
Abstract
Objective
To describe the prevalence of childhood overweight and obesity in rural high- and low-altitude populations of southwestern Saudi Arabia and to identify specific at-risk groups within these populations.
Methods
A cross-sectional study was conducted on 912 school children and adolescents aged 6–15 years born and living permanently at high altitudes (2800–3150 m) and 972 children and adolescents of comparable ages born and living permanently at low altitudes (≤500 m). Height and weight were measured. For children <10 years, the weight-to-height index according to World Health Organization (WHO) standards was used for assessing overweight and obesity. For adolescents 10–15 years, overweight and obesity were assessed by age and gender-specific percentiles for body mass index based on the WHO/National Centre for Health Statistics reference population. A questionnaire was used for measuring parents’ socioeconomic status.
Results
The overall prevalence of overweight and obesity at high and low altitudes was 10%. The study showed that some school children and adolescents were at a significantly higher risk of developing overweight and obesity. Significant risk factors included moderate-to-high parental income, age ≥10 years, high-altitude birth and residence, and female sex (crude odds ratio 3.2 [95% CI, 1.8–5.5], 2.3 [95% CI, 1.6–3.2], 2.1 [95% CI, 1.5–2.9], and 1.9 [95% CI, 1.4–2.6], respectively). A multivariate analysis using the direct binary logistic regression model revealed that moderate-to-high parental income, age ≥10 years, female sex, and high-altitude birth and residence were significant independent predictors of childhood overweight and obesity. (adjusted OR 3.2 [95% CI, 1.6–2.6], 2.6 [95% CI, 1.8–3.8], 2.0 [95% CI, 1.6–2.9], and 1.8 [95% CI, 1.3–2.6]), respectively.
Conclusion
The present study identified risk factors for childhood overweight and obesity in Saudi Arabia. Among these, high altitude was a significant and independent factor. Future research is warranted to evaluate the exact mechanism by which a high-altitude environment may contribute to childhood overweight and obesity.
Introduction
Childhood obesity is emerging as a serious health problem in developing countries worldwide. 1 –6 It has immediate and long-term health risks. There is an increased risk of diseases, such as hypertension, diabetes mellitus and respiratory and orthopedic problems, as well as emotional stress, associated with overweight and obesity during the growing years. 7 The most significant long-term consequence is its persistence into adulthood along with its numerous associated health risks. 7
The study of the characteristics of childhood obesity in different races and geographic areas can help in defining risk factors for such a problem and thus improve control measures. In the kingdom of Saudi Arabia, there have been several studies addressing the problem of childhood obesity.3,8–13 However, all of these studies were conducted in urban areas where affluent segments are living.
Southwestern Saudi Arabia is less urbanized compared with other regions of Saudi Arabia and is characterized by high- and low-altitude areas. The general impression is that obesity is a rarity among highlanders worldwide. 14 However, a recent study 15 found that although the median values of weight and height for Saudi children living at high altitudes were lower than the corresponding values for children in the United States, the median values of the body mass index (BMI) for Saudi boys aged 3–18 years and girls aged 3–9 years were almost identical to the U.S. National Center for Health Statistics (NCHS) median values. After the age of 9 years, the BMI for Saudi girls was higher than that for girls in the United States. 15 However, no actual prevalence rates of overweight or obesity were given in this study.
Therefore, the present study was undertaken to describe the prevalence of overweight and obesity among school children and adolescents in rural high- and low-altitude populations in the southwestern part of Saudi Arabia and to identify specific at-risk groups within these populations. Prevalence differences were examined by age, sex, altitude, and socioeconomic status (SES) of the subjects’ parents.
