
Abstract
Although avian influenza A (H5N1) is common in birds worldwide, it has only recently led to disease in humans. Humans who are infected with the disease (referred to as human influenza A [H5N1]) have a greater than 50% mortality rate. Currently there has not been documented sustained human-to-human transmission; however, should the virus mutate and make this possible, the world could experience an influenza pandemic. Probable risk factors for infection include slaughtering, defeathering, and butchering fowl; close contact with wild birds or caged poultry; ingestion of undercooked poultry products; direct contact with surfaces contaminated with poultry feces; and close contact with infected humans. Possible risk factors include swimming in or ingesting water contaminated with bird feces or dead birds and the use of unprocessed poultry feces as fertilizer. Clinically, early human influenza A (H5N1) resembles typical influenza illnesses, with fever and a preponderance of lower respiratory tract symptoms. Often, patients develop rapidly progressive respiratory failure and require ventilatory support. Treatment is primarily supportive care with the addition of antiviral medications. Currently, travelers to countries with both human and avian influenza A (H5N1) have a low risk of developing the disease. There are no current recommended travel restrictions. Travelers are advised to avoid contact with all birds, especially poultry; avoid surfaces contaminated with poultry feces; and avoid undercooked poultry products. The use of prophylactic antiviral medications is not recommended.
Introduction
Avian influenza A is an endemic disease in birds worldwide. In recent years, one strain has leapt to the forefront of media attention as avian influenza A (H5N1), with the infection and death of human patients in Asia and now deaths in the Middle East and eastern Europe. When avian influenza A (H5N1) infects humans, it is referred to as human influenza A (H5N1). This article will review the etiology, incidence, presentation, diagnosis, and treatment of human influenza A (H5N1) and its implications for travelers. It summarizes the current body of knowledge for clinicians advising travelers to countries with avian and human influenza A (H5N1) outbreaks.
Background
Avian influenza A (H5N1), a member of the orthomyxoviridae family, is a common organism found in the digestive tracts of mainly aquatic wild birds worldwide. It has been described in chickens, ducks, turkeys, guinea fowl, geese, quails, pheasants, partridges, mynahs, passerine birds, psittacine birds, budgerigars, galls, shorebirds, seabirds, and emus. 1 It typically causes few, if any, symptoms in wild birds, as it preferentially replicates in their digestive tracts and is excreted in their feces. Conversely, it can cause severe disease and oftentimes death in domesticated fowl. 1 There have been at least 17 major outbreaks of avian influenza A (H5) or (H7) subtypes in the past 30 years, resulting in the deaths of millions of birds. For example, in 1983 an outbreak of avian influenza A (H5N2) in Pennsylvania lead to the death or culling of 17 million birds at the cost of US$61 million. 1 After the identification of avian influenza A (H5N1) as the culprit in the initial 1997 Hong Kong human outbreak, 1.5 million birds were destroyed in 3 days—the entire country's poultry population. 2
This initial outbreak of disease in humans was the first documented set of illnesses attributed to human influenza A (H5N1). Eighteen people who had close contact with poultry were hospitalized, and 6 later died.
3
Before these cases, it was thought that avian influenza A (H5N1) had limited ability to directly infect and propagate in humans.1,4 Because both humans and birds possess unique receptors for their distinct viruses, and because pigs possess receptors for both avian influenza and human influenza, pigs were thought to be a necessary intermediate host.1,4 Recent outbreaks in humans who had close contact with infected poultry and not swine have challenged this notion. Per the World Health Organization, as of May 23, 2006, there have been 218 reported cases of human influenza A (H5N1) resulting in 124 deaths since 1997.
5
Although the majority of deaths have been reported in Asia, several patients in Turkey, Iraq, and Egypt recently died from the disease, indicating that it has spread to the Middle East and eastern Europe.
