
Abstract
Objective
To test the hypothesis that acclimatization to high altitude results in an improvement of the ventilatory threshold (VT).
Methods
Eight lowlanders underwent cardiopulmonary exercise testing with a cycle ergometer to determine VT and peak oxygen uptake (V
Results
V
Conclusions
Individuals who are sedentary or not participating in regular physical training appear to require a longer period of acclimatization than trained athletes. With the increasing numbers participating in high-altitude trekking and charity climbs of peaks, such as Mt. Kilimanjaro, this information has clinically significant practical implications for those leading or acting as medical advisors.
Introduction
Ventilatory threshold (VT) allows noninvasive assessment of a person's reliance on anaerobic energy production during exercise.1,2 The VT can be defined as the intensity of exercise at which aerobic energy production is supplemented by anaerobic energy systems. VT can be determined with cardiopulmonary exercise (CPX) testing, which is an integrated test of cardiac, respiratory, metabolic and skeletal function during exercise. 1
Changes in maximal oxygen consumption (V
The aim of this study was to assess the response to exposure to high altitude in a group of healthy, untrained trekkers by examining changes in the VT. We hypothesized that VT would improve following partial acclimatization.
Materials and methods
Participants
Eight healthy white Europeans (7 men, 1 woman, mean age 39.5 years (1 standard deviation [SD], 14 years); mean height 178.3 [9.1] cm) were studied. All were nonsmokers, normotensive, taking no dietary supplements, and on no medication, other than antimalarial prophylaxis (atovaquone proguanil, Malarone®). Participants were physically active but not involved in athletic or fitness training on a weekly basis and therefore regarded as untrained. All participants resided at elevations between 50 and 150 m, they had no recent exposure to high altitudes, and were familiar with cycle ergometer– based exercise tests. [The Research and Ethics Committee of the South Birmingham Health Authority granted approval for these studies, and participants gave their written and informed consent.] Participants completed 3 exercise tests: the first in Coventry, United Kingdom (80 m elevation) approximately 4 weeks before departure and the second in Leh, India (3500 m elevation).
Participants traveled to Leh, India, by airplane from the United Kingdom. The journey included a 24-hour stopover in Delhi (239 m elevation). The first measurements at high altitude were made 24 to 36 hours after arrival in Leh. Although the participants’ activity was not strictly controlled during the period between the first exercise tests in Leh and departure on the trek, participants only undertook short, nonstrenuous, sightseeing walks around Leh typical for a group of tourists at altitude. The whole group undertook the same trek from the fifth to ninth day at high altitude. This consisted of approximately 6 hours of trekking per day. During the trek, the group climbed to an altitude of 4770 m and remained above 3500 m at all times. Participants arrived back at the test location on the evening of the ninth day and were instructed to rest completely for that evening and the next day (10th) in order to reduce the effect of residual fatigue from the trek. The second measurements were obtained on the 11th and 12th days after the participants’ initial arrival at Leh, at the same location used for the first altitude test. Barometric pressures were 741 mmHg in Coventry and 486 mmHg in Leh during the first tests and 491 mmHg in Leh during the second tests.
Exercise Tests
Exercise testing was performed using our Alticycle™ cycle ergometer
4
(custom built by the Birmingham Medical Research Expeditionary Society). Participants rested for 0.5 hours before each test and then exercised gently for 5 minutes at 50W to warm up. Participants maintained a cadence rate of 55 pedal revolutions per minute throughout each test. Starting loads for each subject were estimated to produce a test lasting approximately 10 minutes.
