
Abstract
Introduction
Suspension syndrome (SS) develops when venous blood pools in extremities of passively suspended individuals, resulting in presyncopal symptoms and potential unconsciousness or death independent of additional injuries. We investigated use of leg raising to delay onset of SS, as it can decrease venous pooling and increase cardiac return and systemic perfusion.
Methods
Participants were suspended in rock climbing harnesses at an indoor climbing wall in a legs-dangling control position or a legs-raised interventional position to compare physiological outcomes between groups. Participants were suspended for a maximum of 45 min. Onset of 2 or more symptoms of SS, such as vertigo, lightheadedness, or nausea, halted suspension immediately. We recorded each participant's heart rate, blood pressure, oxygen saturation, lower leg oxygen saturation, pain rating, and presyncope scores presuspension, midsuspension, and postsuspension, as well as total time suspended.
Results
There were 24 participants. There was a significant difference in total time suspended between groups (43.05±6.7 min vs 33.35±9.02 min, p=0.007). There was a significant difference in heart rate between groups overall (p=0.012), and between groups, specifically at the midsuspension time interval (80±11 bpm vs 100±17 bpm, p=0.003). Pain rating was significantly different between groups (p=0.05). Differences in blood pressure, oxygen saturation, lower leg oxygen saturation, and presyncope scores were not significant.
Conclusion
Leg raising lengthened the time individuals tolerated passive suspension and delayed symptom onset.
Keywords
Introduction
Suspension syndrome (SS) is a collection of physiological signs and symptoms that occur during prolonged passive suspension. Although time to symptom development is not known, time from symptom onset to syncope can occur rapidly. 1 SS can occur when a person is suspended free-hanging in a harness, in activities such as mountaineering, rock climbing, caving, and in industries working at heights.1–4 During suspension, venous blood pools in the lower extremities, affecting hemodynamics.2,5 This situation can lead to a 20% reduction in circulating blood volume, causing functional hypovolemia, which can induce presyncopal symptoms and, in rare situations, loss of consciousness or death.2,5 Outcomes are especially poor if victims are unconscious or exhausted and unable to engage their leg muscles, as this circumstance can result in decreased venous return and cardiac output, reducing time to onset of SS.1,2,4 An early study replicated symptoms of SS with passive tilt-tables, resulting in hypotension, bradycardia, and presyncopal symptoms within 1 h in 69 of 79 test subjects. 6 Subsequent studies found similar results, with some harness-suspended participants experiencing presyncopal symptoms and losing consciousness within 7 to 30 min.2,7,8 Although these initial investigations provided foundational research into SS, they focused on tilt-table experiments or fall-arrest harnesses and mitigation strategies for industrial settings, such as foot strops and stepping slings.7,8 We were interested in outdoor recreational and occupational activities prone to occurrences of SS and wanted to investigate anecdotal interventions used by arborists to prevent SS. The aim of the study was to investigate leg raising as a nonindustrial prevention strategy for SS, specifically in situations where victims are unable to actively participate in their own rescues.
Reports from mountaineers, arboriculture experts, and occupational safety organizations detail the dangers of SS—notably, syncope and death—but often lack conclusive recommendations for management of suspended victims.2,3 Many of these reports are historical and include discussions of “rescue death,” the suggestion that harness straps cause SS, and recommend that victims should not be placed horizontally immediately after rescue.5,9 These claims have since been disproven, but they linger in literature.5,9 Through this pilot study, we explored the efficacy of raising a passively suspended participant's legs as a therapeutic intervention in aerial suspension. We hypothesized that leg raising could minimize development of symptoms of SS and increase time to symptom onset. We evaluated heart rate, blood pressure, oxygen saturation, pain rating, and presyncope score as indicators of SS.
Methods
Study Approval and Ethics
The University of Birmingham (UoB) Science, Technology, Engineering and Mathematics Ethical Review Committee granted ethical approval for this study (ERN_22-0748). We informed participants about experimental procedures, possible risks or benefits of participation, and participant rights through climbing wall waivers, information leaflets, and participant consent forms.