5
A current list of countries with documented avian and human influenza A (H5N1) infections can be found at the World Health Organization website (
Transmission
The primary mode of transmission of avian influenza A (H5N1) to humans has been animal to human. 6 –8 Activities that put people at in increased risk of contracting the disease include playing with poultry; slaughtering diseased birds; handling fighting cocks; and consuming duck blood and, possibly, undercooked poultry.6,9,10 Interestingly, workers responsible for mass culling of poultry in an attempt to stem the spread of the disease appear to be at low risk, even in instances when they did not wear personal protective equipment.2,11
There have been rare cases of suggested human-to-human transmission in several household clusters. The first case involved a child who was exposed to dying household chickens 4 days before becoming ill. Her aunt attended to her until the girl's mother arrived from a distant city to assume care. The mother had no contact with poultry, poultry feces, or poultry secretions. She did not ingest undercooked poultry products. The aunt, who initially provided bedside care for the sick child, did assist with burying the dead chickens during the initial poultry outbreak by using plastic bags to cover her hands but otherwise had no contact with infected fowl. Both women had extensive, close contact with the sick child, which included hugging, kissing, and wiping secretions from her mouth. The child died of respiratory failure secondary to pneumonia 6 days after she developed symptoms. Three days after the child's death, the mother developed a fever and rapidly progressive respiratory failure secondary to pneumonia. She died 10 days later. The aunt also developed a fever 9 days after caring for the child. She was admitted to the hospital for progressive dyspnea secondary to pneumonia. The admitting physicians, suspecting influenza, initiated treatment with oseltamivir. Her condition gradually improved and she was discharged from the hospital 2 weeks later. Specimens from the aunt and mother were positive for influenza A (H5N1) by reverse-transcriptase polymerase chain reaction. The child's body had been cremated; therefore, no postmortem specimens for influenza A (H5N1) were obtained. After a thorough epidemiologic investigation, it was believed that the most likely explanation for the family cluster of this disease was direct human-to-human transmission. 12