5
The load was increased by 20W increments per minute up to volitional exhaustion. Expired gas was analyzed breath by breath using a Cosmed K4b
2
portable metabolic cart (Cosmed, Rome, Italy) for oxygen uptake, end-tidal CO2 and O2 and minute volume (VE) (turbine flow meter). Arterial oxygen saturation was measured using an Ohmeda Biox 3740 Pulse Oximeter (Datex Instrumentarium, Helsinki, Finland). The VT was identified by an independent assessor using the ventilatory equivalent method (VE/V
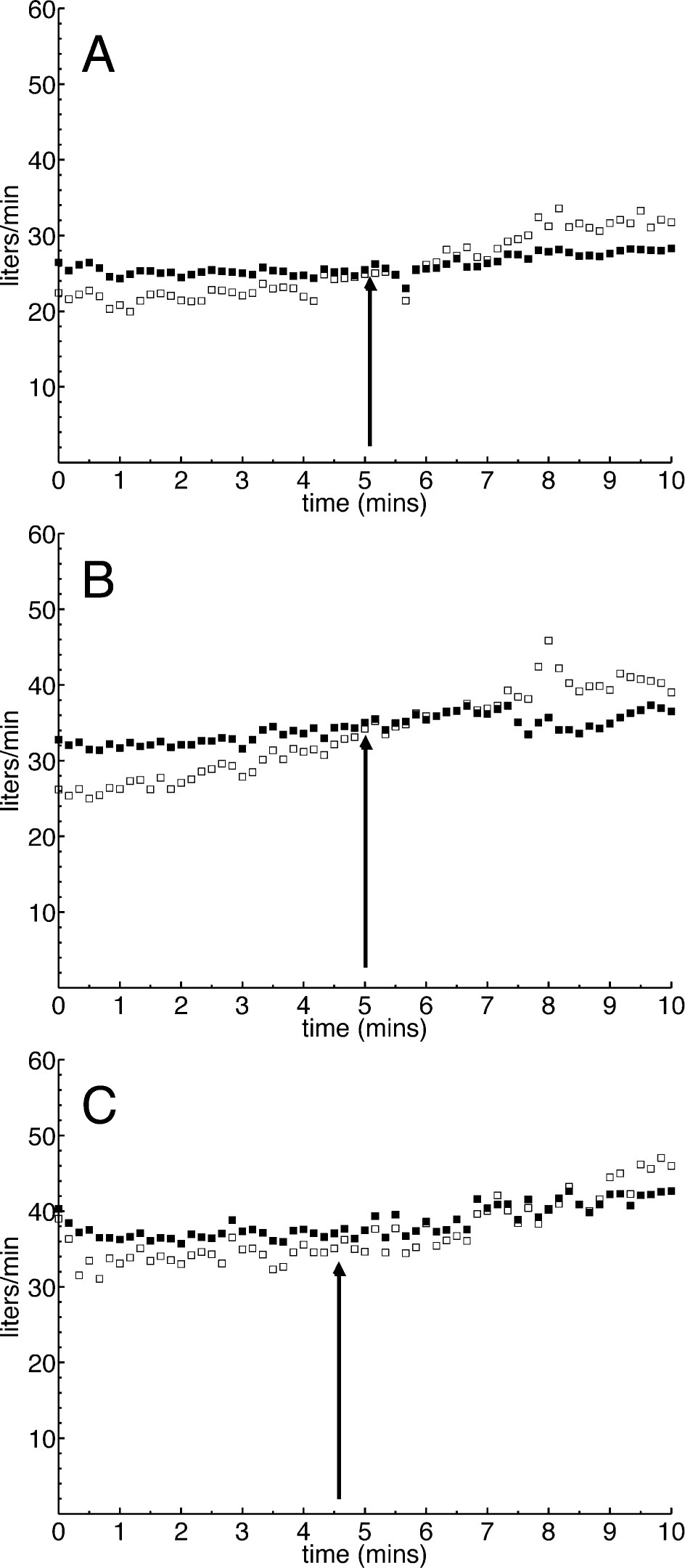
Example plot for one subject of the estimation of the ventilatory threshold using the ventilatory equivalent method.
Altitude Sickness
Throughout their stay at high altitude, participants completed morning and evening Lake Louise questionnaires, 7 which were assessed by the expedition doctor. Acute mountain sickness (AMS) was defined as a Lake Louise score of 4 or greater with accompanying headache.
Statistical Analysis
Respiratory data were collected continuously by logging it to the purpose written K4b 2 software. Oxygen saturation data were logged to a separate computer using a CED Power1401 (Cambridge Electronic Design, Cambridge, UK). Data are presented as mean (1SD). The significance of any change was assessed with a repeated measure analysis of variance (ANOVA), with differences located using Fishers Least Significant Difference test (SPSS version 11, SPSS Inc, Chicago, IL). Significance was accepted at P < .05.
