
Abstract
Fatalities following rattlesnake bite are rare in the United States, usually occur some hours following the bite, and are generally secondary to direct venom effects. We report a patient with acute syncope and subsequent massive aspiration resulting in airway obstruction and rapid death following a probable Northern Pacific rattlesnake (Crotalus oreganus oreganus) bite.
Introduction
Venomous snakes inflict approximately 7000 to 8000 bites in the United States each year. 1 The consequences of these bites are usually limited to local tissue problems, and deaths are uncommon. Only 97 deaths were reported in the United States during the 20-year period from 1979 to 1998. 2 Sudden death is extremely rare, though early deaths occasionally occur, particularly in bites to the head, face, or neck that result in airway swelling and asphyxiation. 3 We report a case of rapid death following a rattlesnake bite to the hand of an otherwise healthy adult man.
Case report
The victim, a 46-year-old man without any history of previous venomous snakebite or significant medical problems was alerted to the presence of a “large” rattlesnake in his yard by his wife, who found it and heard it rattle. The man, who had last eaten 20 minutes earlier and had not had any alcohol to drink, attempted to pin the snake with an object while his daughter went to get a shovel to kill it. As he restrained the snake, he lost his grip and was bitten on the web of his left hand, between the thumb and first finger. He yelled to his daughter, who witnessed the event; he then walked approximately 6 feet and collapsed face down on the ground.
The local emergency medical service was immediately summoned. The emergency medical technicians initially were told that the man was unresponsive, but breathing spontaneously. Five minutes before arrival (15 minutes after the event), they were recontacted and told that family members were attempting cardiopulmonary resuscitation.
The emergency medical technicians arrived on scene approximately 20 minutes after the bite, and, on primary examination, found the patient unconscious with his oral pharynx full of emesis and blood. He had obvious facial trauma to his nose, mouth, and teeth (had broken a dental bridge), with swelling of his distal tongue and posterior oropharynx. He had no spontaneous respirations, no pulse, and was cyanotic above the nipple line. His pupils were fixed and dilated, and he had a Glasgow Coma Scale score of 3. Blood was oozing from the bite wound on the web of his left hand.
Cardiopulmonary resuscitation was continued and an automatic external defibrillator was attached, but no shock was advised. Seven minutes later (approximately 30 minutes after the bite), an advanced life support unit with paramedics arrived on the scene. The man was placed in full spinal immobilization and loaded into an ambulance. In the ambulance, the cardiac monitor revealed asystole, and pulse oximetry revealed an oxygen saturation of 48%, with ventilations being performed by bag valve mask with high-flow oxygen.
While the ambulance was en route to the nearest hospital, endotracheal intubation was attempted, but was unsuccessful because of inability to visualize the vocal Two minute puncture marks are visible postmortem. The hand proximal to the bite is edematous, with swelling extending to the wrist. A 1.5 × 1-cm area of purplish discoloration is present at the base of the thumb.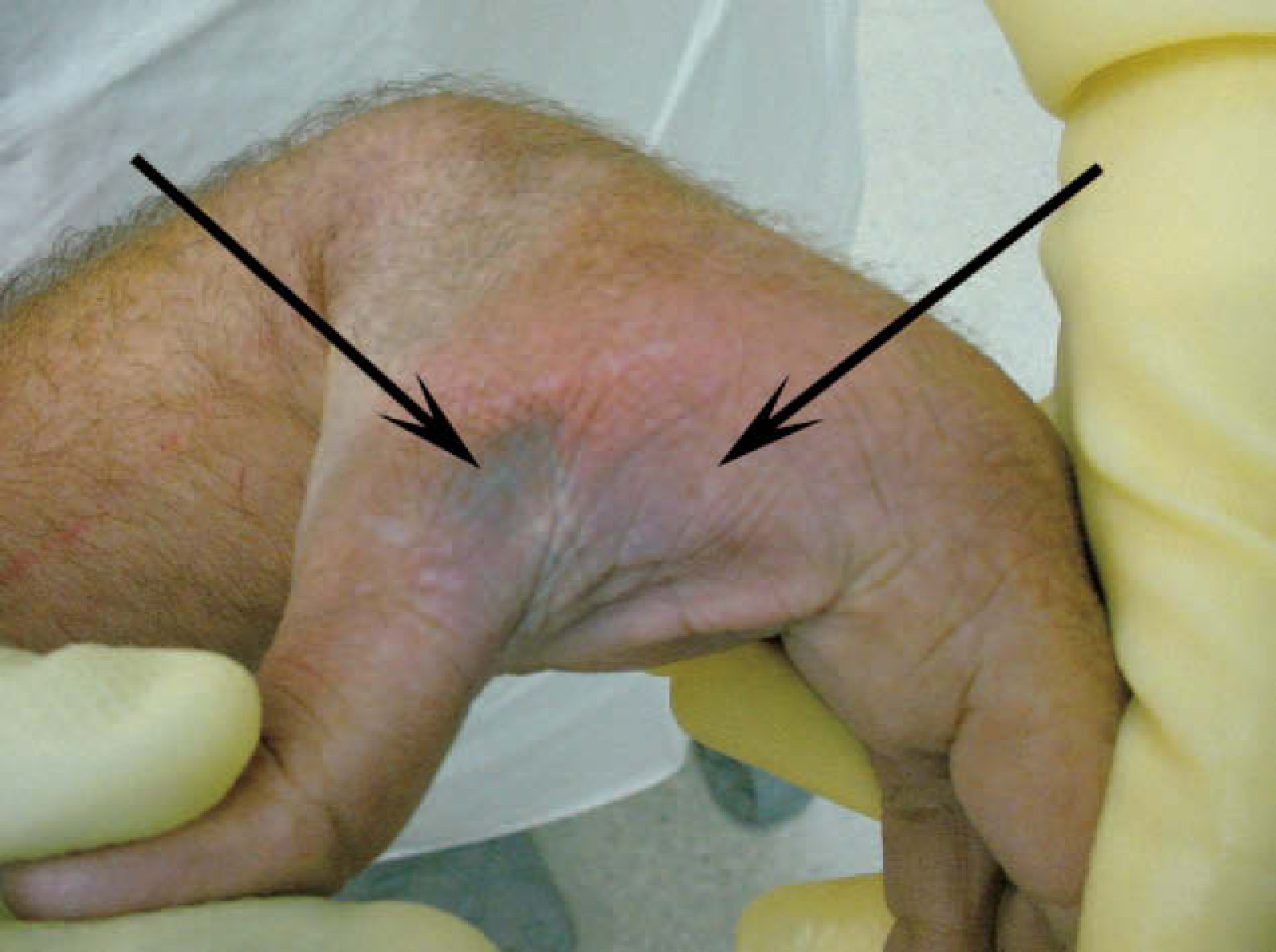
After a peripheral intravenous line was placed, the patient received multiple doses of epinephrine, atropine, and lidocaine intravenously. A finger-stick blood glucose reading of 57 mg/dL prompted administration of 25 g of intravenous dextrose. Ventricular fibrillation was then noted and attempts were made to defibrillate the patient 4 times en route without success. One hour after being bitten by the rattlesnake, the patient arrived at the emergency department.
