
Abstract
Families are traveling with their children in increasing frequency. Travel to Asia offers children many opportunities to learn about new cultures and history. It also offers the potential for exposure to numerous infectious agents not commonly encountered in the United States. Families must begin to prepare for travel to Asia weeks before departure. Children should be up to date on routine vaccinations. Appropriate education should be given on arthropod avoidance and malaria prophylaxis. Additional education and possible prophylaxis should be completed for other infectious agents frequently encountered in Asia. With appropriate pretrip immunizations and prophylaxis, children can travel to Asia with minimal risk of acquiring infection. This article provides general advice to assist providers with pretravel preparation and education of families traveling with children to Asia.
Introduction
Families are traveling with their children on an increasing basis, with an estimated 1.9 million children traveling overseas each year. 1 Many of these families participate in adventure vacations, traveling to developing countries to hike, bike, rock climb, and camp. Asia, a rapidly modernizing continent, has seen a 32% increase in vacation travelers in the last decade, most of whom visit the developing countries. 2 Travel to these areas presents opportunities for children to be exposed to new cultures, as well as to new infectious agents not commonly encountered in the developed world. Due to variable immunity, children are at higher risk of acquiring travel-related infections during trips than adults, requiring that appropriate medical preparation be initiated weeks before travel is to commence. This article will review the most common infectious agents children may encounter while traveling in Asia and the appropriate preventative measures to reduce the risk of illness during and after travel.
Routine health care
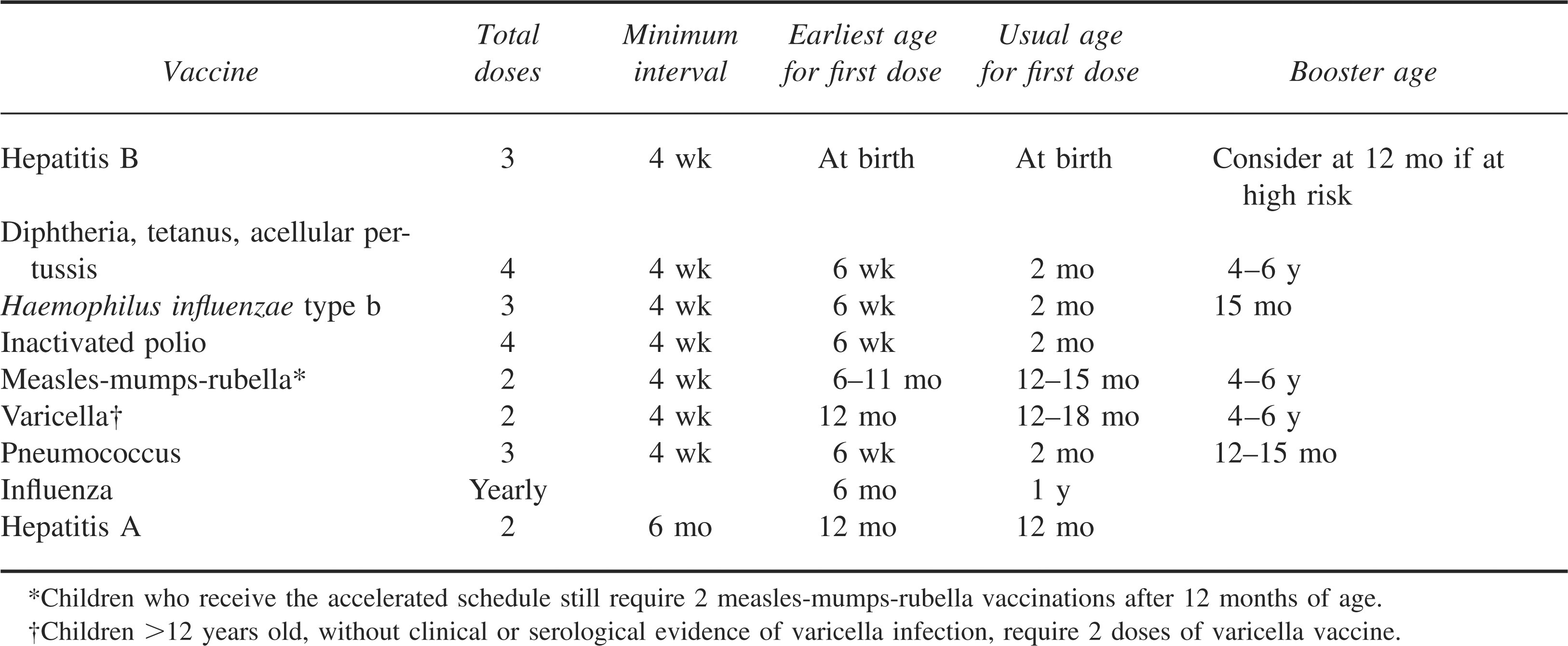
Children traveling to Asia should be up to date on all the routine childhood immunizations, including diphtheria, tetanus, pertussis, measles, mumps, rubella, polio, varicella, Haemophilus influenzae type b, pneumococcal, hepatitis B, and hepatitis A. Influenza vaccine should also be given when traveling during the peak transmission seasons. The most recent recommendations for immunizations according to the American Academy of Pediatrics (AAP) and Centers for Disease Control and Prevention (CDC) are summarized in Table 1. Diphtheria, tetanus, and acellular pertussis (DtaP); polio (IPV); hepatitis B (hep B); and H influenzae b (Hib) vaccines maybe initiated as early as 6 weeks of life and may be accelerated with vaccinations every 4 to 6 weeks in order to complete the full series before traveling to endemic areas. 3 The first dose of measles-mumps-rubella (MMR) vaccine may be given as early as 6 months of life if traveling to an area with an active outbreak. 