Participants
We chose UoB students as subjects, as the experiment occurred on campus during students’ spring term and we had access to the campus rock-climbing wall. To recruit participants, we posted flyers on UoB's main campus and Medical School and UoB student-based social media pages. Participants were eligible if they were current UoB students with valid student email addresses. After initial recruitment, we selected participants for participation by random number generator. We asked prospective participants whether they identified as males or females, but we did not use this information as an inclusion criterion. We consented these participants 24 h prior to experimental sessions. We also requested that participants avoid alcohol, caffeine, and moderate to intense physical activity within 24 h of their experimental session. Some participants were unable to continue due to scheduling difficulties or compliance with abstaining from caffeine or alcohol. We replaced them with other individuals randomly sampled from the remaining potential study participants by using a random number generator. We also required participants to complete the Physical Activity Readiness Questionnaire (PAR-Q). The PAR-Q screens for potential health risks associated with starting an exercise program and is reliable in university student populations. We used it to ensure safety and to avoid introducing confounding variables into the experiment. 10 We based sample size on previous research with sample sizes of 20 and increased it to 24 to accommodate possible participant attrition.4,11,12 Participants were partially blinded during the experiment, as they knew that they were participating in a study regarding suspension position but were unaware of the potential importance of suspension position differences or of outcome measures.
Materials
We used DMM Brenin rock climbing sit-harnesses and screwgate carabiners to suspend participants in free hanging positions. All harnesses were identical and were similarly fitted per manufacturer recommendations by a certified climbing wall instructor prior to suspension. Once harnesses were fitted to participants, we used an additional 240 cm DMM Dyneema sling, 2 additional carabiners, and a Wild Country Ropeman ascender to raise participants’ legs while they were suspended and a separate 240 cm DMM Dyneema sling to counter center-of-gravity displacement. We used a Petzl hand ascender and an etrier to assist participants in achieving a suspendable height: 1 m off the ground. We used a Welch Allyn Vital Signs Monitor 300 (Welch Allyn Inc, Skaneateles Falls, NY), a Welch Allyn Spot Vital Signs LXi device (Welch Allyn Inc, Skaneateles Falls, NY), a Welch Allyn Connex Spot Monitor (Welch Allyn Inc, Skaneateles Falls, NY), and a Mindray Datascope DUO Spot Monitor (Mindray Medical International Limited, Shenzhen, China) to record heart rate, blood pressure, and oxygen saturation.