Methods
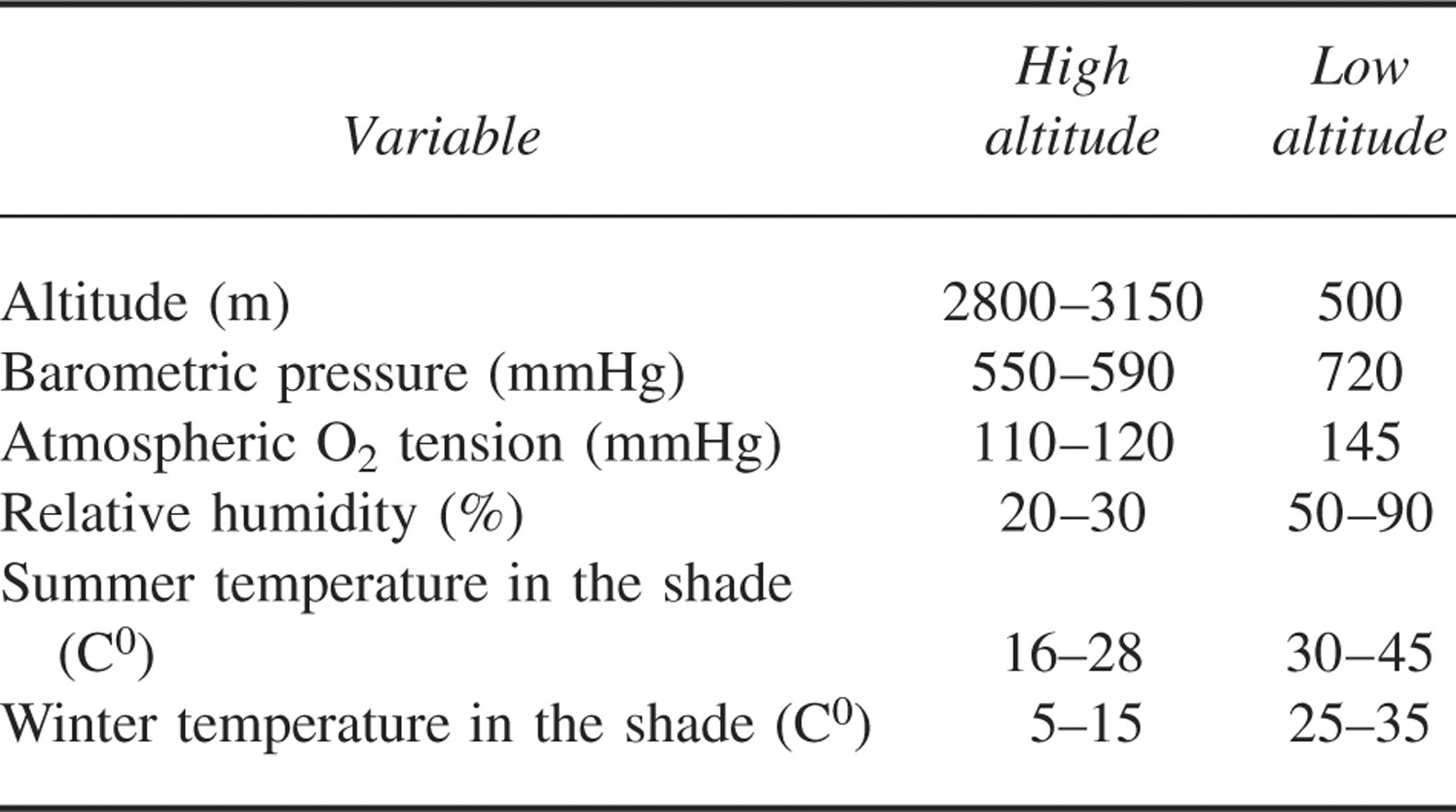
This study was conducted in rural high- and low-altitude areas of the Asser province in the southwestern part of Saudi Arabia. For high altitudes (2800–3150 m), the Alsoda village and the villages around Sabit Allia were selected. For low altitudes (≤500 m), the villages around Mohyel city were selected. Environmental data on these areas are shown in Table 1. 16 Health services to the areas involved in the study are provided by health centers run by qualified physicians who used 2 referral hospitals with good access roads. Potable drinking water and electricity were also available in these areas. The original occupation of the highlanders was farming, and the original occupation of the lowlanders was farming and sheep and goat breeding, but an increasing number of both high- and lowlanders now commute to nearby cities for work. Meat, chicken, and rice constitute the major dietary items for the people living in the 2 localities.
Comparison of study regions
The data presented in this paper were collected from 912 school children and adolescents aged 6–15 years born and living permanently at high altitudes (89% of total school-aged children and adolescents registered in the health centers at the high-altitude study area) and 972 school-aged children and adolescents of comparable ages born and living permanently at low altitudes (also 89% of total school children and adolescents registered in the health centers at the low-altitude study area).
The inclusion criteria for this study included Saudi school children and adolescents aged 6–15 years born and in permanent residence in the designated study areas and without pathologic conditions by clinical examination (eg, chronic renal, respiratory, cardiovascular, or gastrointestinal conditions). A total of 1917 children were seen, and 33 were excluded because they did not fulfill the criteria for inclusion in this study (11 at high altitudes and 22 at low altitudes).
All measurements and interviews were made in the health centers after obtaining approval from the College Medical Research Centre (CMRC) and the Health Affairs of Aseer Region and consent from the parents. This study was conducted from 1999 to 2000.
For each participant, age was calculated and recorded from his or her birth certificate at the time of the examination. Participants were divided according to their age into school children (<10 years of age) and adolescents (10–15 years of age).
To assess overweight and obesity, body weight was measured and recorded using an Avery Beam weighing scale (SECA, Hamburg, Germany) to the nearest 0.1 kg. Participants were weighed in their underwear and a correction of 0.1 kg was made for clothing. Standing height was measured and recorded to the nearest 0.5 cm with a stadiometer (SECA) without shoes.