3 Children receiving the early dose of MMR vaccine still require 2 MMR vaccinations, with the recommended timing of subsequent vaccinations being 12 months of age and again at 4 to 6 years of age to maximize immunity. 3 Varicella vaccine should be given prior to travel to all children older than 1 year. Children who are older than 12 years of age, with no clinical or serologic evidence of varicella infection, will require the first of a 2-shot series 4 to 8 weeks apart prior to departure to maximize immunity. 3
Routine immunizations
Hepatitis A
Hepatitis A (hep A) is the most common vaccine-preventable disease experienced by travelers to Asia. 4 The CDC has listed Asia as a high-prevalence area for exposure to hep A. 4 This is supported by recent data identifying travel to Asia as the source for 6% of all hep A infections in the United States. 5 Hepatitis A is an RNA picornovirus transmitted by fecal contamination of food and water. Infected children may present with fever, malaise, jaundice, anorexia, and nausea. Although adults are more likely to be symptomatic, children may also demonstrate a wide spectrum of symptoms. The disease is generally self-limited, lasting 7 to 87 days, and requires minimal supportive care and monitoring for resolution of the hepatitis. 6 The mortality rate is less than 1.5% in children. 6
Travelers to developing countries are at greater risk for infection due to poor food and water sanitation. Therefore, prevention of hep A is best achieved with close attention to good food and water hygiene. This is accomplished by drinking bottled water, or more conservatively water that is personally disinfected by boiling or by microfiltration combined with halide treatment, in addition to carefully selecting all foods. Fruits and vegetables should be cooked or carefully peeled. Street vendors’ food and beverages should be avoided due to increased likelihood of contamination. Additional prevention measures involve vaccination by the inactivated hep A virus vaccine, of which there are currently 2 licensed for use in the United States: Havrix (GlaxoSmithKline Biologicals) and Vaqta (Merck & Co Inc). This vaccination is now considered a routine childhood vaccination. Children traveling to Asia should receive the first shot in this 2-shot series a minimum of 6 weeks prior to travel. The first vaccination may be given as early as 1 year of age, with the second 6 to 12 months later. 7 If the departure is imminent, the child should receive both the vaccine and the immunoglobulin simultaneously to maximize protection. It is recommended that children younger than 1 year of age be evaluated for potential risk of virus exposure. If traveling to an endemic area and exposure to local water and food cannot be avoided, immunoglobulin should be administered at 0.02 mL/kg for those traveling less than 3 months and 0.06 mL/kg for those children traveling greater than 3 months. This will provide coverage during the duration of travel.