Results
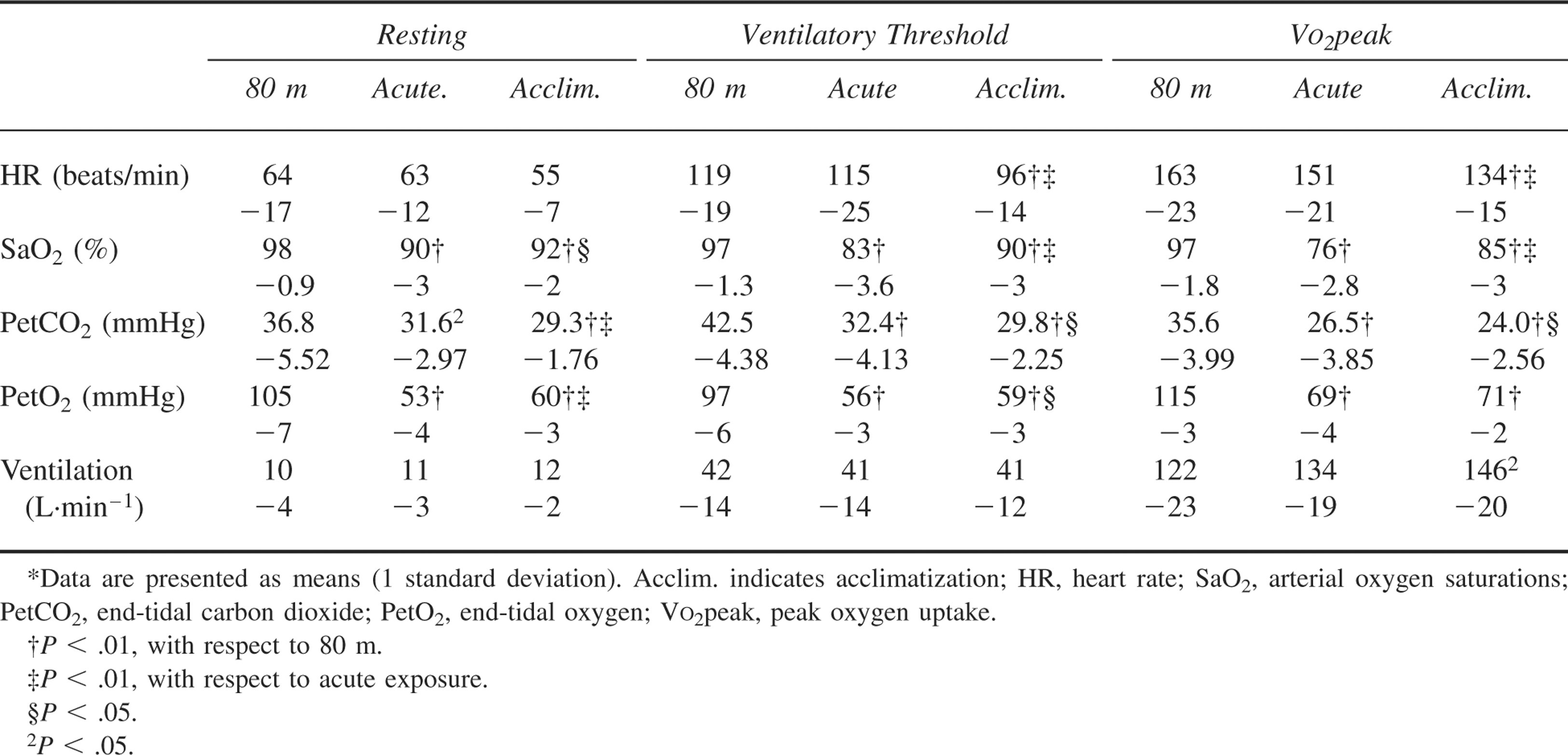
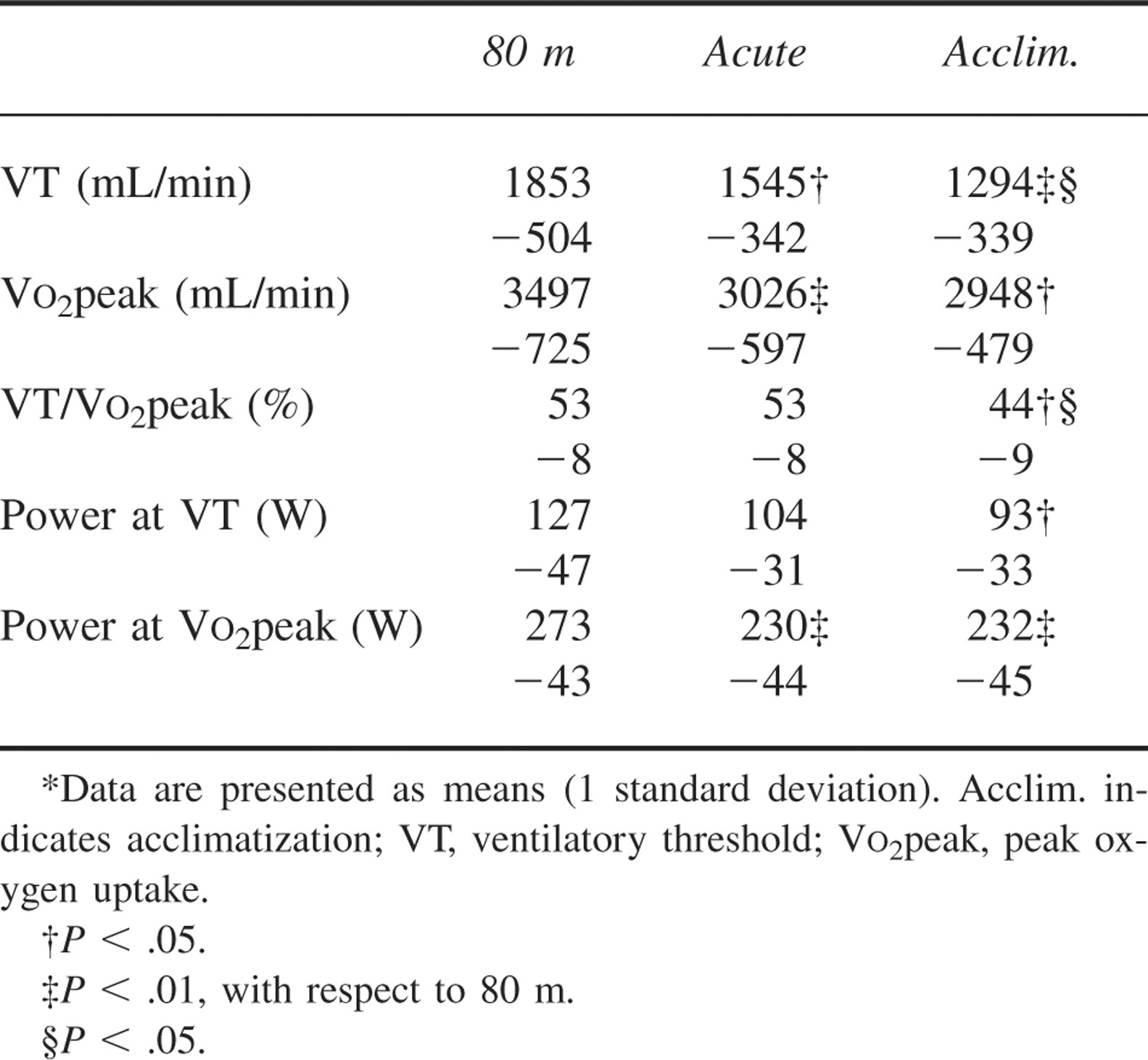
Cardiovascular changes are shown in Table 1. Changes in VO2 and power are displayed in Figures 2, 3, and 4 and Table 2. V
Comparison of physiological changes with altitude at different levels of exercise (n = 8)*
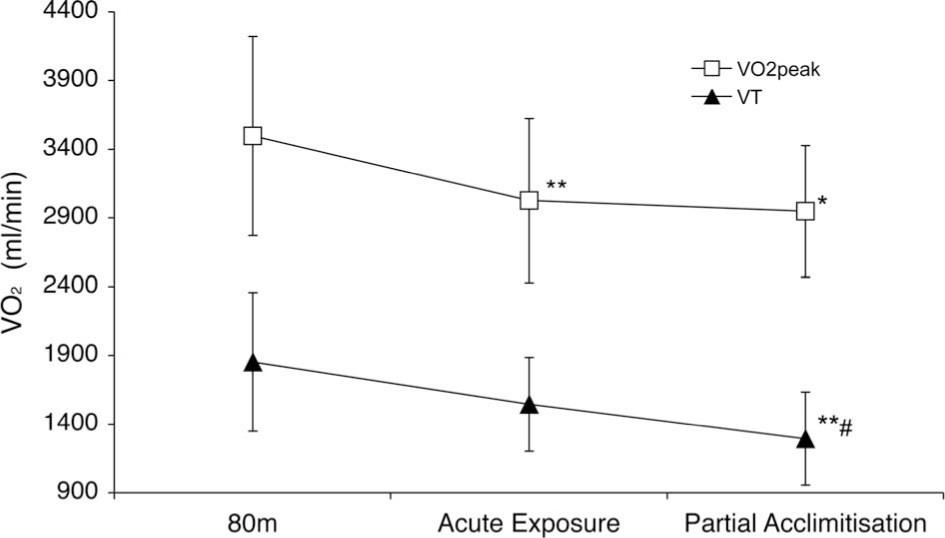
Changes in V
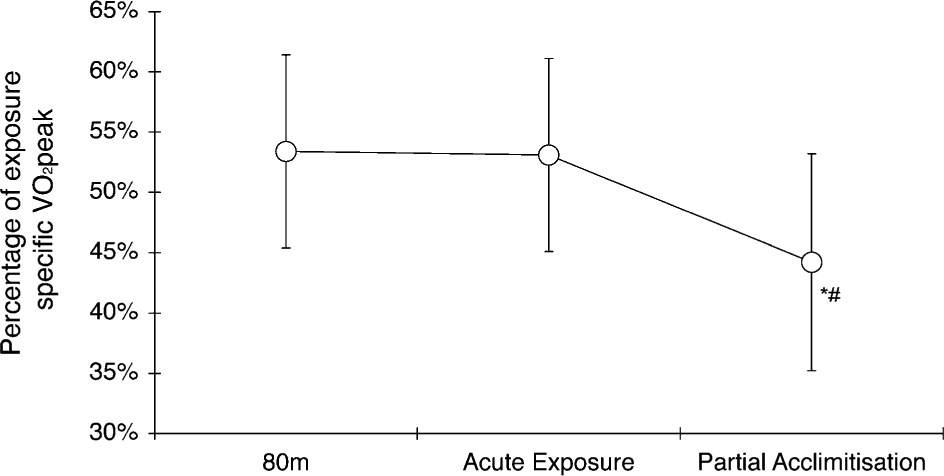