A questionnaire was used for collecting other data. The questionnaire was completed by the attending physicians in the health centers. Parents were interviewed about family size, family income, level of education, and the common types of food consumed by the child. Family size included the father, number of wives, number of children, and number of dependents (eg, a grandfather or grandmother). Family income included income of the father and the mother per year in Saudi Riyals (SR) (1 U.S. dollar = 3.75 SR). Family income per person per year was then computed from the family income and family size (family income divided by family size) and was categorized into 3 levels: low, <3000 SR; moderate, 3000 to 12 000 SR; and high, >12 000 SR. Parental education was categorized into 5 levels: illiterate, primary school, intermediate school, secondary school, and university.
For school children aged <10 years, overweight and obesity was defined as >2 SD from the median weight for height of the World Health Organization (WHO)/ NCHS reference population. 17 This method is noninvasive and inexpensive, reflecting body weight relative to height, and thus more closely reflecting body fatness than other methods. Furthermore, the method is sensitive to current nutritional status and relatively independent of race and age in prepubescent children. For adolescents aged >10 years, overweight and obesity was defined as a BMI >85% according to age and gender-specific percentiles for BMI from the WHO/NCHS reference population, 17 because the weight-to-age index is considered uninformative or even misleading and the weight-to-height index changes dramatically with age and with maturational status.
Statistical Analysis
The collected data were compiled and fed into an IBM computer. The Statistical Package for Social Sciences version 10 (Chicago, IL) was used for statistical analysis. Descriptive data were presented as mean ± SD or percentage. The Student's t test and chi-square test were used to compare between means and percentages, respectively. The effects of the 2 indicators of SES of the parents on childhood overweight and obesity were studied separately. To avoid null cells, the comparisons were done between 2 