Hepatitis B
Hepatitis B (hep B) is caused by a DNA hepadnavirus transmitted by contaminated blood, blood products, saliva, and sexual activity with an infected partner and potentially via contact with the skin lesions of infected persons. Hepatitis B is endemic in Asia, with greater than 8% of the population infected with chronic hep B. 8 Disease presentation in children includes a spectrum of symptoms ranging from subacute illness with nonspecific complaints (eg, anorexia, nausea, malaise), to clinical hepatitis that includes jaundice, to, most severely, fulminant and fatal hepatitis. Children have a higher risk for developing chronic hep B infection, with 90% of infants, 25 to 50% of 1- to 5-year-old children, and 6 to 10% of older children developing chronic hep B after an acute infection. 9 Of those children who become chronically infected, 25% will develop hepatocellular carcinoma, cirrhosis, or chronic liver disease. 9
Prevention is best accomplished with completion of the vaccination series. There are 2 licensed recombinant vaccines available in the United States: Energix (SmithKline Beecham) and Recombivax (Merck). Vaccination for hep B has been routine for children in the United States since 1991. 10 For children who have missed their routine vaccinations, it may be given on the schedule of 0, 1, and 6 months or an accelerated schedule of 0, 1, and 2 months to accomplish full immunization prior to travel in high-risk areas, such as Asia. If the accelerated schedule is used, a fourth dose should be given at 12 months.
Typhoid
Typhoid fever is caused by the bacterium Salmonella typhi and transmitted via the fecal-oral route. The infection lasts 7 to 14 days with nonspecific complaints of fever, chills, malaise, headache, dry cough, myalgia, abdominal discomfort, and occasionally mental status changes. There are documented cases of more severe complications, such as gastrointestinal bleeding, intestinal perforation, and encephalopathy, but these are rare. Asia is considered a high-risk area for exposure to S typhi, with 22 million new cases reported each year. 7 Although it can be treated with oral antibiotics, in some areas of Vietnam, India, and Pakistan, there has been an increasing emergence of antibiotic-resistant strains of S typhi. 5 Treatment of these resistant strains is increasingly difficult, and thus it is recommended that travelers who plan to visit high-risk areas consider immunization. Although vaccination demonstrates an efficacy rate of only 70%, this provides substantial protection and can be further improved with the addition of strict food and water hygiene. 5
There are 2 types of vaccinations: oral Ty21a (Vivotif Berna) and the parenteral purified Vi polysaccharide typhoid vaccine Typhim VI (Pasteur Merieux Connaught). The oral Ty21a vaccine is a live attenuated vaccine that can be given to children as young as 6 years of age. 5 The child takes one capsule by mouth, 1 hour before or 2 hours after a meal, every other day for a total of 4 doses. A booster dose is needed every 5 years. 5 The Vi capsular vaccine requires a single injection and can be given to children older than 2 years of age. 5 A booster dose is required every 2 years. Vaccinations should be given at least 1 week before travel for the greatest protection.
Malaria
Malaria is endemic in tropical countries of Asia and found in almost all Asian countries. 11 Plasmodium vivax, P falciparum, and P malariae are all found in parts of Asia. 10 It is a mosquito-transmitted, blood-borne parasitic infection. The incubation period is typically 1 to 4 weeks, with many cases initially presenting with minimal symptoms. 10 Children have elevated levels of parasitemia. 11 They may present with paroxysmal fever, nausea, vomiting, diarrhea, cough, arthralgias, and abdominal and back pain. Children have an increased risk of severe complications, such as shock, seizures, coma, and death, making prevention of the infection vital. There are approximately 300 to 500 million new cases worldwide, with 1.5 to 2.7 million deaths annually. 12
Travelers to malaria-endemic countries should be counseled on prevention. The primary means of protection is mosquito avoidance, with a reduction in outdoor activity at dawn and dusk (times of increased mosquito activity). Lodging should be equipped with screens and air conditioning to decrease mosquito exposure. 11 Travelers should wear long pants and long-sleeved shirts to decrease the skin surface area available for a mosquito to find a blood meal. Clothing and equipment should be treated with permethrin, a mosquito insecticide. Mosquito netting, used over sleeping quarters, should be impregnated with permethrin to decrease contact with mosquitoes while sleeping. Additionally, the insect repellant diethyltoluamide (DEET) should be used on all exposed skin surfaces. Twenty to 35% DEET may be used safely on children 2 months of age and older. 13 Higher percentages of DEET, used in excess, have been associated with dermatitis, bullae formation, skin necrosis, and scarring in children. Toxic encephalopathy has also been documented in a small number of children who used elevated levels of DEET, likely due to the increased absorption associated with their large body surface area. 13 For improved safety, DEET should not be applied around the mouth or on the hands in order to reduce the risk of accidental consumption. Finally, DEET should be applied over sunscreen or lotion for the first morning application. 13 Sunscreen will often require more frequent application than DEET, and thus the sunscreen may be applied over DEET later in the day without affecting the performance of DEET or sunscreen.