Recently, there have been reports of probable human-to-human transmission in Indonesia as well. The index case was a woman suspected of being infected with influenza A (H5N1) from chickens she kept in and around her house. Three chickens became ill and died, and she was known to have used chicken feces as fertilizer in her garden as well. She developed symptoms of an influenza-like illness and later died. No antemortem samples were taken for influenza A (H5N1) before her burial; however, her clinical course was consistent with the disease. During the time when the patient was severely ill and coughing heavily, 9 of her family members spent the night in a small room with her. Three of these family members became ill. In addition, 4 other family members who had close contact with the patient became ill. All 7 of these family members had laboratory-confirmed influenza A (H5N1). Six of the 7 cases were fatal. No additional cases of influenza A (H5N1) have been identified beyond the single extended family. No health care workers became ill either, even in the absence of adequate personal protective equipment. 13 Significantly, genetic sequencing of the virus responsible for this outbreak has demonstrated no evidence of reassortment between human and pig viruses as well as no evidence of genetic mutations to include mutations associated with resistance to neuraminidase inhibitors. 14
Aerosolized particle transmission is not thought to be responsible for the above instances of probable human-to-human transmission. Rather, intimate person-to-person contact is hypothesized to be the cause.6,12,13 Fortunately, the risk of transmission from patients to health care workers also seems to be low.2,6,13,14 Of 449 health care providers studied, there were 2 reported cases of suspected illness that had not been confirmed serologically and 8 cases of seroconversion that, by in large, remained asymptomatic. 6 Other theoretical avenues of human infection include the ingestion of contaminated water, mucous membrane exposure (during bathing or swimming), fomite transmission, and the ingestion of food contaminated with unprocessed poultry feces fertilizer.6,12
Clinical course
The clinical course of human influenza A (H5N1) has been extrapolated from hospitalized patients because the incidence of minimally symptomatic infections is not known. The incubation period for the disease ranges from 2 to 17 days, with the average period being 3 days.2,6,8,15,16 The majority of patients presented with fever and influenza-like symptoms with a preponderance of lower respiratory symptoms to include dyspnea with cough. Sputum production is variable. Upper respiratory symptoms are less common.2,6,8,15,16
