
Abstract
Objective
Our objective was to determine the incidence of acute mountain sickness (AMS) and the cardiorespiratory responses, in children and their parents, after rapid ascent to 3500 m. The sample population was composed of children and their parents who ascended within 24 hours from Arica (sea level) to Putre (3500 m) in Chile.
Methods
Acute mountain sickness symptoms were evaluated using the Children's Lake Louise Score (CLLS) in children and the Lake Louise Scoring System in their parents. Heart rate, pulse oximetry, and AMS symptoms were evaluated in Arica before ascent, in Putre, and on return to Arica.
Results
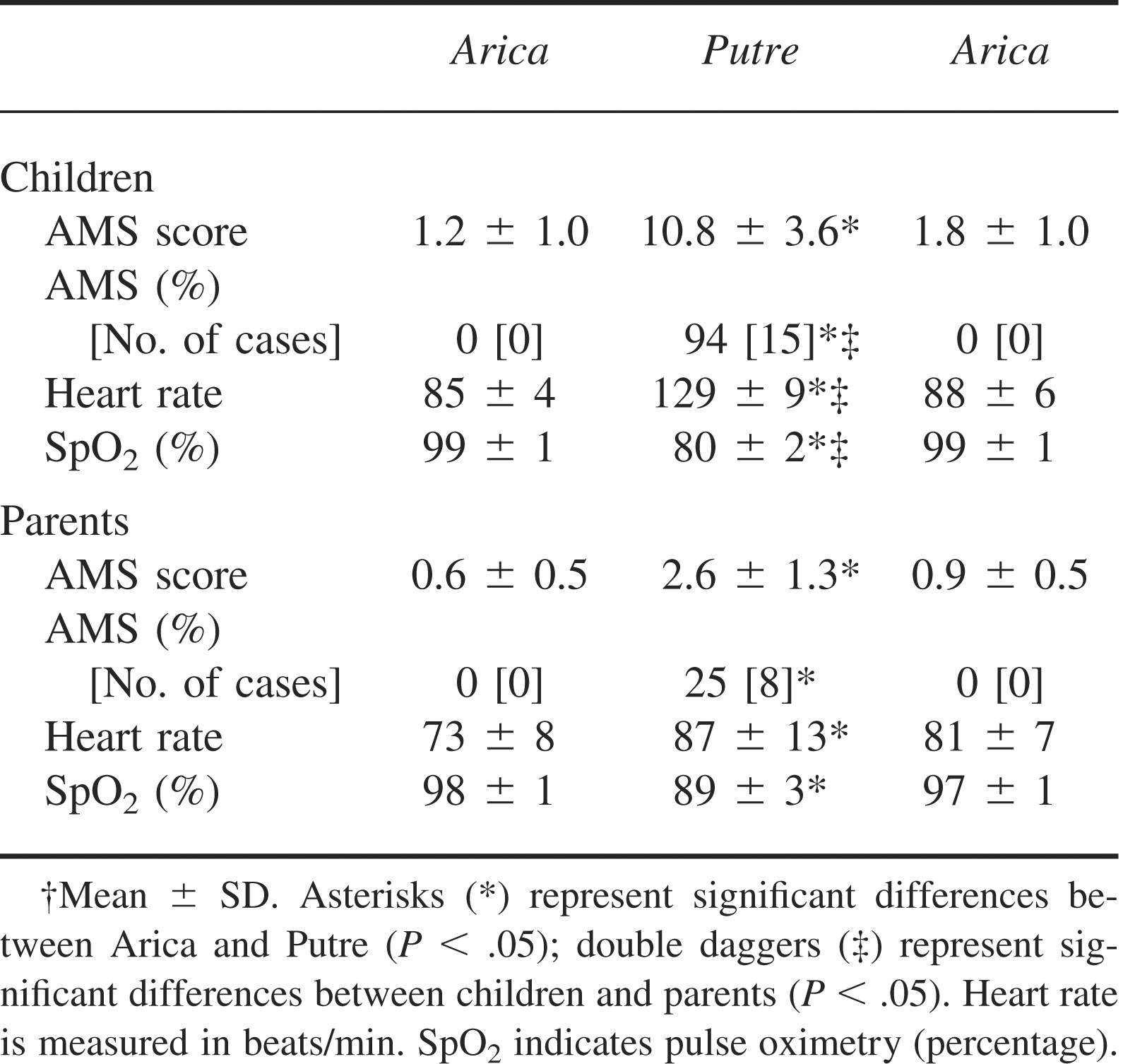
The mean CLLS was 10.8 ± 3 at Putre, with 92% of children developing AMS. Low oxygen saturation (80% ± 2%) and tachycardia (129 ± 9 beats/min) were observed in children with higher AMS scores. In contrast, parents had higher oxygen saturation (89% ± 3%), less tachycardia (87 ± 13 beats/min), and a 25% incidence of AMS.
