
Abstract
The cardiovascular system participates in both blood pressure (BP) and temperature regulation. As a result, salt ingestion creates conflict between BP and temperature homeostasis, as vasodilatation that would promptly lower the BP would simultaneously increase cutaneous blood flow, thereby accelerating heat loss. If temperature homeostasis has precedence over blood pressure homeostasis, as postulated by the thermoregulatory-vascular remodeling (TVR) hypothesis, then in order to minimize heat loss, BP remains elevated following salt ingestion until the kidneys excrete the excess salt. A case of amlodipine overdose offered an opportunity to test a corollary of the TVR hypothesis: vasodilators should cause a drop in body temperature and/or an increase in the metabolic rate. Following the ingestion of 1000 mg of amlodipine, the temperature and BP of a single patient were monitored during the initial 36 hours and during the 13th day of hospitalization. The BP dropped markedly between the fifth and seventh hours postingestion, but then rose steadily and normalized by 28 hours postingestion. The temperature was normal at 7 hours postingestion, declined gradually between the seventh and 26th hours postingestion, stabilized between the 26th and 31st hours postingestion, then began to rise. During this case of amlodipine overdose, a modest temperature decline lagged behind a marked BP decline. As the BP rose, the temperature also rose, but lagged behind the BP increases. These findings suggest that there is a relationship between BP and temperature and are consistent with the TVR hypothesis.
Introduction
Approximately 95% of all hypertensive patients have essential hypertension, and no etiology can be determined for the elevated blood pressure (BP). Numerous explanations for the development of essential hypertension have been proposed. These include abnormalities in the renin-angiotensin-aldosterone system,1,2 alterations in the levels of circulating catecholamines,1,3 abnormalities in the excretion of kallikrein, 4 insulin resistance, 5 hyperuricemia, 6 and genetic mutations in the enzymes that regulate the activity of sodium channels and mineralocorticoids in the kidney tubules.1,7–9 Nonetheless, when essential hypertension develops, it remains unclear as to why the body's multiple regulatory mechanisms fail to maintain BP homeostasis. The recently postulated thermoregulatory-vascular remodeling (TVR) hypothesis addresses this dilemma. 10 We report a case of amlodipine overdose 11 that offered an opportunity to test one of the corollaries of the TVR hypothesis.
TVR hypothesis
The cardiovascular system participates in both BP and temperature regulation. As a result, sodium chloride ingestion causes conflict between the goals of BP and temperature homeostasis. The TVR hypothesis postulates that temperature homeostasis has precedence over BP homeostasis. While prompt vasodilatation would lower the BP following an ingestion of sodium chloride, vasodilatation that included the cutaneous circulation would accelerate heat loss, thereby lowering the core body temperature. The BP remains elevated following an ingestion of sodium chloride until the kidneys excrete the excess sodium chloride, and BP homeostasis is gradually restored. However, vascular remodeling occurs during the periods of BP elevation. 12 Vascular remodeling irreversibly increases peripheral resistance. 12 Each episode of sodium chloride ingestion causes an incremental increase in peripheral resistance. Numerous incremental increases in peripheral resistance ultimately raise the baseline BP, with the outcome being essential hypertension.
One of the predictions of the TVR hypothesis is that antihypertensive medications that are vasodilators will accelerate heat loss due to increased blood flow to the cutaneous circulation. As a result, 1 of 3 possible temperature-related outcomes will occur: either the core body temperature will decrease, there will be a compensatory increase in the metabolic rate, or a combination of these 2 phenomena will occur.
Case report
A 40-year-old woman attempted suicide by ingesting 1000 mg of amlodipine (100 tablets of amlodipine, each of which contained 10 mg of amlodipine). About 5 hours after ingestion, her husband brought her to an emergency department for treatment. Her initial BP was 100/60 mm Hg. She was treated with ondansetron intravenously because she was nauseated. The BP subsequently fell to 88/76 mm Hg and she became somnolent. A dopamine infusion was begun. Eighty minutes after presentation for emergency care, her BP dropped to 58/38 mm Hg. She was intubated, an orogastric tube was placed, and charcoal was administered. Insulin was administered intravenously because studies support the administration of insulin while maintaining normal blood glucose levels in the treatment of poisoning with calcium channel blockers. 13 The rate of the dopamine infusion was increased, and norepinephrine and dextrose infusions were initiated. Calcium gluconate and calcium chloride were administered in order to overcome calcium-channel antagonism by using supratherapeutic doses of calcium salts, 14 and the patient was transported to a second emergency department. She arrived at the second emergency department less than 2 hours after presenting to the first emergency department. In the second emergency department, the initial temperature was 36.7°C (orally), the BP was 42/32 mm Hg, and the pulse was 74 beats per minute. As she continued to receive medical treatment, her BP improved. She was admitted to the hospital and eventually discharged.