Design
We collected observations pre-, mid-, and postintervention. We randomly assigned participants to testing sessions on 1 of 2 testing days and to the intervention or control group by using a random number generator. Each group had 4 participants—2 control participants and 2 intervention participants—with equal numbers of control and intervention participants tested on each study day. The independent variable was suspension position: either the interventional legs-raised position or the neutral control position. We measured heart rate, oxygen saturation, blood pressure, lower leg oxygen saturation, pain rating, presyncope score, and total time suspended. We documented variables at pre-, mid-, and postsuspension, except for total time suspended, which we documented postsuspension. We measured heart rate, oxygen saturation, and lower leg oxygen saturation by fingertip pulse oximeter and blood pressure with an automated blood-pressure cuff. We measured presyncope scores with a checklist detailing each sign or symptom with yes or no checkboxes (Figure 1). Participants verbally stated yes or no to each symptom, and investigators documented pallor. 4 We totaled yes answers for numerical presyncope scores ranging from 0 to 6. We measured pain rating on a 10-step numeric rating scale, with 0 being no pain and 10 being the worst possible pain. 13
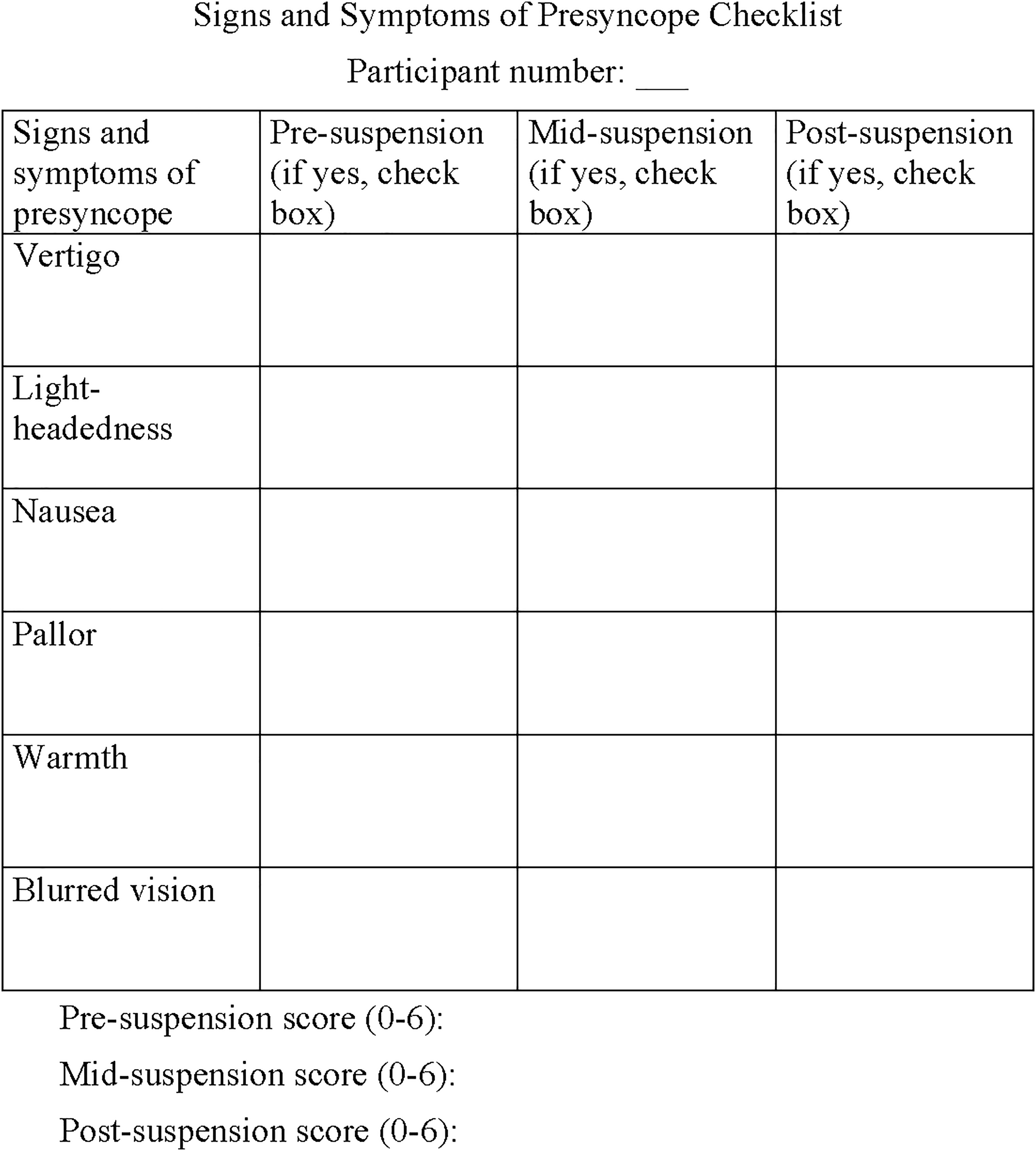
Presyncope checklist of signs and symptoms.
Procedure
We suspended participants for a maximum of 45 min and instructed them to avoid moving their legs while in suspension. The control group (n=12) hung in a neutral position with torso upright and legs dangling, maintaining their upright position without an additional sling (Figure 2A). The intervention group (n=12) hung with torso upright and legs raised, with an additional sling in the axilla to counter center-of-gravity displacement (Figure 2B). Intervention group participants had standardized raised-leg positions, as each participant's knees were raised approximately 15 cm above the waist. We continuously monitored variables and documented them at 3 time intervals: presuspension, with participants supine 1 min prior to suspension; midsuspension, after 20 min of suspension; and postsuspension, with participants supine within 1 min after suspension terminated. We discontinued suspension for participants meeting any of the following criteria: participant requested to stop; the 45 min time limit was reached; heart rate decreased below 45 bpm or increased more than 40 bpm from baseline; any decrease, from baseline, in systolic blood pressure of >20 mm Hg or decrease in diastolic blood pressure of >10 mm Hg; Glasgow Coma Scale score ≤14; oxygen saturation ≤94%; or 2 or more presyncopal signs or symptoms occurred.