Conclusions
Our results indicate that children exposed acutely to high altitude are more sensitive to hypobaric hypoxia than are their parents, as manifested by symptoms of AMS, significant oxyhemoglobin desaturation, and tachycardia. Young children may experience an exaggerated hypoxemic response to high altitude exposure, and young age may be an additional risk factor for the development of AMS.
Introduction
The first description of malaise associated with ascent to high altitude was written by the priest Jose de Acosta in 1590. 1 However, a more complete description of “soroche” (or acute mountain sickness [AMS]) was compiled by Ravenhill in 1913. 2
Presently, AMS in adults is defined by the following signs and symptoms: headache, fatigue and/or weakness, gastrointestinal symptoms, dizziness/light-headedness, and difficulty sleeping. Symptoms can appear between 4 and 8 hours and up to 96 hours after arrival at high altitude. 3 The likelihood of developing AMS is determined by individual susceptibility, speed of ascent, altitude attained, and previous acclimatization.3,4 Age and gender also appear to be significant factors in the development of AMS, as several studies have shown that older people are less susceptible to AMS, 4 –7 and evidence indicates that women seem to be less susceptible than men.3,5
Several questionnaires, such as the Lake Louise self-assessment questionnaire (LLS), have been developed to assess the symptoms and signs of AMS, principally among trekkers, climbers, and tourists. The LLS has been widely used for the study of AMS in adults. 8 However, there is little knowledge related to the occurrence of AMS in infants or children. In recent years a questionnaire that allows diagnosis of AMS in preverbal children has been developed; the scale is a modified LLS that incorporates a pediatric symptom score and a fussiness score. 9 The use of this questionnaire has shown that the incidence of AMS in preverbal children is similar to that observed in adults up to moderate altitudes. 9 Furthermore, in another study performed by Yaron et al, 10 children less than 36 months of age and their parents ascended from 1610 m to spend a night at 3100 m. This produced a similar incidence of AMS in both children and their parents after acute ascent. In contrast, Moraga et al 6 described a higher incidence of AMS with low arterial oxygen saturation in 6 preverbal children at 3500 m, indicating that children under 36 months of age are more susceptible to high altitude than teenagers and adults. Our objective was to determine the incidence of AMS in children (3–5 years of age) and their parents after rapid ascent to 3500 m.
Participants, materials, and methods
Sixteen children (9 male/7 female) under 5 years of age and their parents with no previous experience of high altitude exposure participated in the study. The sample population was composed of tourists (parents and children) who ascended from sea level (Arica) to the town of Putre (3500 m) located 145 km northeast of Arica in the province of Parinacota, Chile.
At sea level (Arica), tourists with children were contacted through travel agencies that take tourists to high altitude. All participants arrived in Arica on holiday and were hoping to stay in Putre over night. When a group of tourists with children was contacted, a nurse visited them, giving them information about the objective of our study. At this point children were evaluated in order to ensure that they had no respiratory illness, ear inflammation, or viral infection. Furthermore, an interview with the parents highlighted any history of cardiopulmonary illness. If there was such a history, they were informed of the risks involved in taking children to high altitude.
Parents of all children signed consent forms prior to participation in the study. This study follows the Helsinki protocol and was approved by the Ethical Committee of the Universidad de Antofagasta.
We evaluated heart rate and arterial oxygen saturation in all children and parents by pulse oximetry (Nonin 8500M, Nonin Medical Inc, Plymouth, MN). Acute mountain sickness was diagnosed in children by use of the Children's Lake Louise Score (CLLS) and in parents by the LLS.8,9 Briefly, the CLLS questionnaire identifies AMS in children who show signs and symptoms of nonspecific irritability (fussiness score ≥3) and a pediatric symptom score (appetite/vomiting, playfulness, sleep disturbance) totaling ≥4. The CLLS is positive when the fussiness score plus the pediatric symptoms score is ≥7. 8 The LLS self-questionnaire evaluates 5 items: headache, gastrointestinal symptoms, fatigue and/or weakness, dizziness/light-headedness, and difficulty sleeping. Each item has a score of 0 to 3. We considered AMS present in participants for whom the sum of the scores was ≥3. 9
Measurements in parents and children were made over 3 separate days. The CLLS was measured daily after breakfast by the mother on days 1 to 3. Day 1 measurements were made in a hotel room in Arica at sea level; on day 2 at high altitude, children were evaluated on arrival at the primary care center and the following morning in a hotel room in Putre; on day 3 at sea level, children were evaluated in the hotel room in Arica.