Changes in ratio V
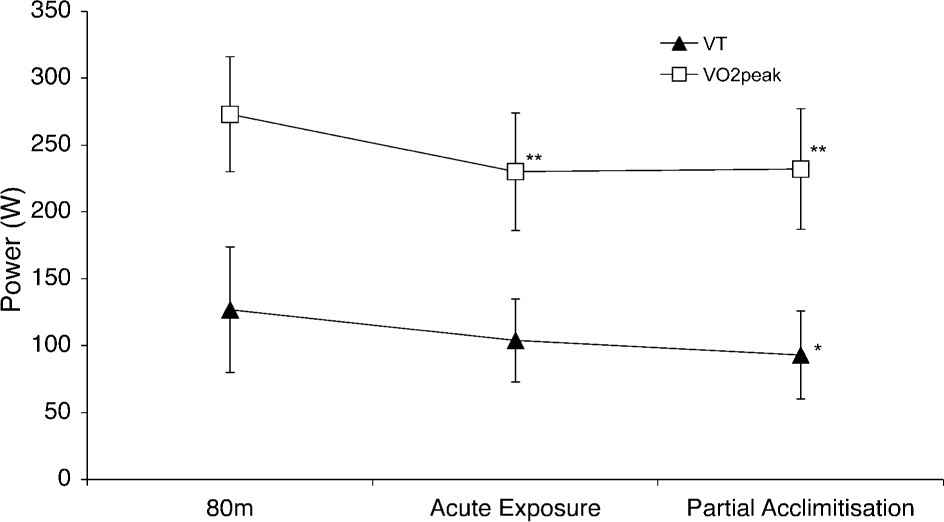
Changes in power output on cycle ergometer at the ventilatory threshold and at V
Comparison of changes in exercise performance with altitude at different levels of exercise (n = 8)*
Discussion
The main novel finding in this study is the observation of persistent reduction in VT with 12 days acclimatization, which contrasts with the improvement in VT seen in the study by Subudhi et al 3 performed in a physically fit population who regularly participated in endurance (cycle) exercise (greater than 6 hours per week). We believe a possible explanation may be in the individuals studied. Our study group was considerably older and less fit and, therefore, may more closely represent a tourist trekking group.