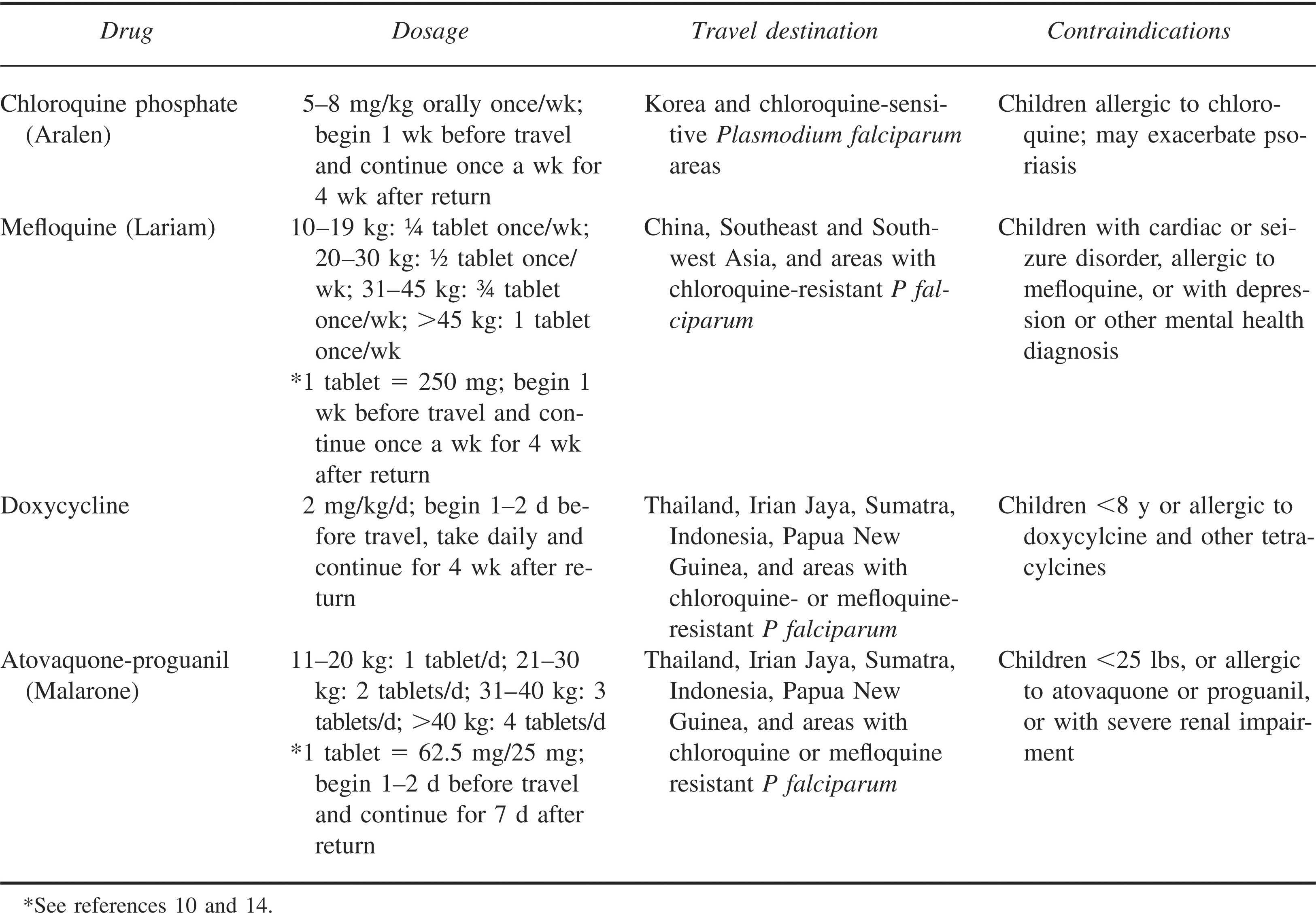
Pharmacological prevention is also recommended for all children traveling to endemic areas. There are many options for prophylaxis, with selection based on the itinerary, malaria risk of the destinations, and the species and their resistance patterns for each destination. Weekly dosed medications provide elevated serum levels and may provide slightly increased coverage if a dose is delayed. All malaria medications are most effective when taken exactly as prescribed. The most commonly used malaria prophylaxis agents for travel to Asia are mefloquine, doxycycline, and atovaquone-proguanil. 14 Chloroquine (Aralen) continues to be used in chloroquine-sensitive areas of Asia, currently only Korea. Mefloquine (Lariam), dosed weekly, can be used in chloroquine-resistant areas, including China and Southeast and Southwest Asia.14,15 Patients prescribed mefloquine should be encouraged to initiate treatment 3 weeks before travel to evaluate for significant side effects, such as anxiety and night terrors, that would prevent proper usage of the medication during travel. If intolerance is identified, the medication may be changed prior to departure. Patients with seizure and cardiac disorders should not use mefloquine. Doxycycline is a third option for pharmacological prophylaxis, with documented resistance remaining low worldwide. Use is limited to children 8 years of age and older due to concerns of dental discoloration and enamel hypoplasia. Atovaquone-proguanil (Malarone) is another medication available for prophylaxis in resistant areas and, given the ease of use, may be the preferred medication. This medication may be stopped 1 week after return from endemic areas, whereas most must be continued for 4 weeks. Malarone may be used on children 11 kg and heavier. 14 It should not be used in conjunction with rifampin, metoclopramide, or tetracycline due to a decrease in efficacy of 1 or both drugs. For dosage information of these malaria medications, see Table 2.10,14
Malaria chemoprophylaxis based on destination and resistance patterns in Asia