The patient's medical record was reviewed after she was discharged from the hospital. BP readings were available beginning 5 hours postingestion, when the patient presented to the first emergency department. Temperature readings were available beginning 7 hours postingestion, when the patient arrived at the second emergency department. Thereafter, simultaneous temperature and BP readings were available at 1- to 4-hour intervals.
The figure graphically depicts the auscultatory BP and temperature measurements during the initial 36 hours following the ingestion of 1000 mg of amlodipine and provides BP and temperature data during the 13th hospital day following the overdose. All the temperature readings were obtained with an oral thermometer. The BP readings are expressed as the mean arterial pressure. The patient had a low BP 5 hours post amlodipine overdose. Comparing this initial BP with the BP readings on the thirteenth hospital day, the initial BP was close to the patient's baseline BP. The BP dropped markedly between the fifth and seventh hours postingestion, but then the BP rose steadily and normalized by 28 hours postingestion. The temperature was normal at 7 hours postingestion, declined gradually between the seventh and 26th hours post ingestion, stabilized between the 26th and 31st hours postingestion, then began to rise. On the 13th hospital day, both the BP and the temperature fluctuated, but both of these vital signs were presumably within the normal range for the patient at this stage of her medical treatment.
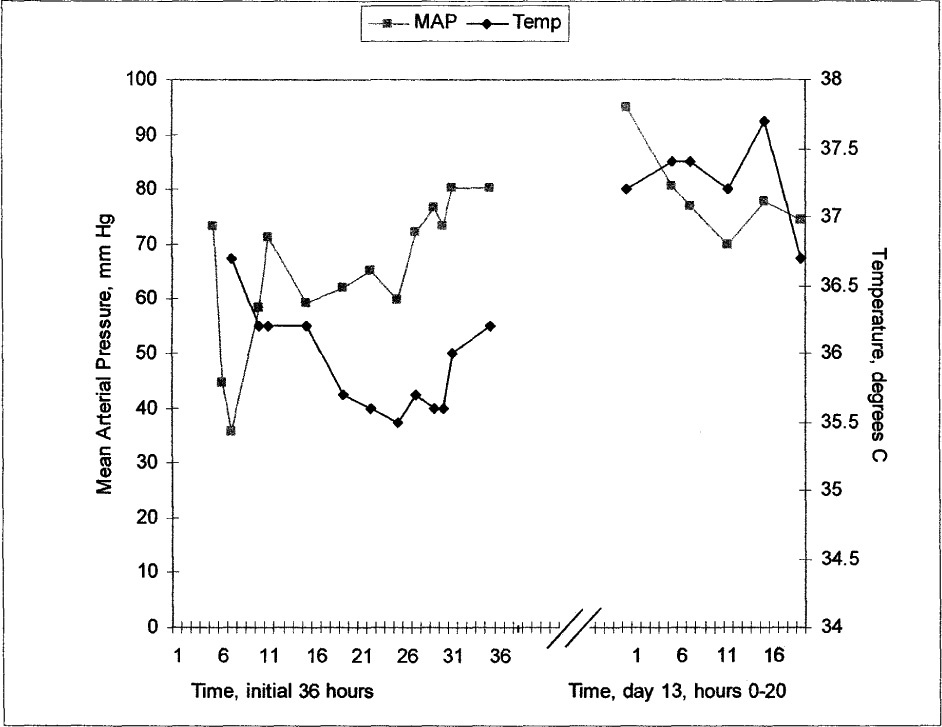
Mean arterial pressure (MAP) and oral temperature during the initial 36 hours post amlodipine ingestion and on day 13.
Discussion
In terms of being a test case for the TVR hypothesis, this report has several limitations. For one thing, this case was not an experiment, and there was no systematic attempt to collect relevant data. As a result, there are many gaps in the medical record: there are no BP data for the initial 5 hours, the collection of temperature data begins even later, and there are no simultaneous BP and temperature readings for hours on end. Another limitation is that none of the temperatures were obtained rectally. Consequently, the temperature readings can only be considered approximations of the core temperature. In addition, there is no information regarding the metabolic rate. Finally, environmental factors such as ambient temperature and the amount of clothing being worn would be expected to influence body temperature. It is an additional limitation of this report that the patient's temperature was recorded in different areas of the hospital with possibly differing air temperatures and relative humidities, and the amount of clothing and blankets covering her were unspecified.
Despite these limitations, the findings of this case of amlodipine overdose are instructive. This case suggests that there is a relationship between BP and temperature. During the initial 36 hours postingestion, the changes in temperature paralleled the BP changes, albeit with a delay of several hours. When the BP declined, there was a delayed drop in the temperature. When the BP rose, there was a delayed increase in the temperature. These BP and temperature data are consistent with the predictions of the TVR hypothesis.
Further research is needed in order to better understand the interrelationship between temperature regulation and BP regulation. Studies in which volunteers have their BP lowered or raised in a controlled environmental setting, while at the same time their core temperature and metabolic rate are monitored, would help shed light on this issue.