If children presented symptoms of AMS associated with low oxygen saturation (<80%) it was considered that they had severe AMS, and they were taken to the primary care center and stabilized with bed rest and oxygen (0.5–1 L·min−1 for 30–60 minutes). If oxygen saturation and symptoms of AMS did not improve after 2 hours of observation, parents were recommended to descend with their children.
Statistics
The AMS in children and adults was expressed as a percentage, and the differences between groups were tested by a proportional test. Cardiorespiratory measurements were expressed as mean ± SD. The difference between groups was tested by analysis of variance, followed by rank analysis with the Newman-Keuls test; and for simple relationship, the Spearman correlation test was used. Significance was assumed at P < .05 (Statistica Statsoft, Tulsa, OK).
Results
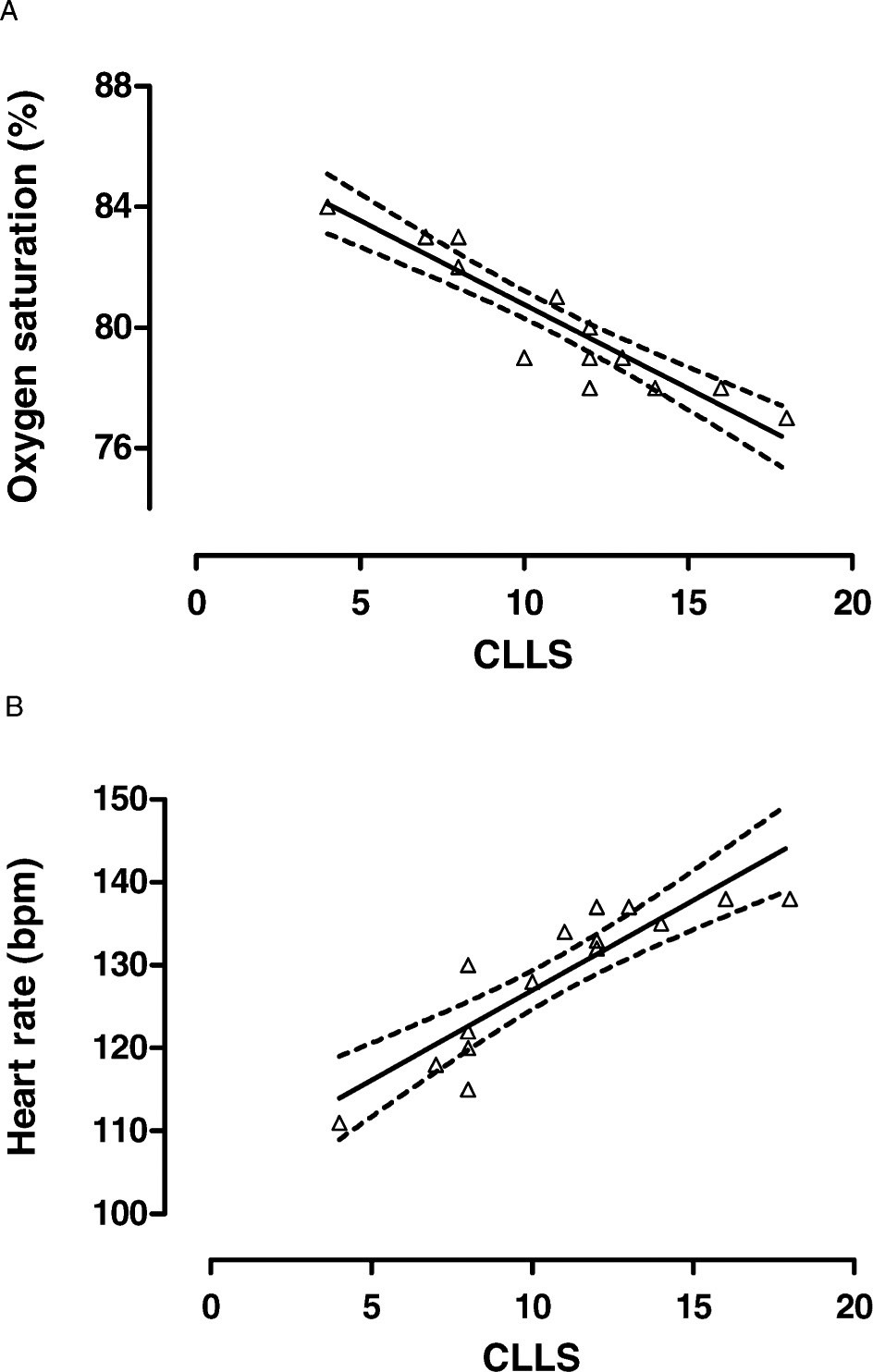
The sample population consisted of 16 children of 4.3 ± 1.0 years of age (age range, 3–5 years) and their parents (age range, 27–36 years). Cardiorespiratory responses and CLLS values in children at sea level (Arica), at high altitude (Putre), and on return to Arica are shown in Figure 1 and Table 1. We observed that the children at sea level (Arica) had lower CLLS values, showed no signs of AMS, and had normal heart rates and oxygen saturations. In contrast, at high altitude higher CLLS values were observed and increased percentages of AMS, which represented 15 of 16 children, plus a