levels. Parental education was categorized as illiterate or educated. Lower income per person per year was defined as <3000 SR (<800 U.S. dollars), and moderate-to-high income was defined as ≥3000 SR. The relationship between each potential risk factor and childhood overweight and obesity was estimated using the chi-square test. P values <.05 were considered significant.
In order to determine the effect of each risk factor on the development of childhood overweight and obesity, crude odd ratios (cORs) were derived using 2 × 2 tables and expressed with 95% CIs. A direct binary logistic regression analysis with the presence of childhood overweight and obesity as dependent and significant potential risk factors as covariates (ie, age, sex, parental income, and high-altitude birth and residence) was then performed to identify the independent risk factors for childhood overweight and obesity. 18
Results
The total number of school children and adolescents in this study at high and low altitudes was 912 and 972, respectively, with equal response rates of 89% at high and low altitudes. Table 2 shows the number of school children and adolescents by sex at high and low altitudes. Forty-seven percent of the boys and 53% of the girls in the sample were from high altitudes. The respective percentages in the sample from low altitudes were 46% and 54%. There were no significant differences between the percentages of boys and girls at the same altitudes or between boys and girls at high altitudes and their respective sexes at low altitude (χ2 = 0.25; P < .6). There were also no significant differences in the mean ages between boys and girls at the same altitude or between boys and girls at high altitudes and their respective groups at low altitudes. This was true for the total group and the 2 subgroups.
The prevalence of overweight and obesity by age (mean ± SD) and sex of Saudi high- and low-altitude school children and adolescents
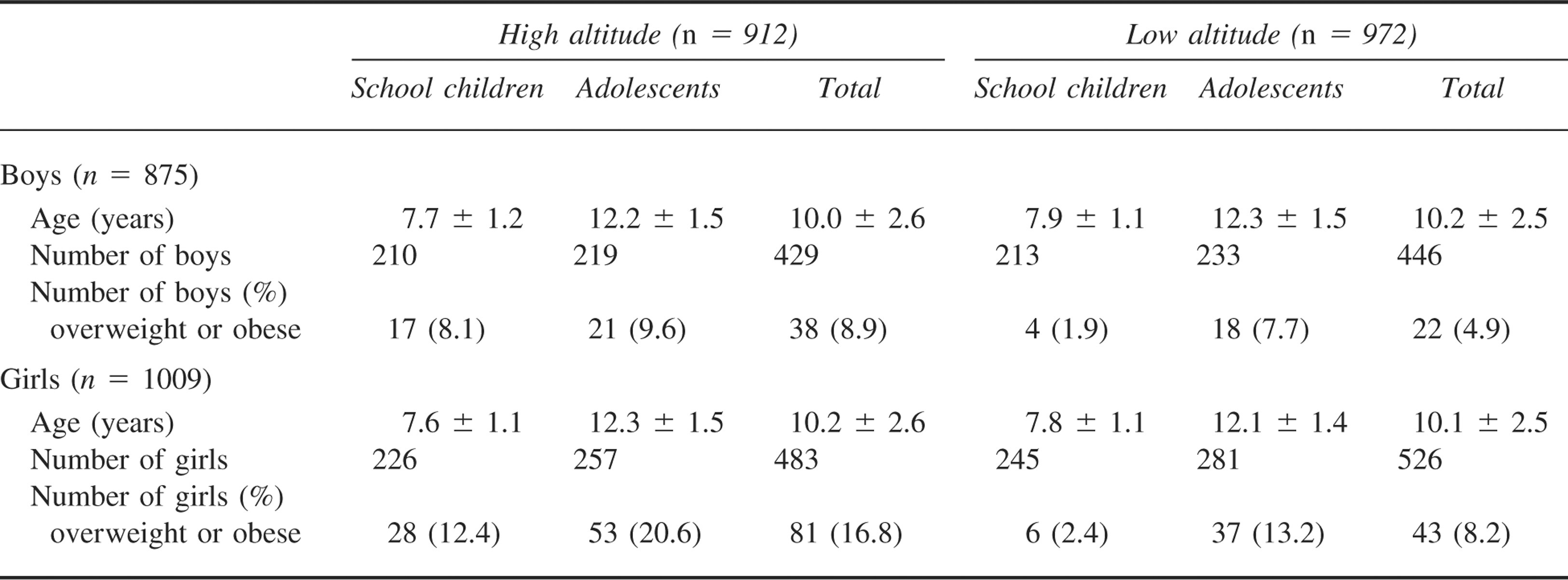
