
Abstract
Introduction
Individuals ascending to elevations above 2500 m are at risk of developing altitude illness. We sought to establish the incidence and to determine what risk factors, if any, increased the likelihood of developing acute mountain sickness (AMS) in adolescents at Philmont Scout Ranch (PSR) in Cimarron, New Mexico. PSR, with elevations ranging from 2011 to 3792 m, attracts thousands of adolescent participants each year, many of whom arrive from lower elevations with little or no experience ascending to high altitude.
Methods
We conducted a prospective observational study of adolescent participants aged 14 to 19 years who ascended to a minimum of 3000 m while trekking from June to July 2021. Prior to the start of each participant's trek, pretrek survey data were obtained at PSR's basecamp (2011 m). During the trek at 3048 m, the Lake Louise AMS score was used to diagnose AMS.
Results
The incidence of AMS in our study was 13.7%. Participants reporting a history of daily headaches had more than four times the risk of developing AMS. A history of gastrointestinal problems carried three times the risk of developing AMS, and a prior history of AMS increased the risk of developing AMS by 44%.
Conclusions
Our findings enhance our understanding of AMS risk in adolescents and may provide guidance to youth for developing AMS. For individuals with a history of headaches or gastrointestinal problems or a prior history of AMS, there may be an opportunity to reduce the risk of developing AMS.
Introduction
Acute mountain sickness (AMS) is a common illness that occurs in individuals traveling to altitudes greater than 2500 m. Typical symptoms of AMS consist of headache, fatigue, dizziness, and nausea. