
Abstract
Flying snakes (Genus Chrysopelea) are a group of ophisthoglyphous colubrids in South and South East Asia known for gliding in the air. Of the five species of flying snakes, Sri Lankan flying snake, Chrysopelea taprobanica, is endemic to Sri Lanka. Authenticated bites and the venom characteristics of this uncommon snake remain unknown. We report the first authenticated case of C taprobanica bite, in which a 45-year-old woman had signs of mild local envenoming after the bite, with no evidence of systemic envenoming.
Keywords
Introduction
Although snakebite leads to high morbidity, identification and documentation is poor in many parts of the world. Reports on medically significant and authenticated colubrid bites are even rarer. 1 Annually, approximately 37,000 snakebite victims are admitted to government hospitals in Sri Lanka, of which bites only 1% to 10% are caused by mildly venomous and nonvenomous snakes. 2 Very few reports have been published about mildly venomous snakebites from Sri Lanka. 3
Flying snakes of the genus Chrysopelea are arboreal colubrids known for their unique ability to glide through the air. 4 Similar to some other colubrid snakes, flying snakes possess enlarged posterior maxillary teeth, produce venom from Duvernoy's glands, and are believed to be mildly venomous. 4 The genus Chrysopelea comprises five species, namely, Chrysopelea pelias (Linnaeus, 1758), Chrysopelea paradisi (Boie, 1827), Chrysopelea rhodopleuron (Boie, 1827), Chrysopelea ornata (Shaw, 1802), and Chrysopelea taprobanica (Smith, 1943). The latter two species are present in Sri Lanka whereas C taprobanica is endemic to Sri Lanka. Reports on bites caused by these snakes appear to be limited to C pelias, 5 C paradisi, 6 and C ornata. 3 Basic characteristics of the flying snakes remain unexplored, 6 and hence, clinical reporting of the authenticated bites becomes important. Here, we report an authenticated C taprobanica bite from Sri Lanka that appears to be the first such case.
Case Presentation
A 45-year-old woman was bitten on her right thumb by a snake hanging to the window grill when she was trying to close the window panes of her bedroom on August 23, 2012, at 9:00
On admission to the teaching hospital in Anuradhapura, the patient had moderate pain, mild swelling, and erythema around the base of the right thumb. The numbness was radiating along the right upper limb. Three puncture marks were observed arranged in a triangular shape at the right thumb (Figure 1). Her pulse was 74 beats per minute and her blood pressure was 120/70 mm Hg. The victim had no signs suggestive of neurotoxicity such as ptosis, ophthalmoplegia, weakness, or dizziness. No bleeding manifestations were observed. The whole blood clotting time, 3 hours after the bite, was more than 20 minutes (normal value, less than 20 minutes). The clotting time was 90 seconds (normal value, less than 8 minutes). The electrocardiogram showed no abnormalities, and urine analysis was normal. The random blood sugar was 5.6 mmol/L (3.9–7.8 mmol/L). White blood cell count was 4900/mm3 with 59% neutrophils and 40% lymphocytes. The blood urea was 3.2 mmol/L (normal values, 2.9–8.2 mmol/L), serum creatinine was 67 μmol/L (normal values, 60–120 μmol/L), and her serum Na+ and K+ levels were 147.0 mmol/L (normal range, 135–147 mmol/L) and 4.4 mmol/L (normal range, 3.5–5.2 mmol/L), respectively. Tetanus toxoid was given, and oral cloaxicillin therapy was begun. The repeat whole blood clotting time done 9 hours after the bite was again more than 20 minutes. The local swelling and the numbness radiating up along the right arm was completely settled within 6 hours of the bite, although the moderate local pain persisted until the patient was discharged from the ward on the following day. The offending snake (Figure 2) was 58 cm in total length and was identified, using the identification key described by De Silva, 4 as an adult female Sri Lankan flying snake (C taprobanica, Smith, 1943).

Photograph of the right hand of the patient, showing the site of the bite (encircled), 12 hours after the bite. (Used with permission of the patient.)