Atypical initial presentations have been reported to include 1 case of fever with diarrhea alone 17 and 2 cases of fever with diarrhea and coma without respiratory symptoms. 18 Gastrointestinal symptoms (eg, diarrhea, abdominal pain, vomiting) are more commonly seen with human influenza A (H5N1) compared with other typical human influenza illnesses. 2 Unlike avian influenza A (H7), human influenza A (H5N1) is not usually associated with conjunctivitis.6,19 Other possible complications include multiorgan failure, pulmonary hemorrhage, pneumothorax, pancytopenia, Reye syndrome, and sepsis syndrome without documented bacteremia. 6
Radiographic findings
Patients with human influenza A (H5N1) usually develop lower respiratory symptoms early in the disease process. Nearly all patients develop pneumonia. Radiographic findings include segmental or lobar consolidations as well as diffuse, multifocal infiltrates. As patients progress toward respiratory failure, the radiograph may demonstrate diffuse, bilateral ground-glass infiltrates consistent with acute respiratory distress syndrome. The mean time to onset of acute respiratory distress syndrome in one study was 6 days.8,20
Laboratory screening
Both viral cultures and H5-specific RNA antigen studies have been successfully used to detect human influenza A (H5N1). 6 Routine viral cultures should not be performed unless appropriate Biosafety Level Laboratory precautions can be observed at all times. 21 Reverse-transcriptase polymerase chain reaction assays are superior to commercially available rapid antigen studies, which are not recommended at this time because the clinical accuracy of the detection of influenza A (H5N1) in humans is unknown. 22 It appears that pharyngeal sampling yields a higher level of detection than do nasopharyngeal swabs.6,20,22 However, because of limited clinical data, it is currently recommended that nasopharyngeal swabs, nasopharyngeal aspirates, or nasal washing be used in addition to pharyngeal swabs to collect samples. Nasal swabs and acute and convalescent sera can also be obtained. 23 For optimal yield, specimens should be obtained within 3 days of onset of symptoms. 23
During routine laboratory screening, common findings include leukopenia (particularly lymphopenia), thrombocytopenia, and a mild increase in aminotransferases.2,6,8 In one small study, increased mortality was associated with leukopenia, thrombocytopenia, and lymphocytopenia on presentation for medical care. 20 Finally, bacterial cultures are usually negative, indicating that the illness is primarily related to a viral pneumonia with limited secondary bacterial infection.2,6
Treatment
