
Abstract
Objective
Avalanches pose a life-threatening risk to participants of outdoor winter activities. Determining the causes of death in avalanche fatalities can aid rescue and resuscitation strategies and hopefully improve survival.
Methods
The study population included all avalanche fatalities in Utah from the 1989–90 to 2005–06 winter seasons. The Utah Avalanche Center and Medical Examiner records were reviewed to identify accident circumstances, autopsy findings, and causes of death.
Results
Fifty-six avalanche deaths were identified during the study period. Most deaths occurred while participating in recreational backcountry activities; 85.7% of deaths were due to asphyxiation, 8.9% were due to a combination of asphyxiation and trauma, and 5.4% were due to trauma alone. Head injuries were frequent in those killed solely by trauma.
Conclusions
Most avalanche deaths in Utah result from asphyxia. Therefore, most victims are alive in the postavalanche period and have the potential for live recovery. Rescue strategies that employ rapid recovery as well as techniques that prolong survival while buried provide the best means of improving outcome.
Introduction
Avalanches can turn mountain travel into a dangerous endeavor. They are usually triggered by the victims themselves and travel at speeds of 90 to 120 km/h (56 to 81 mph) with tremendous force. 1 A person caught in an avalanche is tumbled within a sea of large snow blocks and may encounter trees, rocks, or cliff bands during the descent. When the victim and slide come to a halt, the body is often deposited under many meters of high-density snow making movement and breathing difficult or impossible. Even a small avalanche can cause death by asphyxiation under less than a meter of snow.
In addition to traveling with a partner, backcountry travelers should carry an avalanche transceiver (beacon), a probe, and a shovel to perform an immediate rescue if a fellow party member is buried. Live recovery is relatively high (92%) within the first 15 minutes after burial. 2 However, survival chances plummet to 30% after 35 minutes as asphyxiation occurs. Failing to carry proper safety gear or delaying rescue will significantly decrease survival. 3
Apart from the standard rescue gear, other self-rescue strategies may also improve survival chances. When an avalanche begins to slow, the victim should attempt to expand his chest to prevent snow from compressing the thorax. The victim should also try to clear an air pocket, or a space in front of the mouth, to assist in respiration. Under ideal situations, this may extend the period of survivability to approximately 90 minutes. Thereafter, chance of survival is extremely low as death occurs from asphyxiation or hypothermia. Asphyxiation during avalanche burial occurs because expired gases (containing approximately 5% carbon dioxide and 16% oxygen) are rebreathed. Carbon dioxide displaces oxygen in the alveoli according to the alveolar gas equation, PAO2 = PIO2 − (PACO2/R). Asphyxiation death ultimately results from a combination of hypercapnia and hypoxia.
Evaluating the causes of death in avalanche fatalities is of utmost importance in order to guide approaches to avalanche rescue and resuscitation. If traumatic mechanisms are responsible for many avalanche deaths, then prevention measures yield the primary means of reducing fatalities. If, however, most victims survive the initial slide but then quickly die from asphyxiation, swift rescue efforts and devices that either prevent burial or prolong burial survival time are additional measures to reduce deaths. A limited number of studies 4 –9 have specifically examined causes of death during avalanche burial, and 4 studies 10 –13 have examined it peripherally. All include small numbers and only 4 8 –11 are published in the English literature.
This study was a descriptive retrospective case review that examined the causes of death in avalanche fatalities in Utah from the winter seasons of 1989–90 to 2005– 06. By examining this information, we hope to direct advances in avalanche medicine and provide strategies for improving survival.
Methods
The Utah Avalanche Center (UAC) is a federal agency within the Forest Service division of the US Department of Agriculture. It is the primary avalanche organization in Utah. The UAC conducts daily snow and climate analysis and issues daily avalanche forecasts during the winter season for the Wasatch and Uinta Mountain Ranges. The center investigates all avalanche accidents that occur in Utah by studying the snow pack that contributed to the avalanche as well as reporting on human and safety factors. The UAC is the only organization that performs this service in Utah.