The CDC maintains current data on worldwide resistance patterns. Its website includes a map with up-to-date information and destination-specific recommendations for prophylaxis. 16 Providers are highly encouraged to confirm malaria prophylaxis recommendation with this website due to changing resistance patterns and the possible development of new medications and recommendations.
Dengue fever
Dengue fever is caused by a mosquito-transmitted arboviral infection in tropical and subtropical zones of the world, including South Asia. The vector is both Aedes aegypyti and A albopictus mosquitos. 10 Children may present with high fever, headache, chills, anorexia, nausea, vomiting, myalgias, and arthralgias, much like malaria. The course is self-limited, and there are currently no medications or vaccinations to prevent or treat dengue. Supportive care measures should be utilized. Hemorrhagic dengue, a more severe form of dengue infection, presents with hypotension and shock that require cardiovascular support and intervention. Treatment includes fluid resuscitation, pressors, and respiratory support required to maintain perfusion. Dengue fever prevention is best achieved with strict arthropod avoidance measures, application of permethrin and DEET, proper clothing, and activity modifications, as discussed in the Malaria section. Travelers should be advised to seek medical attention immediately to be evaluated for malaria, which presents similarly, given that delay in treatment of malaria may be life threatening, particularly in children.
Japanese encephalitis
Japanese encephalitis is the leading cause of mosquito-transmitted viral encephalitis in Asia, mostly affecting young children and adults older than 65 years of age. The incidence in Asia is 30 000 to 50 000 new infections annually. 5 The symptoms of Japanese encephalitis vary, depending on the severity of infection, from fever and headache to rapid onset of headache, high fever, neck stiffness, altered mental status, coma, tremors, and spastic paralysis. Treatment is limited to supportive care.