The treatment for human influenza A (H5N1) is primarily supportive. The majority of hospitalized patients require early ventilator support (usually within 48 hours of admission).2,6,20 They are typically started on both broad-spectrum antibiotics and antiviral agents. Corticosteroids, though widely used, have not shown clear clinical benefit. 6 Similar to other influenza infections, preliminary data indicate that the early administration of antiviral agents offers the greatest advantage, whereas instituting antiviral therapy late in the illness provides little benefit.2,6,24
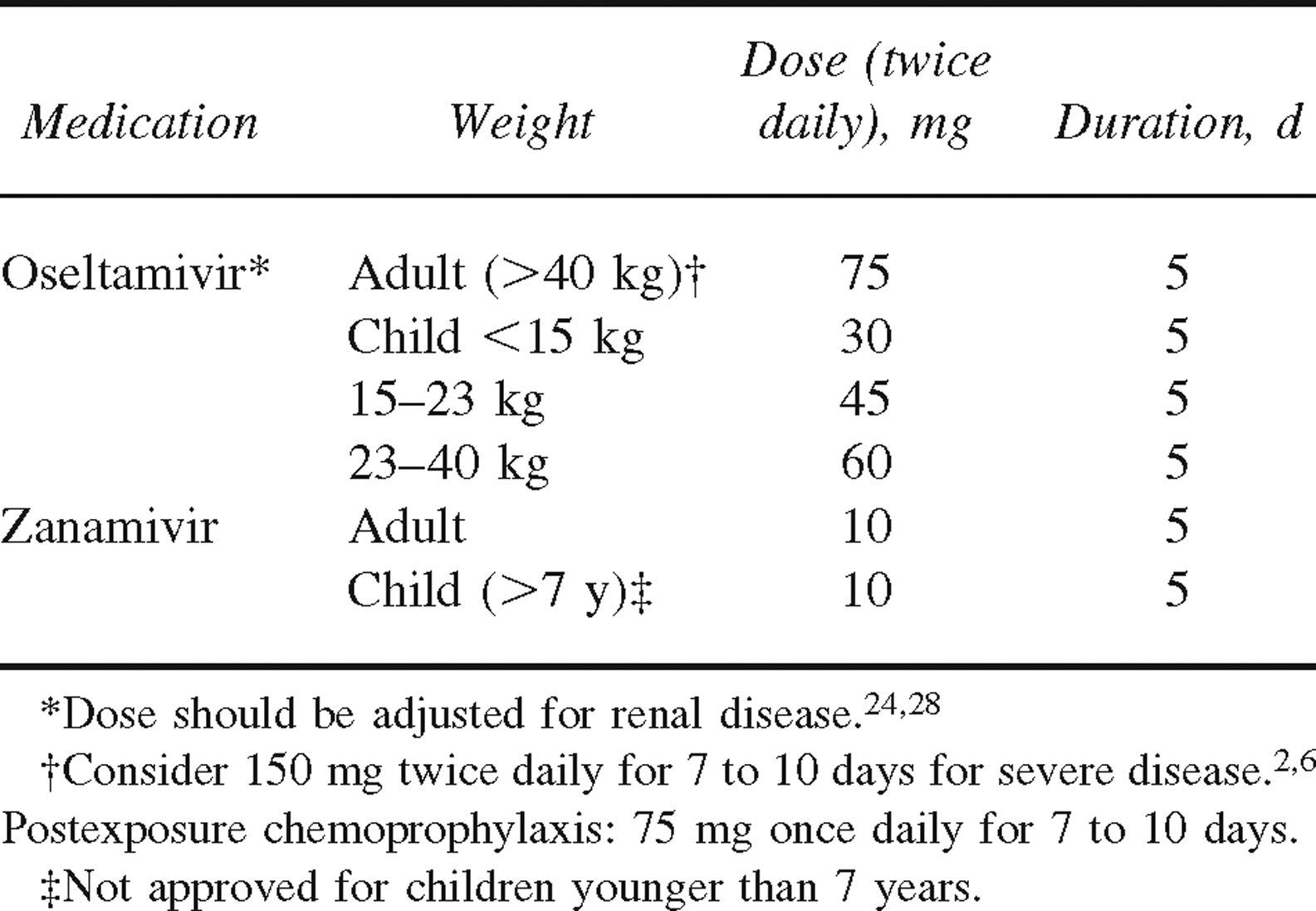
The oral neuraminidase inhibitor oseltamivir appears to be the most useful agent. Although 5 days of therapy is considered adequate for treating mildly symptomatic patients early in the disease process, higher doses may be needed for a longer duration in more severe infections. The optimum dose and duration has not been prospectively studied, and the dose should be adjusted for renal disease.2,6,25–27 The inhaled neuraminidase inhibitor zanamivir has been used in animal models with some success; however, it has not been studied in humans. Table 1 summarizes the treatment of human influenza A (H5N1) with the neuraminidase inhibitors.
Drug-resistant human influenza A (H5N1) has recently made the news with case reports of oseltamivir-resistant infections, primarily in Vietnam. 30 This is significant because the older antiviral M2 inhibitors, amantadine and rimantadine, are ineffective against this organism.6,24 Should human influenza A (H5N1) develop widespread resistance, the pharmacologic treatment options would be severely limited.
Future considerations
A major concern is a mutation of avian influenza A (H5N1) that would allow sustained human-to-human transmission. An antigenic shift in avian influenza A (H5N1) that allows direct human-to-human transmission could spark the next global influenza pandemic. Because human immune systems have had little exposure to avian influenza A (H5N1), it is plausible that direct human-to-human transmission of a new viral genome would lead to widespread infection and high mortality. (Currently, laboratory-confirmed human influenza A [H5N1] infections that are symptomatic have an approximately 50% mortality rate.) It has been estimated that an influenza pandemic in the United States would yield up to 50 million infected individuals, hospitalize 700 000 people, cause 100 000 to 200 000 deaths, and cost US$100 billion to US$200 billion. 31
Prevention
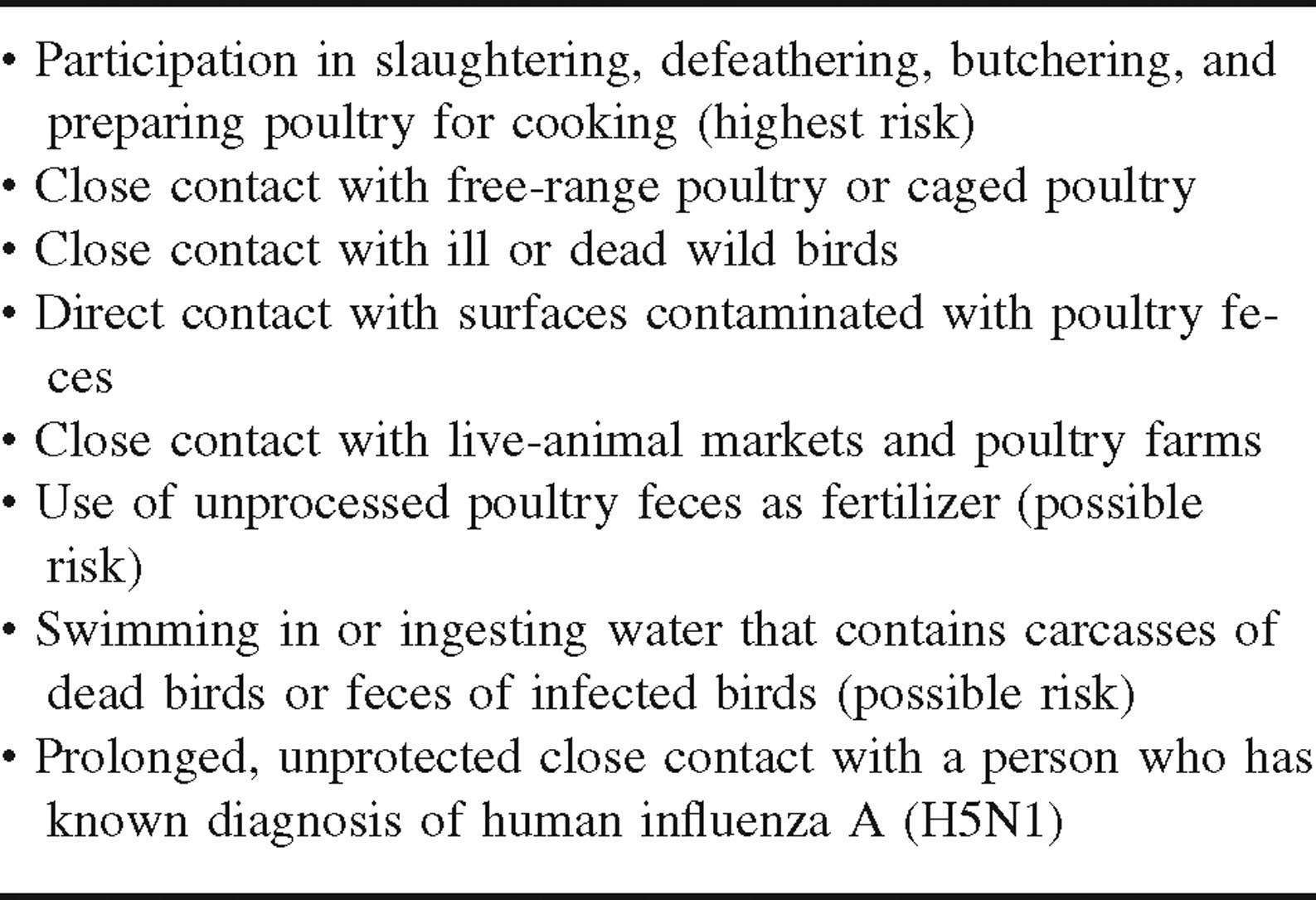
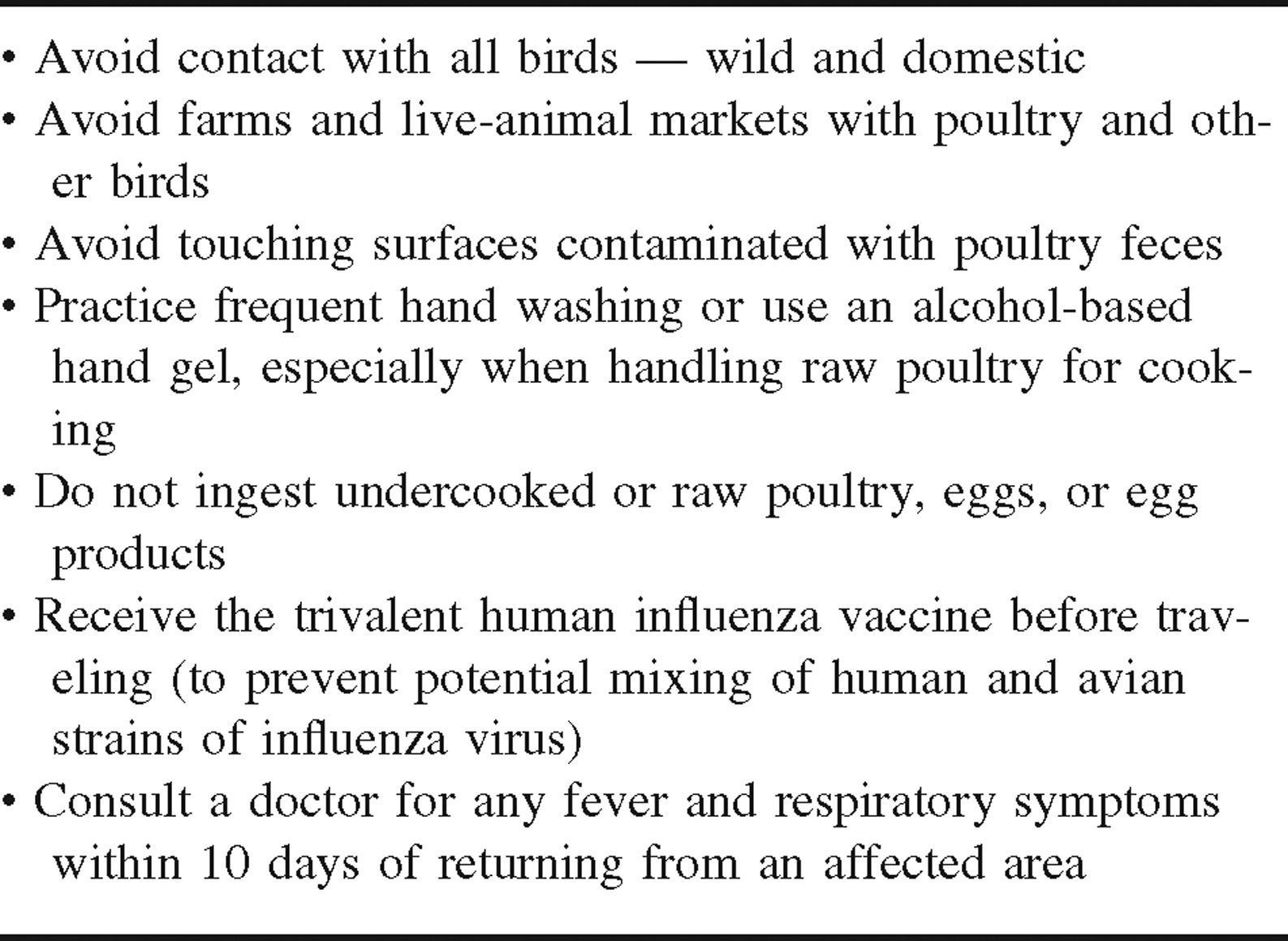