significant increase in heart rates and a decrease in oxygen saturations were noted. After return to Arica, CLLS values, percentage of AMS, heart rates, and oxygen saturations returned to values similar to those observed before ascent. A negative relationship between CLLS value and arterial oxygen saturation was also found (Figure 2A); also found was a positive relationship between CLLS value and heart rate (Figure 2B).
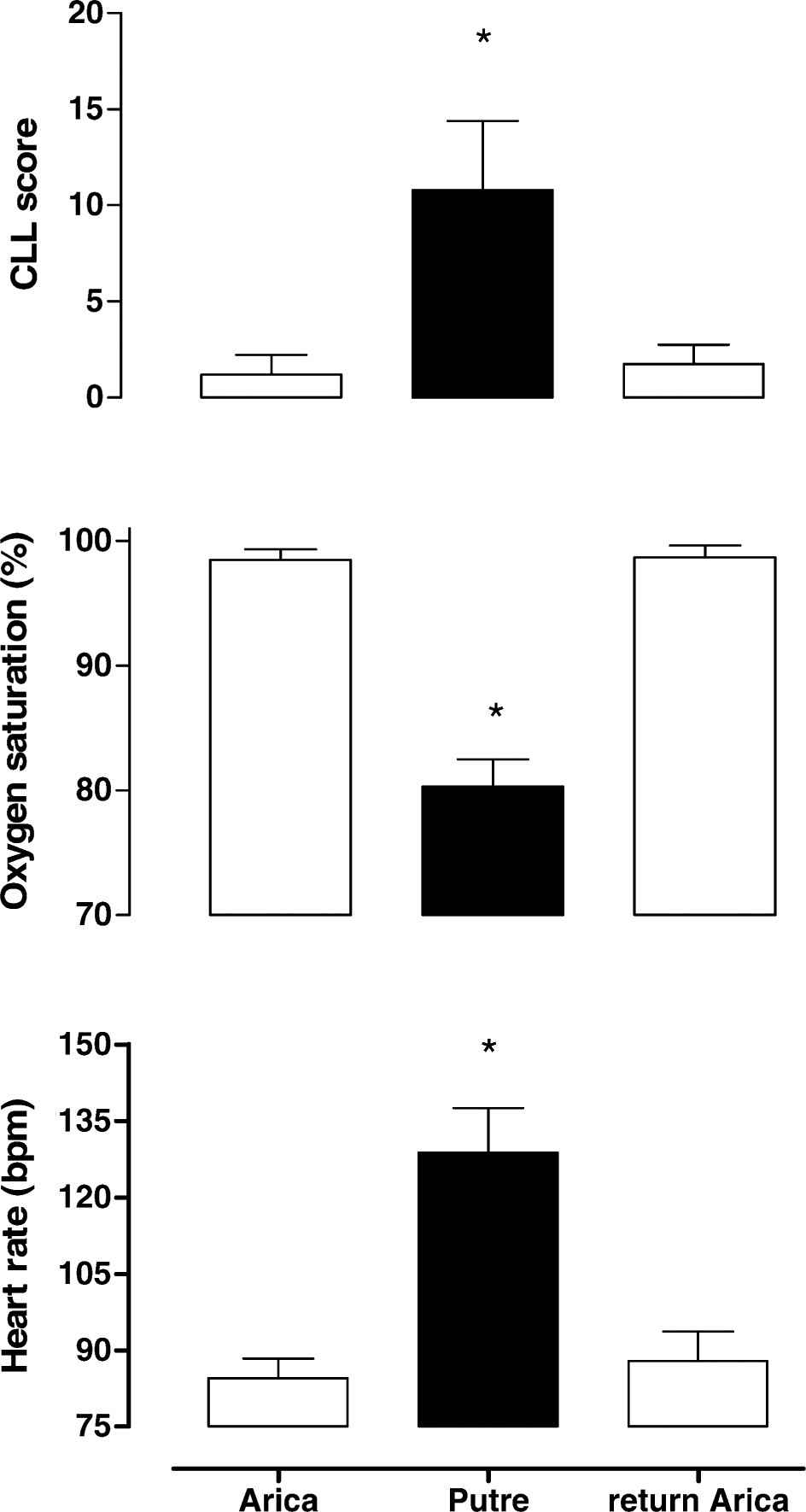
Children's Lake Louise Score (CLLS) (top graph), oxygen saturation (middle graph), and heart rate (beats/min) (bottom graph) for children in this study. White bars represent values of children in Arica (sea level) (at baseline and on return), and black bars represent measurements in Putre (3500 m). Bars represent mean values and brackets represent SD. * indicates significant difference from values at Arica (baseline and on return).
Children's Lake Louise Score, percentage of acute mountain sickness (AMS), and cardiorespiratory response of children and parents at sea level (Arica) and high altitude (Putre) and upon return to Arica†
No difference in AMS using CLLS was associated with gender between males (10.7 ± 3) and females (11.0 ± 4.4), and no difference in AMS using CLLS was associated with age (11.8 ± 3.7; 3–4 years, and 10.8 ± 3.5; 5 years) from observations of children acutely exposed to high altitude.
In this study, no children were observed with saturations lower than 75%. However, 5 children whose oxygen saturation dropped lower than 80% were given oxygen supplementation and after 1 hour were returned to the hotel in Putre.