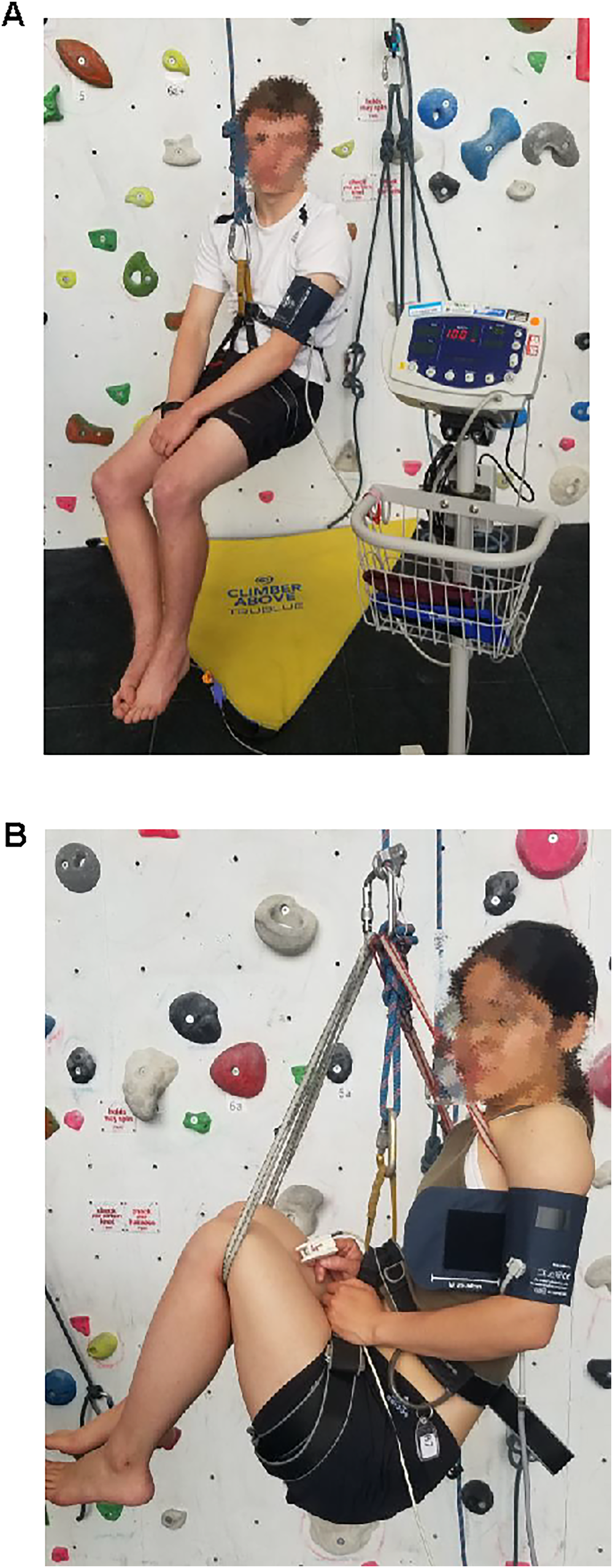
(A) Control group suspension position and (B) intervention group suspension position.
Statistics
We ran statistical analyses with SPSS version 28.0.1.1 (IBM Corp., Armonk, NY). We used 1-way multivariate analyses of variance (MANOVAs) to evaluate differences between control and intervention groups across each dependent variable, barring total time suspended, at midsuspension and postsuspension. Mid- and postsuspension time interval data were analyzed to determine whether the intervention led to a significant difference between groups overall or whether it had more impact at one stage of suspension or another. We also used a 1-way analysis of variance (ANOVA) to analyze differences in total time suspended between groups. We used a p value of ≤0.05 to indicate a statistically significant difference and an eta squared value (η2) of >0.138 to indicate a large effect size. 14 Additional descriptive statistics were expressed as mean±standard deviation.
Results
There were 28 individuals initially recruited for the study, with 24 selected for participation by random number generator. Three of the 24 were unable to participate due to time factors or inability to comply with the conditions of the study. We replaced them with 3 other individuals randomly selected from the remaining potential study participants by using a random number generator. Prior to final participant selection, we excluded 4 individuals who volunteered for the experiment based on their affirmative answers to the PAR-Q and replaced them with other volunteers who did not answer the PAR-Q affirmatively. The experiment started with 24 participants who were12 male-identifying individuals and 12 female-identifying individuals. We randomized participants to the intervention or control group, with presuspension measurements collected for all participants prior to suspension. However, 2 control-group participants terminated suspension due to onset of presyncopal symptoms before the 20 min midsuspension time point. Their data were not collected for midsuspension or postsuspension and were solely used in the total time suspended analysis. All additional participants who discontinued their suspension early terminated due to onset of presyncopal symptoms. One of the 12 intervention-group participants and 11 of the 12 control-group participants ended suspension after midsuspension data collection but before the 45 min maximum suspension time.