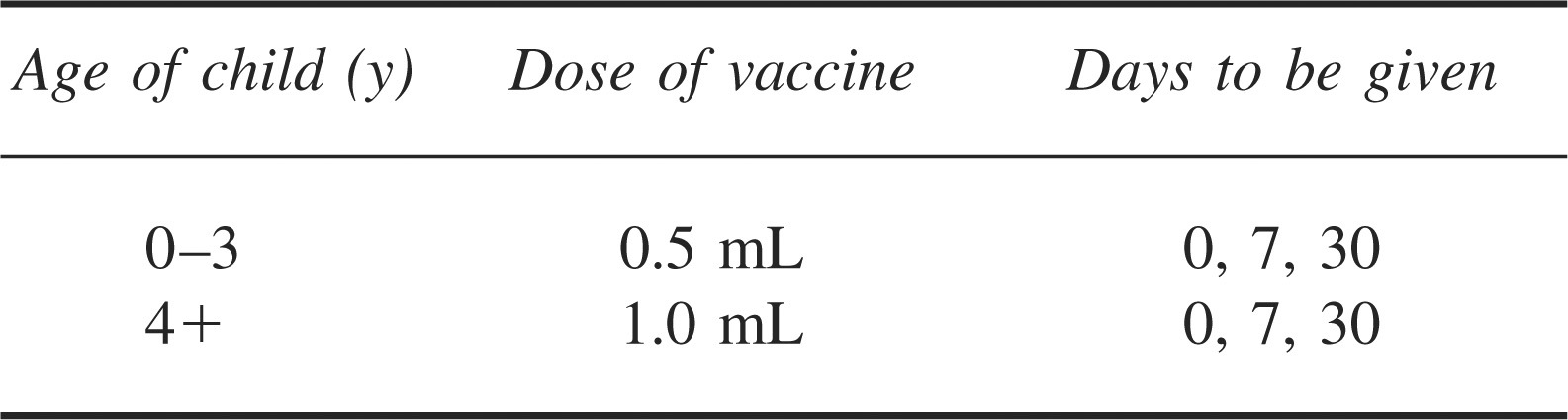
It is not recommended that all travelers to Asia receive Japanese encephalitis vaccine due to the low risk for infection in most travelers. The vaccination is an inactivated viral vaccine, JE Vax (Biken with distribution in the United States by Connaught). 10 The vaccine should be recommended to travelers to endemic areas who plan to stay for at least 30 days during the peak transmission season (spring and monsoon season), especially those visiting rural areas with a large number of rice patties and subsequent large mosquito populations. 10 Vaccination should be strongly recommended to travelers on adventure vacations with anticipated frequent exposure to arthropods. Table 3 summarizes the dosage information of JE Vax. The last dose of JE Vax must be given a minimum of 10 days before departure due to possible severe adverse effects, including urticaria and angioedema, which have been documented up to 10 days post vaccination. All travelers should be educated on arthropod avoidance measures to decrease possible exposure.
Japanese encephalitis vaccination (JE Vax) dosage information
Traveler's diarrhea
Traveler's diarrhea affects 30 to 50% of travelers to the developing world.10,17 Children are at a significantly higher risk due to limited pre-existing immunity and likely increased contact due to frequent hand-to-mouth behaviors.1,18 Adventure travelers are also at increased risk due to presumed increased exposures. Asia is ranked by the CDC as a high-risk area for the development of traveler's diarrhea, with an increased risk during the warm months preceding monsoon season. 5 The cause can be bacterial, viral, protozoal, or toxin mediated. Bacteria, including enterotoxigenic Escherichia coli, remains the most common cause (50–85% of the cases). 19 However, the pathogen remains unknown in many cases. 19 Traveler's diarrhea in children is defined as 3 or more unformed stools daily, with an additional symptom of fever, nausea, vomiting, abdominal pain, or tenesmus. Very young children will demonstrate a twofold increase in bowel movements. It is important to identify and treat invasive bacterial diarrhea, which presents with sudden onset of diarrhea, cramping, urgency, watery stools, fever, and possibly bloody stools. Protozoal diarrhea has a more gradual and less severe course, often presenting after return from travel.
Prevention of traveler's diarrhea requires strict food and water precautions and good hand washing techniques for the duration of travel in developing countries. With a large percentage of traveler's diarrhea being bacterial and protozoal, good water and food precautions can reduce exposure to the pathogens and therefore the incidence of diarrhea. Raw or poorly cooked meat, seafood, and unpasteurized dairy products should be avoided. 18 Water should only be consumed from sealed bottles, personally boiled water, or water purifiers. Ice should be avoided due to the unknown source of the water. Fruits and vegetables should be peeled or cooked before consumption. Food vendors should also be avoided due to concern of contamination. In addition to intake precautions, travelers older than 12 years of age may consider taking prophylactic bismuth subsalicylate (Pepto-Bismol), which has been shown to have a 60% efficacy in diarrhea prevention over a 7-day period. 19 It is dosed at 200 mg 4 times per day for the entire trip. 19 Children younger than 12 years of age are at an increased risk of Reye's syndrome and therefore should not take salicylate products.