Historical records from the UAC were reviewed for all avalanche fatalities during the winter seasons of 1989–90 to 2005–06. Medical examiner case files and autopsy reports were reviewed. Demographic information, type of autopsy (external vs internal), injuries, and cause of death were recorded. An internal autopsy is defined as a full examination of internal and external organs. An external autopsy is defined as a visual and tactile examination of the exterior body. The medical examiner's decision to perform an external or internal autopsy was based on circumstances of death, potential legal liability, and appearance on external examination. The default is typically an internal examination. The medical examiner's stated cause of death was based on circumstances surrounding the death as well as physical evidence revealed during the autopsy.
The study was reviewed and approved by the University of Utah Institutional Review Board. Descriptive statistical techniques performed by SPSS 14.0 (SPSS Inc., Chicago, IL) were used to analyze data. The Fisher Exact test was used to determine whether traumatic mechanisms were related to snowmobiler deaths vs other activities. Tests were 2-sided with alpha set at 0.05.
Results
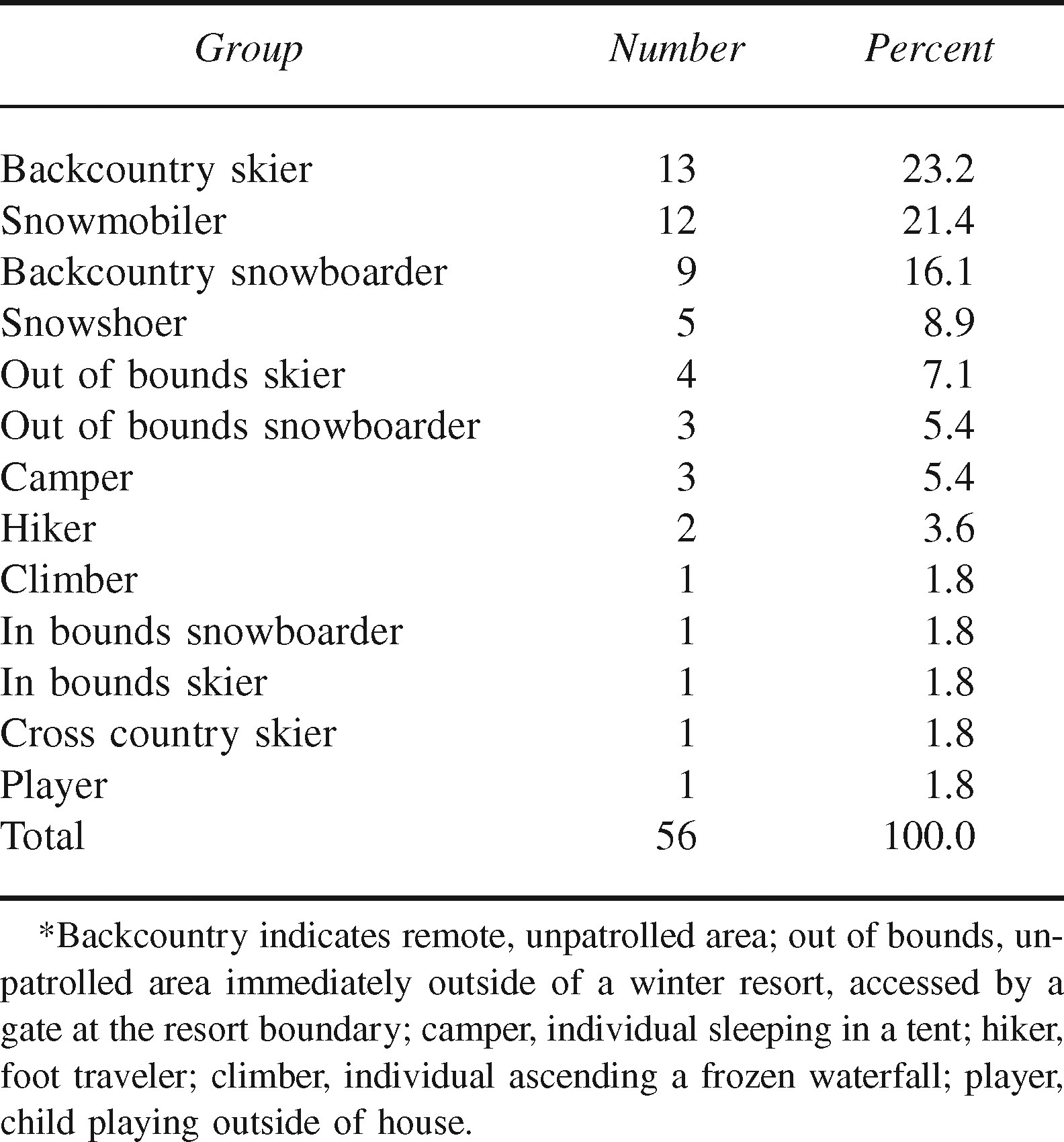
Fifty-six fatalities occurred as a result of an avalanche in Utah during the study period. The mean age was 31 (SD 10) with a range of 7 to 59. Fifty-three victims were male, and 3 were female. The activities undertaken by the victims during the fatality are listed in Table 1. All except 1 fatality occurred during winter recreational activities. The exception was 1 child who was playing outside a house when the avalanche occurred on the slope above.
Activities of victims of fatal avalanche accidents in Utah: 1989–90 to 2005–06 winter seasons*
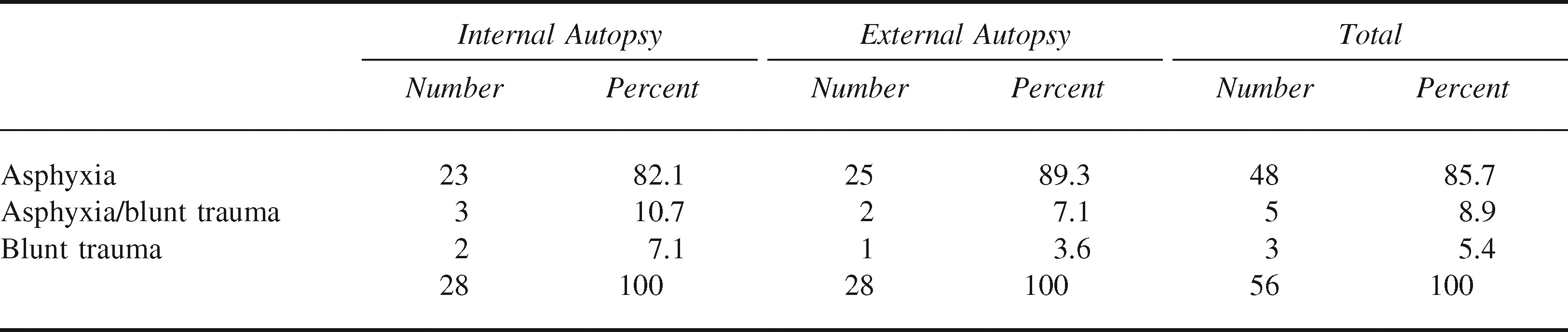
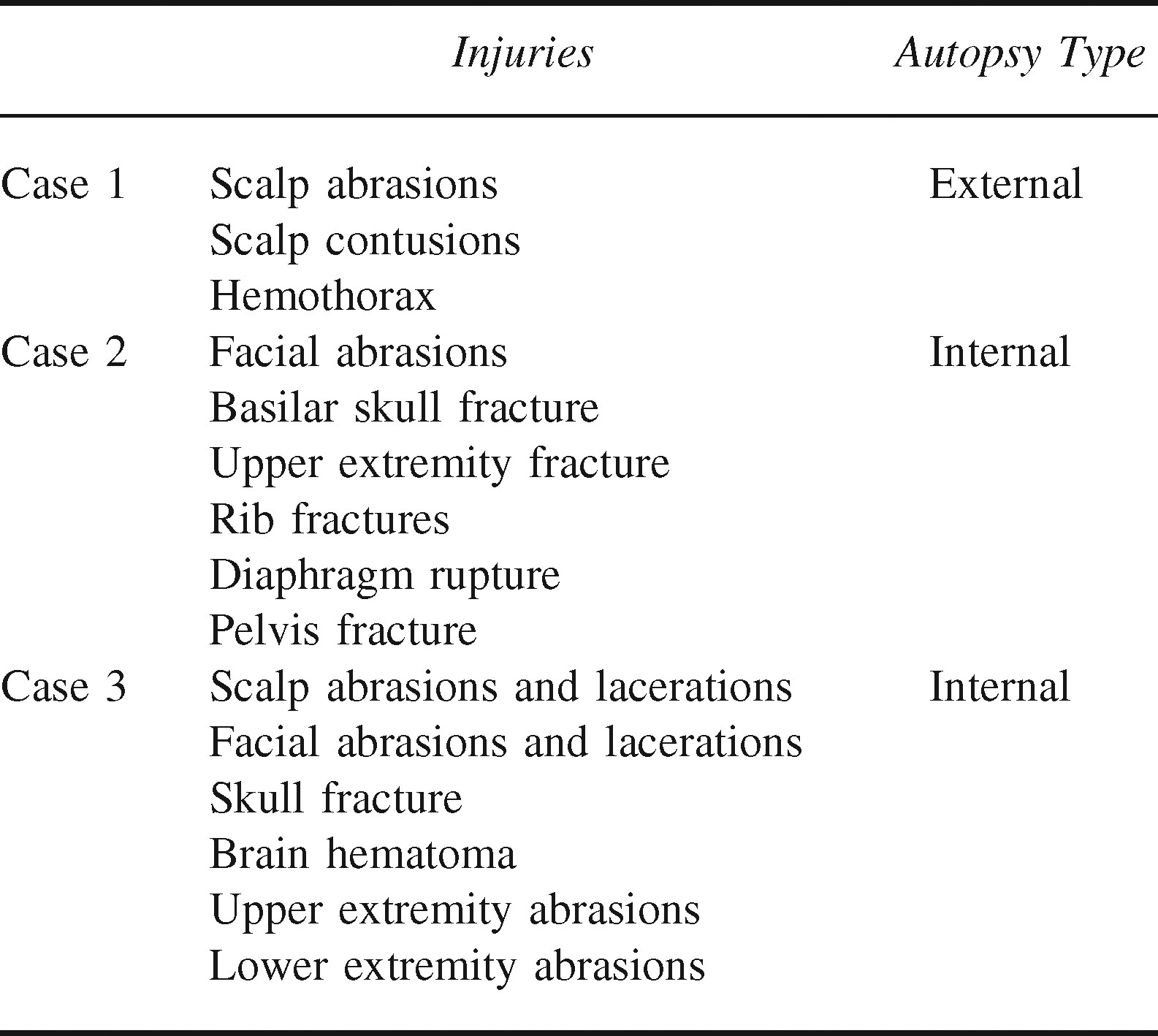
A medical examiner review and autopsy was conducted in all cases. Fifty percent of the victims received an internal autopsy whereas the other 50% received an external autopsy. The primary causes of death are described in Table 2. Asphyxia or a combination of asphyxia and trauma accounted for the majority of fatalities. Blunt trauma as the sole mechanism accounted for only a small percentage. One death, which the medical examiner attributed to asphyxia and substance intoxication, was merged into the asphyxia category. Cocaine metabolites and ethanol were found in the bloodstream of this victim. Three deaths were attributed to traumatic injuries alone. These injuries are described in Table 3.
Primary cause of death
Injuries discovered on autopsy in traumatic avalanche deaths in Utah: 1989–90 to 2005–06 winter seasons
The number of traumatic deaths among snowmobilers was compared with that of backcountry travelers not using snowmobiles. There was no association between using a machine-powered vehicle and death caused by trauma (P = 1.00).