Table 2 shows the prevalence of overweight and obesity by age and sex. The overall prevalence of overweight and obesity at the 2 study sites was 10%. The prevalence of overweight and obesity was significantly higher among high-altitude school children and adolescents (13.1%) compared to low-altitude children and adolescents (6.7%; χ2 = 21.6; P < .0001). High-altitude birth and residence increased the risk for childhood overweight and obesity by 2.1 (95% CI, 1.5–2.9). In both high- and low-altitude school children and adolescents, overweight and obesity was significantly more common in girls than in boys (χ2 = 15.7; P < .0001). Female sex increased the risk for childhood overweight and obesity by approximately 2 (cOR 1.9 [95% CI, 1.4–2.6]). Among high- and low-altitude boys and girls, the prevalence of overweight and obesity increased from 6.2% in school children to 13% in adolescents (χ2 = 25.2; P < .0001) and those aged ≥10 years were more at risk of developing childhood overweight and obesity (cOR 2.3 [95% CI, 1.6–3.2]).
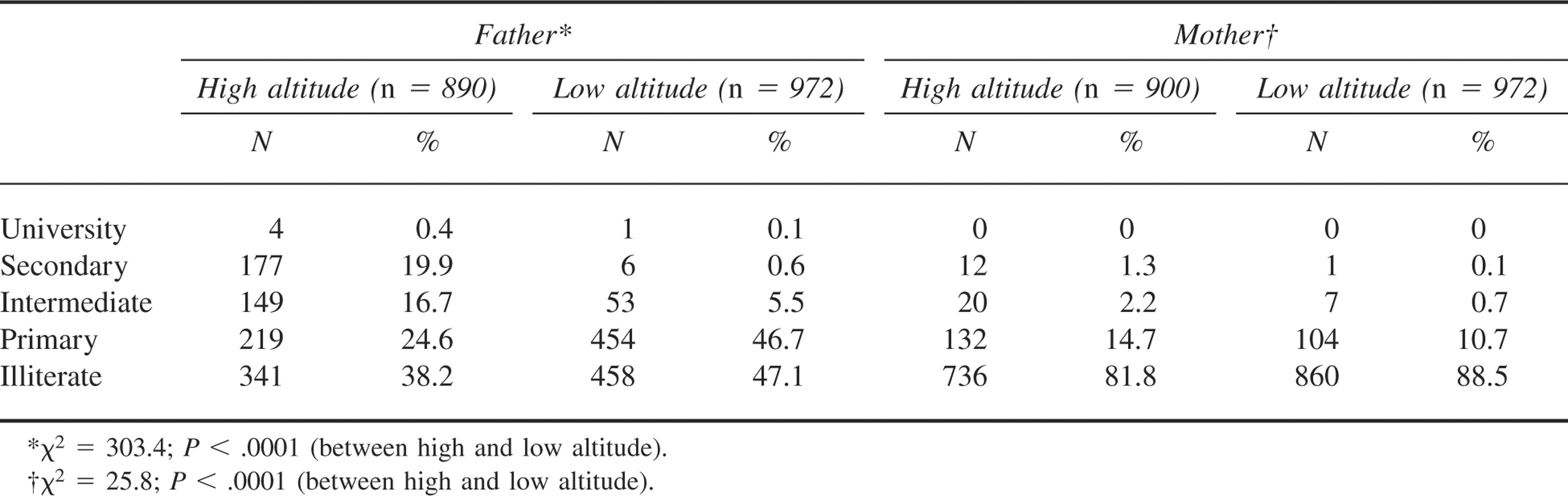
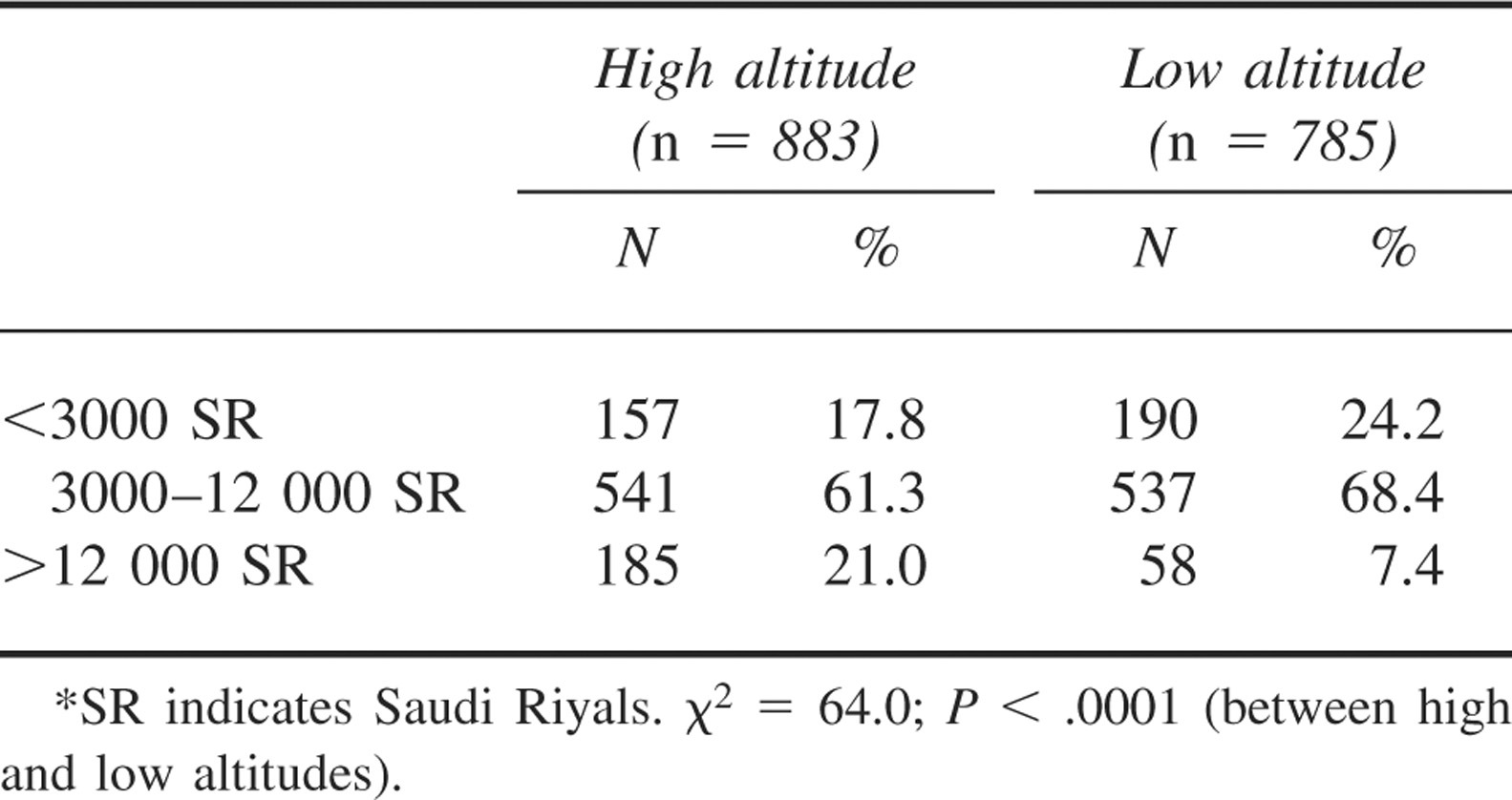
Parental education and family income per person per year were used as indicators for SES. Table 3 shows the number and percentage of school children and adolescents born to parents in the 5 educational categories. At both high and low altitudes, there were significantly more school children and adolescents born to educated fathers (57.1%) than to illiterate ones (42.9%; χ2 = 14.7; P < .0001). An exactly opposite trend was observed when the percentages of school children and adolescents born to educated (14.7%) and illiterate mothers (85.3%) were compared (χ2 = 16.7; P < .0001). None of the mothers interviewed at high and low altitudes had a university education, and only a very small proportion (0.3%) of high- and low-altitude school children and adolescents were born to fathers who finished university. The mean ± SD family income per person per year of high-altitude parents (8296.1 ± 7317.9 SR) was significantly higher than that of lowland parents (5706.7 ± 4314.6 SR; P < .0001). Approximately 82% of high-altitude school children and adolescents were born to parents with a family income per person per year ≥3000 SR compared to 75% of low-altitude school children and adolescents. The remaining percentages (17.8% and 24.2%, respectively) were born to parents with a family income per person per year <3000 SR (χ2 =10.4; P < .001) (Table 4).