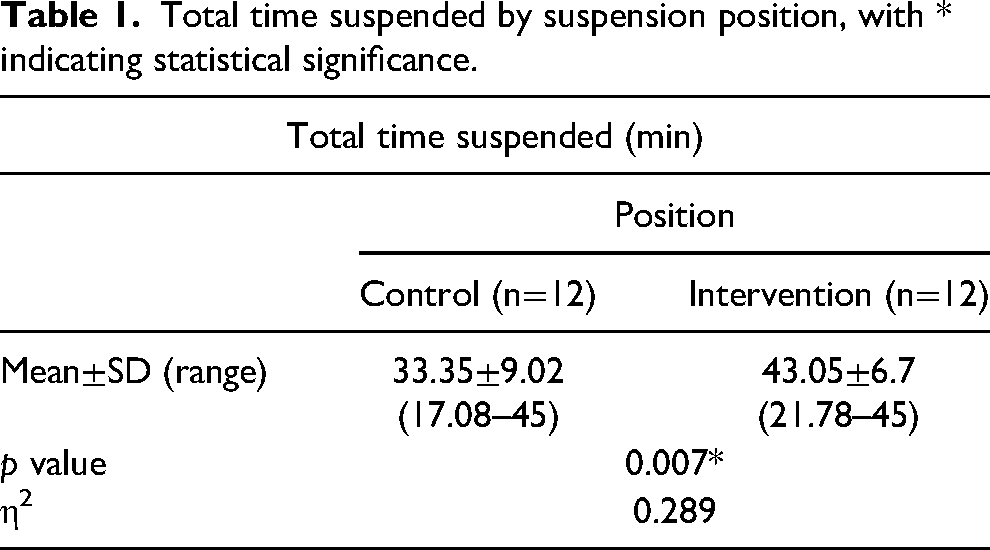
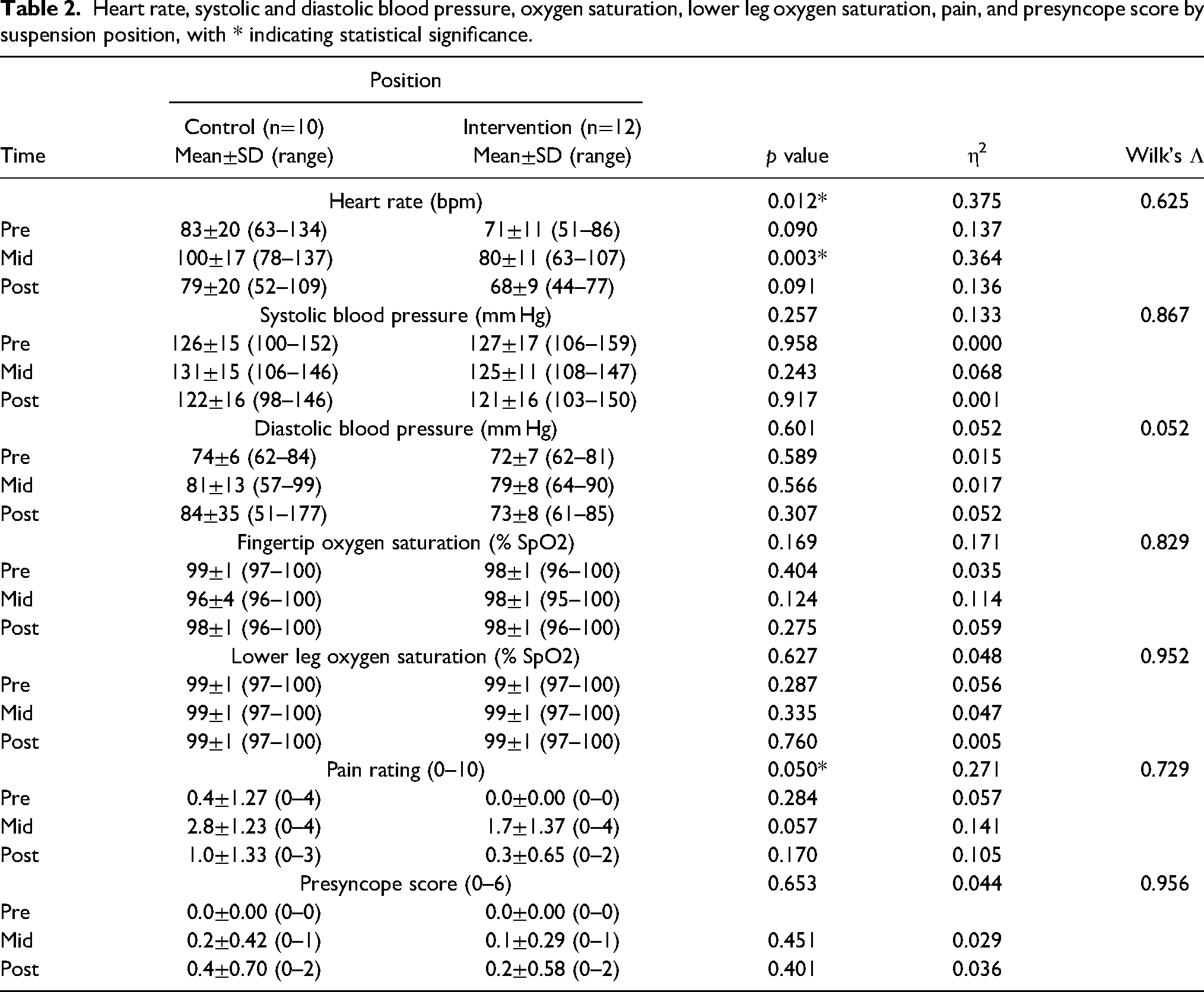
Tables 1 and 2 show descriptive statistics for the primary outcome variable and secondary outcome variables at each suspension time point. The ANOVA results for total time suspended indicated a significant difference between the intervention and control groups (43.05±6.7 min vs 33.35±9.02 min, p=0.007). The MANOVA results for overall heart rate, as a composite of mid- and postsuspension time-interval data, indicated a significant difference between the intervention and control groups (p=0.012). MANOVA heart rate results also indicated a significant difference between the intervention and control groups, specifically at the midsuspension time interval (80±11 bpm vs 100±17 bpm, p=0.003). Pain rating, as a composite of mid- and postsuspension time-interval data, was significantly different between the intervention and control groups (p=0.05). No other variables resulted in significant findings.
Total time suspended by suspension position, with * indicating statistical significance.
Heart rate, systolic and diastolic blood pressure, oxygen saturation, lower leg oxygen saturation, pain, and presyncope score by suspension position, with * indicating statistical significance.
Discussion
Participants whose legs were raised tolerated significantly longer suspension times than participants whose legs were not raised and, unexpectedly, displayed less lower extremity mottling, which can represent an early symptom of SS. These findings may contribute to understanding how to reduce symptoms of SS or delay symptom onset in passively suspended individuals through insight into optimal body positioning. This information may lead to consistent, applicable intervention recommendations for emergency workers and first responders by providing definitive suggestions for standard operating procedures relating to aerial rescue. The significant difference in total time suspended between groups, with intervention-group participants having longer suspension times than control-group participants, shows that raising the legs successfully increased time to potential onset of symptoms of SS.