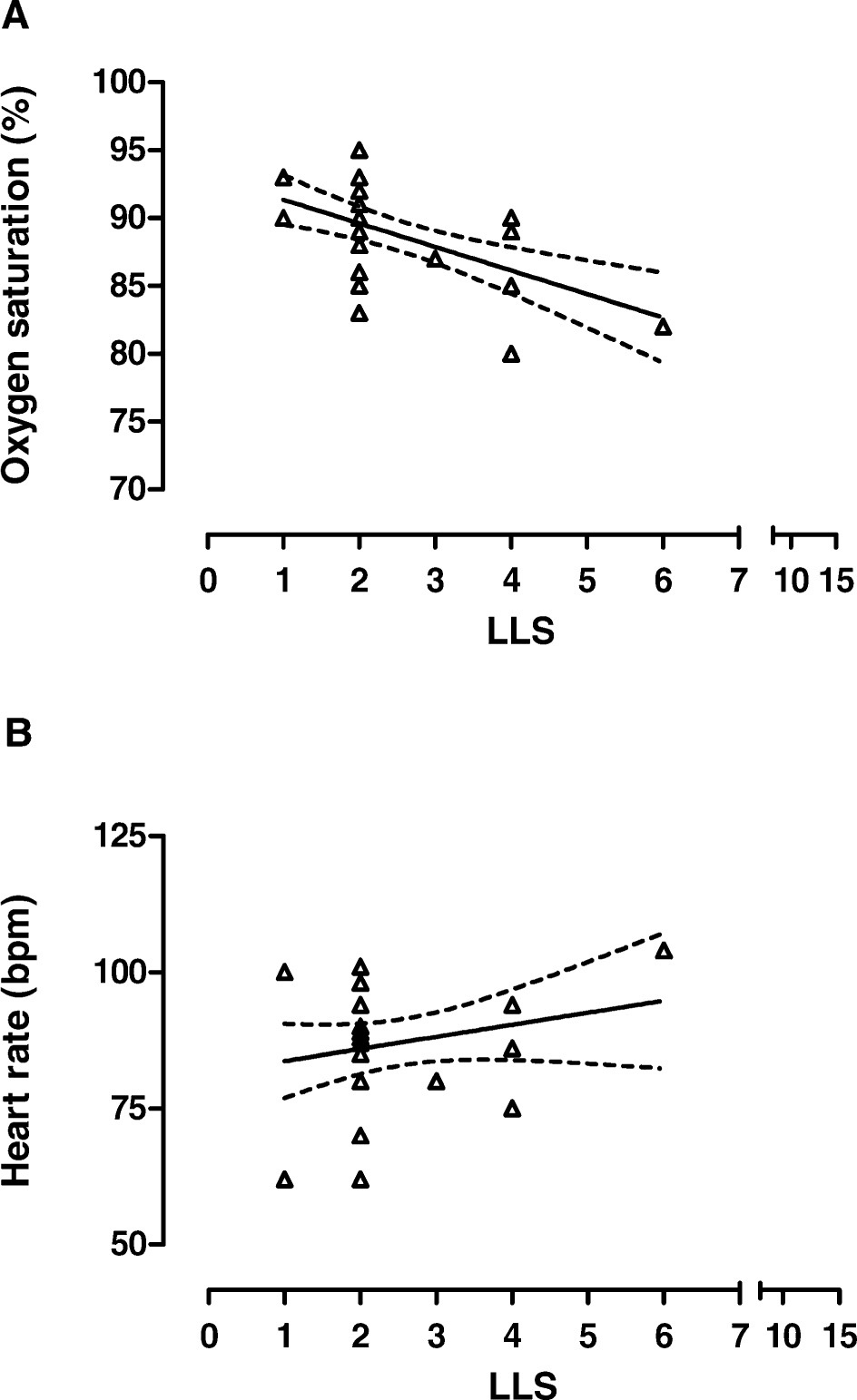
Cardiorespiratory responses and LLS values in parents at sea level (Arica), at high altitude (Putre), and on return to Arica are shown in Table 1. Parents had a lower percentage of AMS and heart rate than children. In contrast, higher oxygen saturation was observed in parents than in children. Furthermore, a negative relationship between CLLS value and arterial oxygen saturation was found (Figure 3A); in contrast, no relationship was observed between CLLS values and heart rate (Figure 3B).
No difference in AMS using LLS was associated with gender between adult males (2.3 ± 0.9) and adult females (2.9 ± 1.6) acutely exposed to high altitude.
Discussion
The likelihood of developing AMS is determined by individual susceptibility, speed of ascent, altitude attained, and previous acclimatization.3,4 It appears from our study that young age may also be a significant risk factor. We found that 3- to 5-year-old children were more likely to develop AMS and to experience significant oxyhemoglobin desaturation than were their parents after an acute ascent from sea level to 3500 m. The children in our study developed a high incidence (94%, 15/16) of AMS. These results agree with our previously reported 100% incidence of AMS in children under 4 years of age and a 25% incidence in parents ascending to the same altitude, 6 indicating that young children may have a higher incidence of AMS than adults.