The number and percentage of school children and adolescents born to parents in the 5 educational categories
The number and percentage of school children and adolescents born to parents in the 3 levels of family income/ person/year*
There were no significant associations between childhood overweight and obesity and the education of the father and the mother. The proportion of overweight and obese school children and adolescents born to illiterate and educated fathers and mothers were 9.4% and 10.1% for fathers and 9.9% and 9.1% for mothers, respectively (χ2 = 0.24; P < .3 for fathers and χ2 = 0.19; P < .4 for mothers). The percentage of overweight and obese was significantly higher among school children and adolescents born to parents with a moderate-to-high family income (11.7%) than those born to parents with a low family income (4%; χ2 = 17.9; P < .0001). Moderate-to-high parental income increased the risk for childhood overweight and obesity by more than 3 (cOR 3.2 [95% CI, 1.6–2.6]).
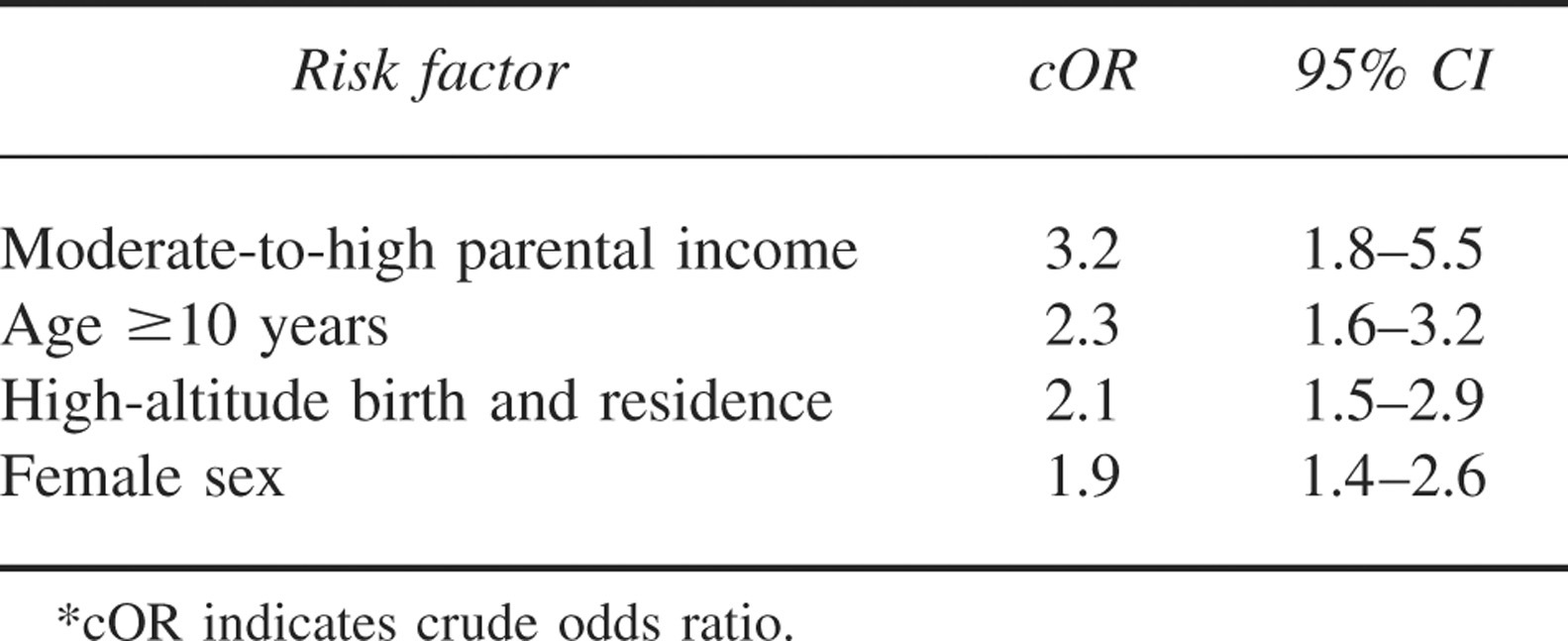
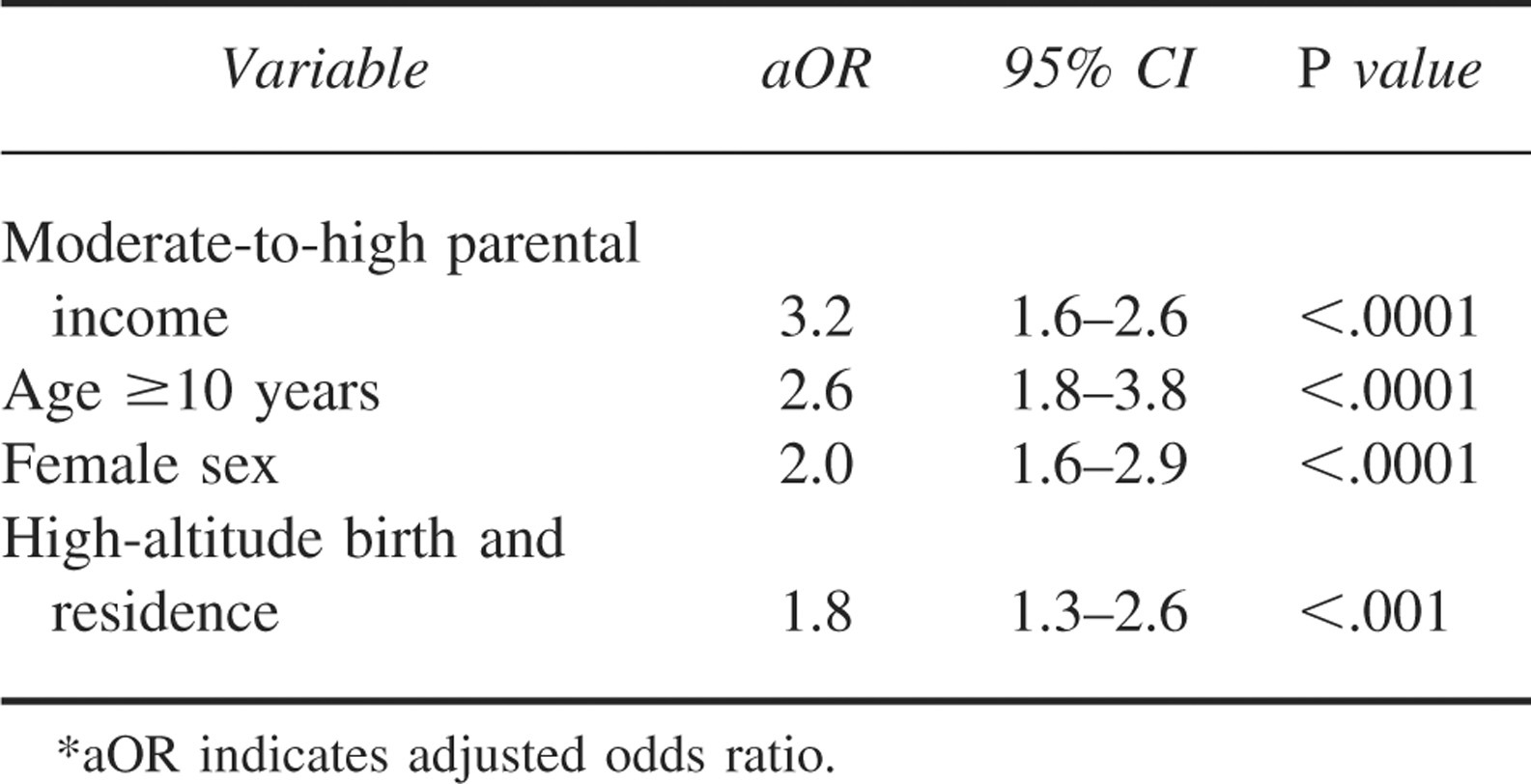
Table 5 summarizes the significant risk factors for childhood overweight and obesity in the Aseer region of Southwestern Saudi Arabia. The risk factors included moderate-to-high parental income, age ≥10 years, high-altitude birth and residence, and female sex. A binary logistic regression with childhood overweight and obesity as dependent and the above-mentioned potential risk factors as covariates revealed moderate-to-high parental income, age ≥10 years, female sex, and high-altitude birth and residence as the significant independent predictors of childhood overweight and obesity (adjusted OR 3.2 [95% CI, 1.6–2.6], 2.6 [95% CI, 1.8–3.8], 2.0 [95% CI, 1.6–2.9], and 1.8 [95% CI, 1.3–2.6]), respectively (Table 6).
Crude odds ratios and 95% confidence intervals of significant sociobiological factors in developing childhood overweight and obesity in the Aseer region of southwestern Saudi Arabia*