Further insight into the findings of this study may be found in tilt-table studies that explored orthostatic intolerance as the influencing factor in venous return via accumulation of venous blood in the lower extremities. Researchers subjected participants to 50° head-up tilt on a tilt table, with half of those participants experiencing presyncopal symptoms within 27 min of tilting. 6 These presyncopal participants had decreased venous return to the heart, measured by elevated thoracic electrical impedance, reduced central venous saturation, and reduced muscle oxygen saturations. 6 However, researchers found that elevating the legs with a tilt table prevented presyncopal symptoms, much like leg raising with slings did in this study. 6 Although we did not measure venous return, participants unexpectedly displayed venous pooling in the lower extremities in a mottling pattern consistent with livedo reticularis, a process in which blood flow to the superficial, cutaneous arteries is obstructed.11,15,16 Progression of symptoms appeared to follow a sequential pattern: Participants developed paresthesia in the lower extremities, followed by pallor, mottling consistent with livedo reticularis, and presyncopal symptom onset. 15 We documented the presence of livedo reticularis spontaneously with written notes and photographs, as it was an unexpected finding. We did not discuss these findings in the presence of participants to preserve participant blinding. Livedo reticularis was visible in all 12 participants suspended in the control position (Figure 3A) but was not observed in the 12 participants suspended in the intervention position (Figure 3B). This finding may have use in emergency rescue situations as an early indicator of venous pooling or onset of SS.