Travelers who experience severe diarrhea can begin antibiotics to treat the possible bacterial sources. Treatment with oral antibiotics has been shown to significantly reduce the duration of the illness. In children younger than 12 years of age, azithromycin is the treatment of choice at a dose of 10 mg/kg/day for 1 to 3 days.17,20 Young adults may use ciprofloxacin at a dose of 500 mg twice daily for 3 days to treat the presumed bacterial diarrhea. 20 An increasingly popular choice for children older than 12 years of age, due to concerns of increasing fluoroquinolone resistance, is rifaximin, dosed at 200 mg 3 times daily for 3 days.21,22 Rifaximin is effective against E coli, making this a poor choice for travelers in Thailand, where Campylobacter remains the primary cause of traveler's diarrhea. 22 Travelers to Thailand younger than 18 years of age should use azithromycin as the first line. Prophylactic antibiotics are not recommended by the CDC; instead, treatment should be initiated at the onset of severe diarrhea. 18 Loperamide may also be given to children older than 2 years of age for treatment of nonbloody diarrhea to shorten diarrhea by an average of 1 day. 17 Loperamide is dosed at 0.1 mg/kg/dose after each lose stool, not exceeding 1 mg per day in children weighing less than 20 kg and 2 mg per day in children weighing more than 20 kg. 23 Finally, there is increasing research on Lactobacillus as a prevention measure and treatment for traveler's diarrhea with widely varying results of 15 to 60% reduction in the incidence of diarrhea. 19 The optimal dose is not yet known, and therefore no recommendation can be made. Theoretically the Lactobacillus colonizes the gastrointestinal tract and prevents pathogenic organisms from causing infection.
Parents should be educated on signs of dehydration, use of oral hydration solutions, and the importance of early feeding in the event the child has traveler's diarrhea during the trip. Early feeding has been shown to decrease changes in intestine permeability and improve nutritional status during a gastrointestinal illness. Education prior to travel ensures that parents are prepared to treat early in the illness and avoid dehydration that requires medical evaluation.
Rabies
Rabies, caused by the RNA Rhabdoviridae virus, is endemic in China, Southeast Asia, Indonesia, the Philippines, and India. The clinical presentation is characterized by an acute prodromal illness with progressive central nervous system manifestations, including seizures, paresis, and dysphagia. 24 Infection occurs after a bite or scratch by an infected animal or mucus membrane exposure. Dogs remain the primary reservoir in the developing world. 25 Travelers who are unable to report bites (young children), work with animals, have extensive unprotected outdoor exposure (hiking, camping, biking), or will be spending significant time in rural areas more than 24 hours away from a major medical facility should consider vaccination prior to travel. Prophylaxis consists of vaccination on days 0, 7, and 21. There are 2 culture-derived inactivated virus vaccines currently available in the United States: human diploid cell vaccine (RabImmune, Aventis) and purified chick embryo cell vaccine (Rabvert, Chiron). Rabies vaccine absorbed (SmithKline Beecham) is no longer produced. The objective of prophylaxis is to prevent neural tissue infection with the virus. This prevention is initiated with immediate cleansing of the contaminated tissues by wound flushing and cleaning with a povidone-iodine preparation, if available, or soap and water. 25 Postexposure prophylaxis, rabies immunoglobulin, must be given as soon after the exposure as possible in all nonimmunized individuals. 24 These individuals also require the full postexposure immunization series (on days 0, 3, 7, 14, and 21).24,25 In comparison, the fully immunized traveler requires thorough wound cleaning and a 1-mL rabies vaccination on days 0 and 3 after the possible exposure.
Prevention of this infection with pretravel immunization is increasingly warranted because the availability of rabies immunoglobulin is rapidly waning with significant reductions in production worldwide. Due to these shortages, it is vital that travelers be educated on the steps required after exposure so the patient can be a self-advocate and ensure proper treatment, which includes immunoglobulin. Pretravel prophylaxis simplifies the postexposure requirements, which is vital for travelers to countries with limited medical capabilities.
Tuberculosis
Tuberculosis is endemic in the developing world, including the majority of Asia. Eighty percent of cases are concentrated in 22 countries, with India accounting for 30%. 26 Children present 1 to 6 months after exposure with fever, growth delay, weight loss, cough, night sweats, and chills. 27 In Asia the Bacillus Calmette-Guerin vaccine is used to prevent active infections in very young children, but it has little effect on lifelong prevention of tuberculosis. 27 The recommendation is for purified protein derivative placement 12 weeks after return from an endemic area to screen for latent tuberculosis. 27 If the purified protein derivative is positive, the traveler must take isoniazid for 9 months to treat chest radiograph-confirmed latent tuberculosis infection.