In contrast, Yaron et al8,10,11 reported a similar incidence of AMS development in children and adults after acute ascent from 1610 m to 3109 and 3488 m. The significant differences between these studies and the current study include the age of the children studied, the simplicity of the language used in applying the CLLS scale, time of exposure to altitude, acclimatization prior to ascent due to altitude of residence, and total ascent distance (starting from sea level or 1610 m). These factors combined or individually may be responsible for differences between these studies and our own.
Normal oxygen saturation in healthy adults at 3500 m is 90% to 91%. 12 Thilo et al 13 reported normal arterial oxygen saturation of 93% to 94% at 1610 m in 3-month-old children, while Niermeyer et al 14 reported saturations of 81% to 91% in 3-month-old children at 3100 m. Yaron et al 11 reported a significant decrease in oxygen saturation, from 95% ± 2% to 91% ± 2%, with a significant increase in the respiratory rate, from 45 ± 13 to 52 ± 15 breaths/min, and without evidence of AMS in children 3 to 36 months of age acutely exposed to 3109 m elevation (from 1600 m).
The physiological mechanism responsible for the observed arterial oxygen saturation in our study could involve one or more of the initial steps in the oxygen transport system: ventilation, pulmonary perfusion, hemoglobin-oxygen affinity, or alveolar-arterial oxygen diffusion.