(A) Mottling (livedo reticularis) in lower extremities of participants in the control position and (B) absence of mottling (livedo reticularis) in lower extremities of participants with legs raised in the intervention position.
As total time suspended, heart rate, and pain rating results were significant, they merit additional research with longer time intervals, larger sample sizes, or continuous data collection methods to further investigate SS and presyncopal symptom onset. Ultrasound and near-infrared spectrometry have the potential to indicate venous pooling and onset of SS by measuring the diameter of the superficial femoral vein.4,11 Although other clinical trials used these methods, they were not used with participants in different suspended positions, such as leg raising versus legs dangling.4,11 Blood tests, such as arterial blood gas testing or plasma catecholamine levels, might be useful to determine onset of SS. For example, arterial blood gas testing could determine arterial oxygenation levels, with lower oxygenation indicating venous pooling and SS. 17 Likewise, plasma catecholamines could be measured to determine epinephrine levels, as these have been shown to increase prior to syncope in tilt-table experiments and could give a more precise indication of presyncopal symptom onset when paired with continual data capture.18,19
Limitations
This was a simulation study, as conducting research on SS during an actual rescue would not be ethical. The measurements chosen to indicate SS may not be accurate representations, influencing interpretation and validity of data or results. This study simulated a scenario in which individuals could not be active participants in their own rescues. The enforced lack of participant movement in this study may have biased the results by inducing symptoms of SS in individuals otherwise able to move. This circumstance may have limited the applicability of the study, as the results pertain specifically to the rescue of unconscious individuals. Using foot loops and pumping the legs to encourage venous return are valid mitigation strategies that have been researched in other studies, 3 but these work best for conscious victims who can be actively involved in their own rescues, not unconscious or exhausted victims, as simulated in this experiment.
Ending suspension after 45 min may have prevented capture of important presyncopal symptom data. Not using continuous measurements may have resulted in missed data, affecting the apparent efficacy of the intervention. The time intervals at which we chose to record data may have been limiting, as not all participants displayed symptoms at or near the 20 min midsuspension mark.
Potential limitations are related to outcome variables, with nearly all specific to data capture. Blood pressure drops 11 at the onset of circulatory decompensation and syncope. Unless this change occurred near the midsuspension recording interval, the data were missed. Heart rate and oxygen saturation did not capture presyncopal symptom onset unless symptoms coincided with the 20 min midsuspension time interval. The signs and symptoms we chose for the checklist, the presyncopal symptom scoring or suspension termination criteria, or the time intervals at which the checklist was recorded may have provided inaccurate understanding of presyncopal symptoms and onset in participants.
The sample size was small because of logistical constraints, so the generalizability of MANOVA/ANOVA results may be limited. The lack of participant demographics meant that no further stratification of results could occur. The study may have been inadequately powered to detect significant differences between groups.
The ability of participants to terminate suspension may have limited their experience of higher levels of pain and other symptoms, potentially resulting in lower pain ratings and fewer perceived symptoms of SS. The experimental testing location could have produced limitations, as facility skylights affected ambient temperature, which may have altered participants’ experience of presyncopal symptoms. Yet as with systolic blood pressure, presyncopal symptom scores were not measured at presyncopal symptom onset unless symptoms coincided with the 20 min midsuspension time interval.
Conclusion
Few studies have investigated onset of SS, particularly in situations where individuals are aerially suspended. We found that leg raising in passively suspended individuals delayed the development of some symptoms of SS, thereby delaying the overall onset of SS. We recommend further investigation into interventions that could delay or prevent symptoms of SS, especially with suspended victims in other recreational or occupational settings.
Footnotes
Acknowledgments
We thank UoB Sport & Fitness Center for use of its indoor climbing wall. Additional thanks go to Geo McIntyre for his assistance in designing the suspension rigs and securing climbing equipment, Bryar Kadir and Ayesha Ali for their statistical advice, and Michael Manarkattu and James Longman for providing medical assistance.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financial/Material Support
All medical equipment was generously loaned by the University Hospitals Birmingham Clinical Education Center.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.