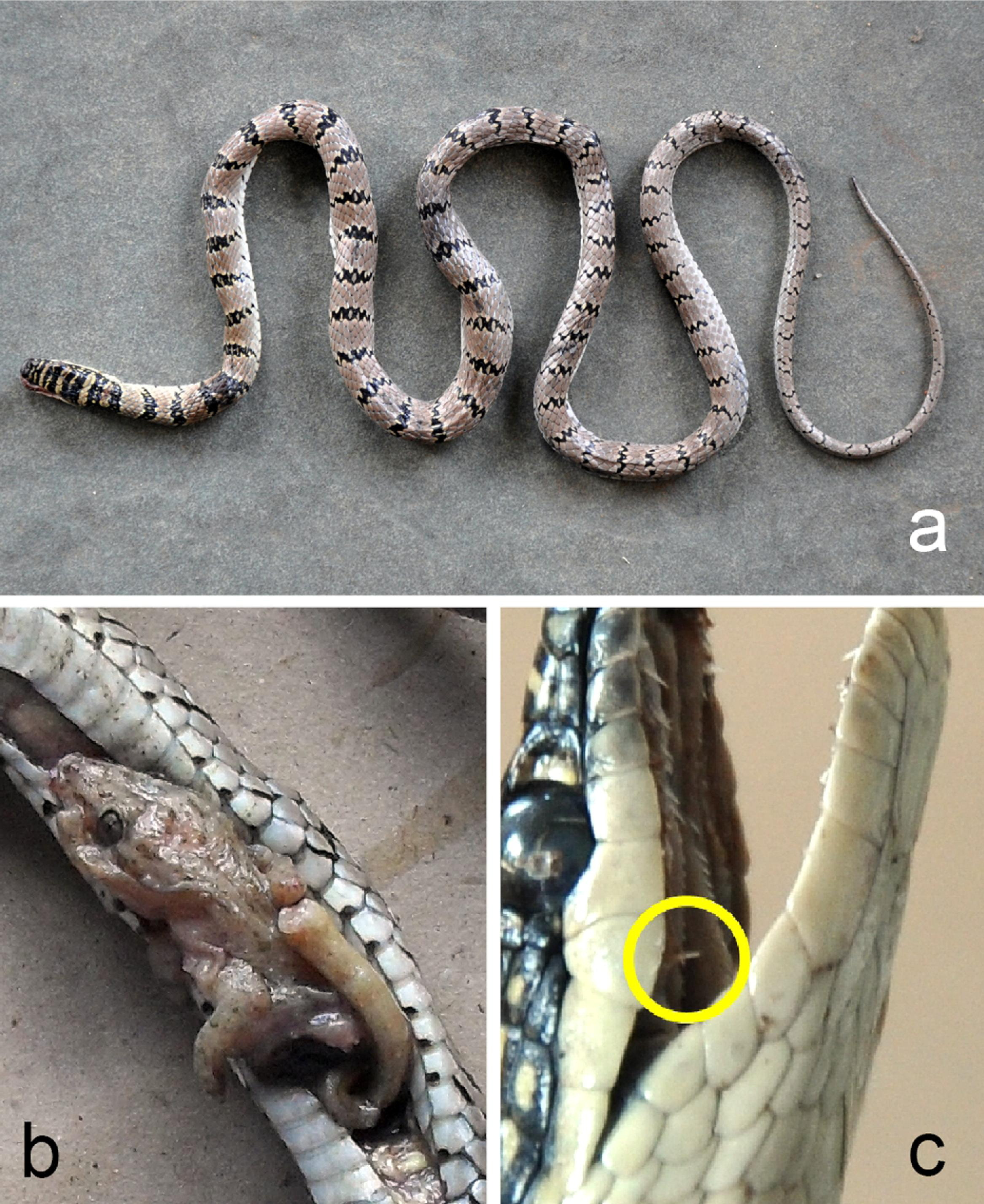
(a) The offending snake, an adult female (total length, 58 cm) Sri Lankan flying snake (Chrysopelea taprobanica, Smith, 1943). (b) Partially digested specimen of adult common house gecko (Hemidactylus freanatus, Schlegel, 1836) among the gut content of the snake. (c) Head of the offending snake; note the enlarged posterior maxillary teeth (encircled) used in delivering the secretions from Duvernoy's gland.
Discussion
Chrysopelea taprobanica is restricted to dry and intermediate zones of Sri Lanka.4,7 Because this snake is uncommon, arboreal, and prefers forests, encounters with humans are rare. Extensive literature search, including the gray literature, failed to locate a single report of authenticated bite of C taprobanica; hence, this is probably the first authenticated such report.
In this patient, signs and symptoms of the C taprobanica bite were limited to mild local effects and are likely to be effects of the secretions (venom) from the Duvernoy's gland of the snake. No local or systemic envenoming signs were observed in patients bitten by C paradisi 6 or C ornata. 7 However, moderate local pain radiating along the lower limb and numbness that persisted for days had been observed in a patient bitten on her right middle toe by C pelias. 5 It is difficult to comment further on this as the venom characteristics of these snakes remain unknown. 5
The observed transient prolongation of whole blood clotting time does not confirm presence of a coagulopathy, as the laboratory clotting time performed at the same time was found within the normal range. However, transient derangement of the coagulation profile had also been previously observed in a victim of C paradise, 6 and therefore, such activity in C taprobanica venom cannot be completely excluded.
The venomous colubrids possess a low-pressure venom delivery system. 8 A considerable volume of Duvernoy's secretions being injected into this patient was unlikely because the snake reportedly had not hung on to the victim's finger. In addition, gut contents of the offending snake revealed partially digested specimen (Figure 2b) of adult common house gecko (Hemidactylus freanatus, Schlegel, 1836), indicating the snake must have used its venom on the gecko before biting the patient. That may also have contributed to the reduced effects of the venom.
Interestingly, the first attempt to characterize venom of a flying snake was by Alcock and Rogers, 9 who experimentally injected extracts from crushed parotid glands (probably Duvernoy's glands) of a juvenile C taprobanica subcutaneously to rats in 1902. There were no toxic effects on the rats, and the researchers speculated that the venom's low potency may have been due to the snake being a juvenile. However, medically significant properties of venoms of flying snakes remain unknown owing to the dearth of experimental venom studies, as in the case of many other colubrid snakes. 2
We report the first authenticated human case of a Sri Lankan flying snake (C taprobanica) bite. In this case, the patient had signs of mild local toxicity with no evidence of systemic envenoming.