Multivariate logistic regression model: adjusted odds ratios and 95% confidence intervals of sociobiologic factors in developing childhood overweight and obesity in Aseer region of southwestern Saudi Arabia*
Discussion
The present study identified significant risk factors for childhood overweight and obesity in southwestern Saudi Arabia. These included moderate-to-high parental income, age ≥10 years, high-altitude birth and residence, and female sex.
Of the 2 indicators for SES, family income per person per year was found to be positively and significantly associated with childhood overweight and obesity. This relationship between family income and childhood overweight and obesity is consistent with previous reports from developing countries2,4 but at variance with studies from developed countries. 19 –21 A lack of a significant relationship between parental education and childhood overweight and obesity was also at variance with reports from developing countries that observed a positive significant relationship 2 and developed countries that observed a negative significant relationship. 20
The mechanism by which the SES of parents influences childhood overweight and obesity is poorly understood. It has been suggested that lower SES promotes higher energy intake that results in obesity in developed countries. 22 However, very few studies have been conducted in developing countries, and the general impression is that lower SES causes lower energy intake and lower incidence of obesity and higher SES causes higher energy intake and, therefore, higher incidence of obesity, but this has not yet been verified by research work. In Saudi Arabia, families with a high income own at least 1 car. Their children are driven to school in cars, watch television, use computers, and play electronic games for hours. All these lead to a more sedentary life and, therefore, a higher incidence of childhood overweight and obesity.