Discussion
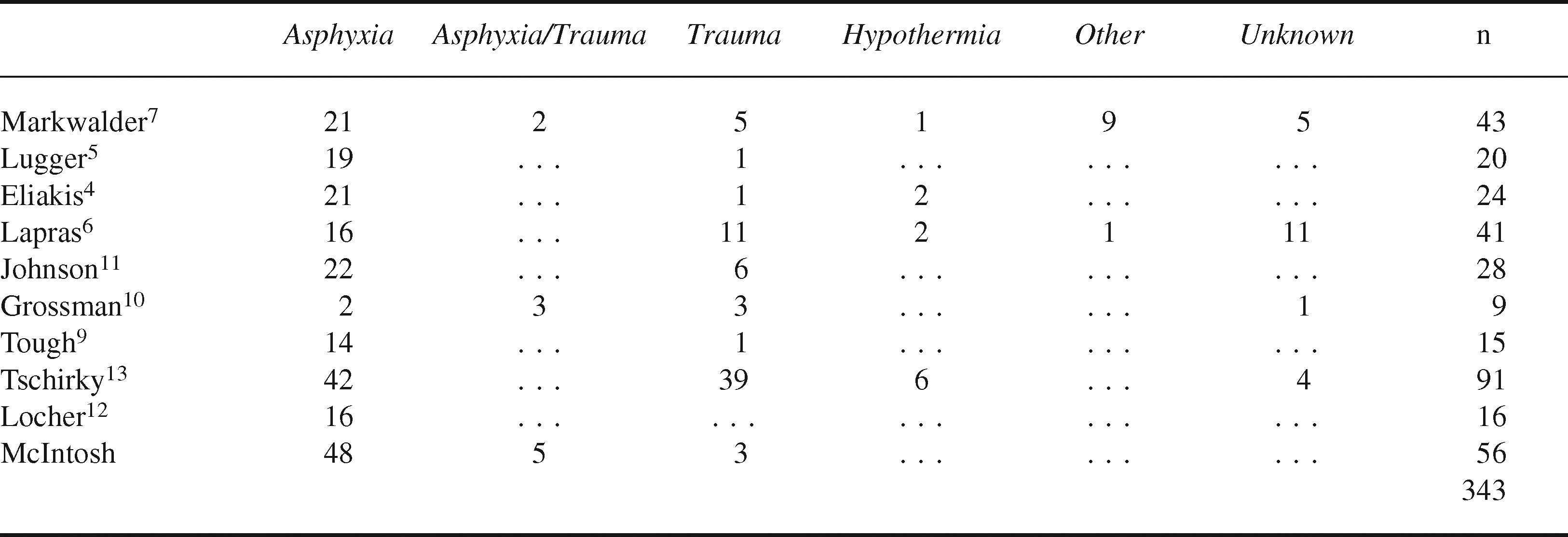
The majority of avalanche victims in our series died as a result of asphyxiation. Blunt trauma was responsible for only a small fraction of fatalities. These results are consistent with the limited number of past studies on the subject. This study represents the largest series on avalanche fatalities in the English literature and the second largest to date. The results of prior studies as well as this study are summarized in Table 4. Variability in cause of death may occur geographically. For instance, data may be collected in terrain that is predominately above tree line or in backcountry areas that lack cliff bands or other rocky hazards, resulting in a higher proportion of asphyxiation deaths. These geographical differences create local avalanche patterns and shape mortality characteristics.