Meningococcal Disease
Invasive meningococcal disease is caused by Neisseria meningitides, a gram-negative diplococcus. There are 5 serotypes: A, B, C, W135, and Y. It is transmitted by person-to-person contact, often by an asymptomatic carrier. Children generally present with symptoms of meningitis, including high fever, chills, malaise, and rash, with more fulminant cases presenting with purpura, disseminated intravascular coagulation, and shock. 28 More atypical presentations include septicemia, pneumonia, arthritis, acute otitis media, epiglottis, and pericarditis. It is recommended that travelers be immunized if traveling to areas of recent outbreak, as identified on the travel pages of the CDC website. There are 2 different vaccinations currently in use. The first, Menomune (Sanofi Pasteur), is a quadrivalent polysaccharide vaccine that covers serotypes A, C, W135, and Y. 29 It may be given as early as 2 years of age, with all children younger than 4 years receiving a booster dose after 24 to 36 months. The second vaccine is a conjugated polysaccharide diptheria toxoid quadrivalent vaccine, Menactra (Sanofi Pasteur) that also covers serotypes A, C, W135, and Y. Menactra may be used starting at 11 years of age and has been shown to provide a better immune response and therefore better protection against meningococcal disease.
Travel considerations
Children traveling to foreign countries are at risk for exposure to a multitude of infectious organisms not encountered at home. Children who are accompanying adults to visit friends and relatives in the developing world are at higher risk for acquiring infection due to travel in areas of the country that are not as well developed. 26 Developing countries often have a poorly developed health infrastructure, resulting in an increased risk of exposure to infectious agents. In addition, these visits are often of a longer duration than other vacations, increasing the risk of infection by prolonged exposure. 26
Car seats are not available in much of Asia. It is vital that children younger than 4 years of age and 40 pounds (18 kg) travel with their car seat to ensure safety during local transport. Families of such children must be encouraged to travel with car seats and be educated on proper installation.
Travelers requiring medication should travel with a sufficient supply to last the duration of the trip. It can be difficult to acquire the correct medications during travel. In many parts of Asia, prescriptions are not needed to obtain medications from the local pharmacy. However, there is a large problem with counterfeit medication sales. Travelers should be educated on the importanceof bringing a full supply of their own medications intheir carry-on luggage. More information is availableon the FDA website at
Evacuation insurance should be strongly considered when traveling to less developed countries. Each insurance company provides different coverage for medical evacuation varying from country to country. It is recommended that travelers discuss this with their health insurance company and consider additional evacuation insurance. Additionally, families should be encouraged to research medical facility options for each destination of the itinerary to reduce time to medical care in case of an emergency.
All families traveling with children should prepare a basic first-aid kit to pack in their carry-on luggage for unexpected accidents and emergencies. The kit should include bottled water and snacks if travel is delayed and food is not readily available. Adhesive bandages and wraps should be packed for minor abrasions or sprains. Antibiotic ointment, diaper rash ointment, and 1% hydrocortisone cream will cover the basic abrasions, heat rashes, and diaper rashes that often occur when traveling to warm climates. Oral hydration solution packets should be added to support hydration and are available online and at many pharmacies and camping stores. Finally, a supply of antipyretic, antihistamine, antidiarrheal, and antimalarial medications should be packed in child-proof containers with appropriate dosing information. Many kits are available prepacked, or families can pack their own first-aid bag to meet their individual travel and medical needs.
Conclusions
Traveling with children to Asia is becoming increasingly common and provides many wonderful opportunities for children and their families. Children are more at risk for travel-related illness and infection due to lack of previous exposures and age-related behaviors that place them at higher risk. Appropriate pretrip medical screening and planning can greatly reduce their risk of acquiring infections during travel. There are many resources available to help medical practitioners select appropriate immunizations and medications to be used for travel in Asia. All families traveling to developing countries should receive education and a thorough medical screening prior to departure.
Resources
International Association for Medical Assistance to Travelers ( Travax EnCompass ( International SOS ( Medex ( Centers for Disease Control and Prevention Yellow Book for travel information ( World Health Organization (
Footnotes
Acknowledgments
The authors thank Timothy Hurtado, DO, and Mark Burnett, MD, FAAP, for their assistance with the review process of this article. The authors received no outside funding or grants for this study.
The views, opinions, and findings contained in this report are those of the authors and should not be construed as official Department of the Army position, policy, or decision unless so designated by other official documentation. Citations of commercial organizations and trade names in reports do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.