A decrease in ventilation could explain lower oxygen saturation. Studies performed in children with hypoxic ventilatory response (HVR) demonstrate that they have a higher HVR when compared with adults, 15 –17 supporting age-related differences in response to hypoxia, as previously reported.16,17 However, in newborns, as in adults, oxygen consumption is very sensitive to varying degrees of hypoxia. 18 Hypoxia could induce a depression in HVR in neonates.18,19 This ventilatory depression could explain the lower arterial oxygen saturation. However, the role that this process might play in the depressive phase of the HVR has not been established. 20
A change in pulmonary perfusion could explain lower oxygen saturation. In neonates and adults, alveolar hypoxia in the range of 40 to 80 mm Hg causes vasoconstriction of the resistance pulmonary arteries. 21 In our study, in children acutely exposed from sea level to 3500 m, the low observed arterial oxygen saturation of 80% could also be explained by hypoxic pulmonary vasoconstriction. 14 Hypoxic pulmonary vasoconstriction alters the ventilation/perfusion relationship, reducing systemic arterial oxygenation. 22 This concept is supported by the study of Sime et al, 23 who reported lower oxygen saturation with mild pulmonary hypertension and an increased pulmonary vascular resistance in children under 5 years of age born and living at high altitude. The increased pulmonary vascular resistance was ascribed by the authors to structural changes in small pulmonary arteries and arterioles. 23 Ionic channels appear to play a role in acute hypoxic pulmonary vasoconstriction through activation of calcium channels or inactivation of potassium channels. In chronic hypoxic pulmonary vasoconstriction, ionic channels also play a role in the vascular remodelling that results in chronic pulmonary hypertension. 24
A shift to the right in the oxyhemoglobin-binding curve could explain the lower arterial oxygen saturation. An increase of 2,3-diphosphoglycerate levels remained elevated in adults who were born at high altitude. 25 However, there is no available information on the levels of this chemical in children acutely exposed to high altitude.
A right-to-left shunting may lower arterial oxygen saturation. Persistence of right-to-left shunting across a patent foramen ovale and ductus arteriosus has been documented in people with such congenital anomalies at high altitude. 26 However, all children in our study were born at sea level, without previous experience to high altitude, and parents did not describe any history of cardiopulmonary illness in their children that could explain the lower oxygen saturation observed.
The incidence of AMS observed in parents at this altitude was in agreement with descriptions by other authors,5,6,27 as was the observation that oxygen saturation can be used to predict AMS, 28 given our finding of a negative correlation between LLS score and oxygen saturation. The low occurrence of symptoms of AMS observed in our study reduces the possibility that the parents overestimated symptoms of AMS in their children.
Finally, in our study we observed no difference in AMS associated with gender in children and adults exposed acutely to high altitude. These results agree with those of a study performed in mountaineers and trekkers, which examined risk factors for AMS. 29
Some limitations of the present study must be considered. First, our study included a small number of participants. Despite this, we showed a strong association among AMS, physiological variables (oxygen saturation and heart rate), and high altitude. Future investigations with larger groups of children are warranted. The CLLS is not intended for use in children who are >36 months old. However, it was easy to apply the CLLS, since this avoided inducing responses and/or increasing irritability of the children when asking about symptoms. In a study using the LLS in 4- to 11-year-old children, the participants displayed difficulties in understanding the complex language used in the questionnaire. 30 Our study showed the usefulness of the CLLS in diagnosing AMS in children aged 3 to 5 years. Although the number of participants was small, we observed no difference in CLLS between 3-, 4-, and 5-year-old symptomatic children.
Conclusions
Our results indicate that 3- to 5-year-old children exposed acutely to high altitude are more sensitive to hypobaric hypoxia than are their parents. This was demonstrated by increased symptoms of AMS, significant oxyhemoglobin desaturation, and tachycardia. Young children may experience an exaggerated hypoxemic response to high altitude exposure, and young age may be an additional risk factor for the development of AMS. Our results indicate that physicians, personnel at tourist destinations, and travel agencies should be informed with respect to the potential consequences of children under 5 years of age ascending from sea level to altitudes in excess of 3500 m.
Footnotes
Funding
We are grateful to Mr Aldo Rivera Director of Posta Rural General de Putre, Province of Parinacota, for his support, and to the Universidad de Antofagasta, Chile, for financial support of this study (grant).