Summary of research on cause of death in avalanche fatalities
Based on this information, most avalanche victims remain alive directly after burial and have the potential for a successful live recovery. Delayed or ineffective efforts will shorten the available time window for rescue. This reinforces the dogma that all parties must be capable of performing swift rescue if an avalanche burial occurs. However, in Utah only about 45% of all backcountry users carry the minimum recommended safety equipment. 14
The results also demonstrate the potential for improving survival via air pocket devices. One artificial breathing device (AvaLung, Black Diamond Equipment, Ltd, Salt Lake City, UT) appears to work well under controlled circumstances. 15 Air from the surrounding snowpack is inhaled through a 1-way valve seated in a housing on the chest. Exhaled gases travel through a separate 1-way expiratory valve around to the back of the victim. Rebreathing of expired gases is therefore limited. This delays the hypercapnia and hypoxia that cause asphyxiation during avalanche burial.16,17
Preliminary studies under controlled conditions 15 and anecdotal reports of avalanche accidents 18 suggest that this artificial breathing device can prolong survival. Adequate oxygenation and ventilation can be maintained for up to 60 minutes during full burial in snow. If all expired gases are experimentally removed from the snowpack, there is sufficient oxygen to allow adequate ventilation and oxygenation for up to 90 minutes. 19
The success of this artificial breathing device as well as other avalanche rescue methods assumes, however, that trauma from the slide has not rendered the victim incapacitated or fatally injured. In order to benefit from the device, the victim must insert the breathing apparatus in the mouth before or during the slide and hold it in place throughout the slide and burial. These are challenging tasks during an avalanche. Furthermore, the thorax must have adequate space to expand. It is unknown whether the majority of asphyxia deaths are caused by hypoxia or thoracic compression. 7 An air pocket device would be useless in compression asphyxia. Although further experience will reveal whether the device will actually reduce mortality, all advances that have the potential to increase avalanche survival are encouraging.
The traumatic mechanisms causing death in this study were quite severe. All three fatalities attributed solely to blunt trauma had evidence of head injury. Other potentially fatal injuries were present in these cases as well. Two had internal pathologic evidence of head injury, and the other had external evidence (no internal autopsy was conducted). Severe thoracic injuries predominated in the 3 victims as well. It is very unlikely that immediate rescue or devices would have changed these outcomes. Traumatic brain injury may compromise the ability of the buried avalanche victim to breathe adequately (assuming the victim has not been killed outright). A case has been made 11 to wear helmets during backcountry activities. Our results support this conclusion.
Hypothermia was recorded as a cause of death in past research4,6,7,13 but not in our study. Core body cooling rates during avalanche burial range between 0.7°C to 3.0°C per hour.12,17,20 Assuming a preavalanche core body temperature of 37°C, the victim would have to be buried for more than 3 hours before life-threatening arrhythmias and hypoventilation would initiate at approximately 28°C. 21 In the vast majority of avalanche cases, the victim will succumb to asphyxia before this time threshhold. 2 For this reason, hypothermia is not normally considered a primary cause of death in avalanche victims.
Although prevention should always be the best mitigator of avalanche risk, avalanches can occur even in presumably safe conditions. If caught in a slide, most victims are killed in the immediately ensuing time period rather than by the avalanche itself. In these instances, rapid rescue by nearby parties poses the best chance for surviving an avalanche. Organized rescue attempts involving dogs, helicopters, or large search parties will likely be unsuccessful because of the time needed to mobilize such resources. Self-reliance continues to be the most important aspect of survival in the mountains.
Limitations
The primary limitation of this study was its retrospective character. By the nature of medical examiner investigations, not all victims received the same type of autopsy and not all autopsies were performed by the same examiner. Traumatic injuries could have been missed on victims receiving only an external examination. Despite these limitations, a large number of victims in this series received internal autopsies. In addition, autopsy examination is the only method of obtaining information in certain cases as many avalanche victims are not evaluated in a hospital.
Conclusions
Asphyxia is the main cause of death in most avalanche accidents. Blunt trauma will kill fewer victims. Although prevention remains the overall goal of safety in the mountains, avalanches can and still occur even when proceeding with caution. If an avalanche occurs, rapid rescue and possibly air pocket devices offer extra survival potential for those buried.
Footnotes
Acknowledgments
The authors thank Dr Todd Grey, Utah Chief Medical Examiner, and the staff of the Utah State Office of the Medical Examiner for their assistance with this project. Special thanks to the staff of the Utah Avalanche Center for their cooperation in assisting with historical records. Dr Grissom has served as a consultant for Black Diamond, Ltd., manufacturer of the AvaLung. He does not own any part of Black Diamond or the AvaLung.