The current study also showed that overweight and obesity increased between the age groups 6–<10 years and 10–15 years in both sexes and at both altitudes and that adolescents were more at risk of developing childhood overweight and obesity. This is in line with a previous report from the WHO 23 that indicated that during adolescence, children displayed an increase in body fat often associated with irregular meals, changing food habits, and inactivity. 23
The present study also demonstrated that the prevalence of overweight and obesity was lower in boys than in girls, a finding consistent with previous studies5,6 but at variance with other investigators who observed an opposite trend4,24,25 or no relationship. 26 Sex differences in the prevalence of overweight and obesity were thought to be due to cultural factors. In some places, it was acceptable for boys to carry excess weight but not girls, 24 while in other places the reverse was acceptable, 27 indicating a possible culturally influenced gender bias. In Saudi Arabia, however, the difference may be again related to difference in physical activity levels between boys and girls. For social and protective reasons, a girl is detained in the house while a boy is free to play with his brothers and friends outdoors.
That the prevalence of obesity was significantly greater among highland children and adolescents as compared to their counterparts living at low altitudes is surprising in view of the fact that high-altitude hypoxia is known to cause retarded body growth. 28 Earlier studies in different parts of the world, including the Andes and Himalaya mountains, have shown that children living at high altitudes are shorter and more linear than their counterparts living at low altitudes 28 and that obesity is a rarity among high-altitude children worldwide.14,29 The difference was attributed to the growth retarding effect of high-altitude hypoxia as well as racial, dietary, and economic factors, 28 although recent investigators argued that socioeconomic conditions are more important than high-altitude hypoxia. 30
However, retarded body growth did not appear to be a feature of high-altitude children in tropical regions.31,32 Studies on native inhabitants of the Simen mountains of Ethiopia 31 and the Sarwat mountains of Saudi Arabia 32 have shown that high-altitude children are taller and heavier than low-altitude children and that obesity was more common among high-altitude adults as compared to low-altitude adults. 33 In Ethiopa and Saudi Arabia, the difference in weight and height between high- and low-altitude children was related to the higher incidence of malaria and other tropical infections in low-altitude children. 31 –33
In this study, we eliminated the racial and dietary factors by using low-altitude children and adolescents of the same ethnic background and dietary habits as controls, and when all other sociobiologic factors were controlled for in the multivariate analysis, high altitude was a significant and independent factor.
It was not clear how a high-altitude environment influences childhood overweight and obesity. However, previous studies on the same population have shown that the mean birth weight was significantly lower at high altitudes than at low altitudes.34,35 The difference was attributed to the intrauterine hypoxia to which the fetus is subjected secondarily to maternal hypoxia at high altitudes.34,35 Infants with a low birth weight have a greater proportion of fat relative to lean body tissue. 36 Therefore, in effect, they are obese if obesity is to be defined as excess of body fat. Also, there is increasing evidence that infants with a low birth weight have a particularly increased risk of developing obesity later in childhood. 37 It follows, therefore, that one of the mechanisms by which high altitude influences childhood overweight and obesity may be related to differences in birth weight between high- and low-altitude school children and adolescents.
Another mechanism could be related to differences in physical activity levels between high- and low-altitude children. Again, a study on this population in adults has shown that strenuous physical activity was significantly and inversely associated with obesity at both high and low altitudes, 38 and a strong association of physical activity and obesity is well recognized, even in school children, worldwide. 39 –41 Because of the cold weather at high altitudes and the topography of the area with its ups and downs, high-altitude children and adolescents tend to spend most of their time indoors watching television and playing computer games. On the other hand, low-altitude children and adolescents tend to be more active when compared with their high-altitude counterparts. They spend more time outdoors helping on farms and rearing their goats and sheep.
In conclusion, the present study identified risk factors for childhood overweight and obesity in Saudi Arabia, a developing country. Among these risk factors, high altitude was a significant and independent factor. It has been speculated that the mechanism by which high altitude influences childhood overweight and obesity could be related to differences in birth weight and physical activity levels between high- and low-altitude children and adolescents. A limitation of this study was that we could not obtain data on birth weight and physical activity. In addition, genetic factors, such as obesity in parents, were not examined. The findings in this respect call for future studies to verify these hypotheses and to look for other possible mechanisms by which a high-altitude environment influences childhood overweight and obesity. Such future studies will help to establish programs to prevent and control overweight and obesity in children living at high altitudes.
Footnotes
Acknowledgments
The author would like to thank all the medical and administrative staff working in the health centers involved in this study during the field work.