measured BP after prolonged HUT (a period of >1 minute) or took an average of several readings across time. The BP fall in response to prolonged HUT (or postural change), sometimes termed “typical orthostatic hypotension,” is different to the initial orthostatic hypotension, 8 which we attempted to measure. The mechanisms responsible for “typical” and “initial” orthostatic hypotension may be different, so comparisons would be unfair.
Nonetheless, with the exception of Sagawa et al, previous work 2 –4 has demonstrated a greater fall in postural BP at altitude in comparison with sea level. Sagawa's group found no difference between the fall in BP (measured at 2 minutes) between sea level and altitude, although the observed fall persisted longer at altitude than at sea level. 5 However, this experiment was conducted in a pressure chamber at a simulated altitude of 3700 m (lower than our high-altitude laboratory), and participants were therefore exposed to a warm (29°C) and relatively humid environment (relative humidity 60%) with a more acute ascent profile. Dehydration is unlikely to have occurred in this setting, suggesting that a possible reason for the reduction in “typical orthostatic hypotension” found in other studies at altitude may have been a reduction in plasma volume.
A reduction in circulating plasma volume might too be expected to lead to greater initial orthostatic hypotension. However, we found a poor correlation between the observed fall in systolic BP and measures of reduced plasma volume at altitude (change in hematocrit from sea level). This raises the possibility of alternative mechanisms contributing to the greater observed immediate fall in systolic BP. Measurement of pulse, real-time BP changes, cardiac output, peripheral resistance, and plasma volume would help determine the nature of and reasons for the observed greater immediate fall in BP at altitude.
Symptoms of dizziness on standing were more common at altitude than at sea level. The observed differences were significant only on the first (in comparison with SL2) and second sample days, although our population size was relatively small. Although those volunteers who had symptoms of dizziness at altitude consistently had a greater fall in systolic BP, the difference was small (2 to 6 mm Hg), did not reach statistical significance, and was comparable to that observed at sea level (0 to 3 mm Hg). It therefore seems unlikely that the greater observed fall in systolic BP at altitude causes more dizziness on standing at altitude. Individuals who reported dizziness on their Lake Louise AMS scoring sheet or who had AMS did not have a significantly different fall in systolic BP compared with those not reporting symptoms. This suggests that the dizziness that is part of AMS is not related to orthostatic hypotension.
Resting BP has been shown to rise at altitude in the short term, attributed to a rise in circulating catecholamines.4,14 Our study found that resting supine BP was greater at altitude, but the rise was only significant for women taking antioxidants and for men taking sildenafil and placebo (CH1 and CH3). This pattern was not expected, and given the small numbers in each of these groups, we should be cautious about drawing conclusions from this pattern.
Despite this study being the largest of its kind, our participants were all young healthy volunteers and the vascular response of older participants to altitude could be different. The use of a vasodilator, sildenafil, was a potentially confounding factor in this study, although our analysis suggested that it did not have a significant effect on orthostatic BP. The majority of the readings (<90%) were conducted by 3 observers. However, the proportions of BP measurements recorded by each observer changed between sea level and altitude. Finally, the observed orthostatic hypotension may be due to dehydration, and future studies could attempt to control for this factor.
Conclusions
Greater immediate falls in systolic BP in response to a simple orthostatic challenge are observed at altitude. Despite the greater fall in systolic BP, mean arterial BP on standing is well maintained. These changes do not appear to be clinically significant or relate to the dizziness included in the Lake Louise scoring system.
Footnotes
Acknowledgments
We thank the volunteers and supervisors who took part in Apex 2, especially Kenneth Baillie; Matthew Bates; Simon Maxwell; Nikhil Hirani; David Webb; Jeff Gertsch; Simon Travis; Brian Angus; Jim MacFarlane; Karen Wood; the Wellcome Trust Clinical Research Facility, Edinburgh, Scotland; the Instituto de Investigaciones Fisicas, Universidad Mayor de San Andres, La Paz, Bolivia; and the Instituto Boliviano de Biología de Altura, La Paz, Bolivia. Pfizer UK and Cultech Ltd (Wales) provided the sildenafil and antioxidant supplement, respectively.
*
This work was presented at the Hypoxia Symposium, Lake Louise, Alberta, Canada, February 2005.