With such dire predictions regarding a possible human pandemic, prevention of the disease has become a key focus. Although there are currently no commercially available influenza A (H5) vaccines available for humans, several are under investigation.6,32 These include conventional parenteral preparations, as well as intranasal vaccines. Therefore, prevention of direct transmission from infected fowl to humans and the prevention of nosocomial infections are of paramount importance. Table 2 describes risk factors for community-acquired infection with human influenza A (H5N1). Prevention of nosocomial infections is reviewed elsewhere. 6 Postexposure chemoprophylaxis should be considered in health care workers and household contacts who have been exposed to patients with known disease, infectious aerosols, and bodily secretions.6,26 It should also be made available to people who have participated in high-risk behaviors (see Table 2). Table 3 describes general advice to travelers who are visiting countries experiencing human influenza A (H5N1) outbreaks.
Considerations for travelers
Currently, the World Health Organization and the Centers for Disease Control and Prevention do not recommend travel restrictions for countries experiencing human or avian influenza A (H5N1) outbreaks, nor do they recommend routine screening of travelers returning from these countries. Because there are no reports of sustained human-to-human transmission, the likelihood of contracting the disease while traveling and exercising prudent precautions is thought to be very low.33,34 Also, because influenza viruses are destroyed by heat (>74°C, or 165°F), there is no risk of contracting human influenza A (H5N1) by eating properly cooked poultry, eggs, or egg products. Finally, there is no indication that taking prophylactic antiviral medications is helpful in preventing travelers from becoming infected.
Conclusion
Travelers’ current risk of contracting human influenza A (H5N1) is low, providing they exercise caution. Although the incidence of infected poultry is high, the risk to humans is low and the incidence of human-to-human transmission continues to be rare. Consumption of well-cooked poultry and egg products does not put travelers at risk for infection, and the use of antiviral chemoprophylaxis is not required under normal circumstances. Currently, there are no recommendations for travel restrictions. Should the human influenza A (H5N1) mutate and demonstrate sustained human-to-human transmission, these risks would change.
Footnotes
Acknowledgment
The author would like to thank Christine Waasdorp, MD, FAAP, for assistance with the review process. The author received no outside funding or grants for this study.
*
The views, opinions, and findings contained in this report are those of the authors and should not be construed as official Department of the Army position, policy, or decision unless so designated by other official documentation. Citations of commercial organizations and trade names in reports do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.