Our findings of reduced V
In contrast to Subudhi et al, 3 and in the interest of representing a real-life situation (sometimes termed ecological validity 10 ), we did not strictly control physical activity between tests. However, the 6 hours daily trekking from the fifth day was far in excess of normal physical activity for our participants, and all participants took part in the same trek as a group. As a result, we believe that the delay in acclimatization of VT in our participants is unlikely to be due to detraining, supported by our observation of unchanged body mass over the 12 days at high altitude.
We feel that both age and training status have important effects upon acclimatization of VT to high altitude. The lack of aerobic enzymatic, muscular adaptations, and central neuromuscular recruitment strategies of untrained individuals may be responsible for this difference. It is possible, therefore, that older, more sedentary individuals, as reported in our study, may require a longer time period for acclimatization of their VT to high altitude in comparison to physically fit males. However, another explanation may be that our untrained participants may be less affected by altitude than a trained group who may extract oxygen from the blood more efficiently and become more hypoxemic. Acclimatization would therefore lead to greater improvement in VT in athletes, because the initial acute exposure to altitude would cause a greater decrease in VT from baseline, and the athletes would have greater capacity for improvement of VT. Anecdotal reports suggest that athletic individuals may suffer worse AMS than nonathletes.11,12 Specific comparisons of athletes with untrained individuals have not been performed. One such anecdotal report is illustrated in observations made by Ravenhill 11 while working in Andean mines in the early 1900s: “There is in my experience no type of man of whom one can say he will or will not suffer from puna. Most of the cases I have instanced were young men to all appearances perfectly sound. Young strong and healthy men may be completely overcome. Stout plethoric individuals of the chronic bronchitic type may not even have a headache.”
The limitations of this study are as follows. First, we did not measure blood lactate. With exercise, individuals exposed to acute hypoxia demonstrate increased ventilation and blood lactate compared with the same exercise intensity during normoxic conditions. 13 However, during hypoxia, the VT occurs at a lower exercise intensity than the increase in blood lactate. 14 Similarly, blood lactate concentration at rest is greater at high altitudes than at sea level. This phenomenon only partially corrects after 3 to 5 weeks at high altitude. 15 It is, therefore, not surprising that a poor correlation between VT and lactate threshold has been demonstrated at high altitudes, 6 which may limit the interpretation of the VT as a noninvasive marker of anaerobic metabolism at altitude. Second, the lack of control in the activity levels during the altitude stay could result in potentially different detraining effects. Third, the subjects went on a long trek that could reduce the VT by reducing glycogen stores. 16
Our study raises more questions. Future research is required in a larger subject group to determine the time necessary for acclimatization of VT and the influence of activity level and exposure to higher altitudes during the acclimatization period. Studies should aim to determine the relationship between blood lactate changes and those seen with noninvasive measures, as in this study. Furthermore, a prospective study comparing acclimatization changes of the VT in athletes with untrained individuals may yield surprising results.