In the emergency department, cardiopulmonary resuscitation was continued. Extensive suctioning of the Combitube and oral pharynx removed large amounts of liquid and solid matter (approximately 800 mL). Subsequently, the Combitube was removed and an attempt was made to orally intubate the patient. The tube was irrigated multiple times in an effort to clear the gastric contents in the patient's airway. After these maneuvers, the patient reportedly was able to be ventilated, but needed frequent suctioning. After the intubation, pulse oximetry improved to 88% on 100% FiO2, but no spontaneous respirations or pulse were observed, and the cardiac monitor indicated asystole. Eighteen minutes after arrival in the emergency department, the patient was pronounced dead.
Postmortem examination revealed crotalid envenomation manifested by fang wounds, edema, and ecchymosis of the left hand (Figure). The likely offending reptile, based on the geographic location (Mariposa County, CA) was a Northern Pacific rattlesnake (Crotalus oreganus oreganus). 4 The autopsy report indicated that the endotracheal tube was misplaced into the esophagus. Remnants of aspirated food were present in the trachea, the major bronchi, and the major lobes of the right and left lungs. Both lungs were moderately congested and edematous. No evidence of intracranial injury was found. No postmortem laboratory studies were obtained. Cause of death was cerebral and cardiac hypoxia resulting from airway obstruction by gastric contents.
Discussion
Syncope has been reported as a sequela of venomous snakebite. 5 Whitley reported syncope and hypotension in a 65-year-old male bitten over a saphenous vein by a copperhead (Agkistrodon contortrix). 6 In a review of 9 snakebite deaths in Arizona, Hardy reported 2 patients who immediately collapsed following bites by rattlesnakes. 7 In 2 of these cases, including 1 of those who collapsed immediately, the cause of death was ruled secondary to hypoxic brain damage from airway obstruction.
Some have suggested, as a possible mechanism for syncope following snakebite, venom-induced autopharmacological release of endogenous vasoactive compounds such as histamine and bradykinin, resulting in an anaphylactoid reaction.8,9 Although it is possible that the cause of this patient's collapse was an anaphylactoid response to venom, this is unlikely given the very small amount of circulating venom that could have been absorbed in the seconds that followed the bite. Apparent anaphylactoid reactions have been reported following venomous snakebite,10,11 but in most of these cases there were other findings suggestive of an allergic-type reaction, including urticaria and/or angioedema, none of which were seen in this case. According to the victim's wife, he had killed at least 20 rattlesnakes on his property prior to his fatal bite, but had never previously been bitten. It is possible that he had had some form of prior mucosal venom exposure in the past that might have sensitized him to rattlesnake venom, but we feel that a true immunoglobulin E–mediated anaphylactic reaction is unlikely, again given the absence of any other findings consistent with anaphylaxis, with the exception of hypotension.
In cases of death thought to be possibly caused by anaphylactic or anaphylactoid reactions, postmortem measurement of serum tryptase may help prove the diagnosis. 12 Tryptase is released by mast cells during such reactions, and its serum half-life is significantly longer than that of histamine. Tryptase levels tend to rise over time in the postmortem period, and thus blood for testing should be drawn as soon after death as possible when anaphylactic or anaphylactoid reactions are suspected. Tryptase levels may also be elevated in deaths related to severe blunt chest trauma or atherosclerotic heart disease. 13
It is also very unlikely that this patient's loss of consciousness was caused by direct venom effects, again given the very small amount of venom that could have been absorbed and circulated in the seconds prior to his collapse. A direct, intravascular envenomation cannot, however, be ruled out as contributing to his demise. It is very unlikely that even direct intravascular venom deposition could have caused his collapse within seconds. Though there was postmortem evidence of envenomation, it is more likely that the patient suffered a sudden neurogenic syncopal episode in response to the emotional shock of being bitten. This led to his loss of consciousness and vomiting with an unprotected airway. If clearing and securing his airway had been possible, he likely would have survived. Nevertheless, this case is unusual in that it represents a rare sudden death following rattlesnake bite.
From this case and the other few similar cases in the literature, it is clear that aggressive attempts to protect and control the airway are required in any victim who collapses suddenly following a venomous snakebite.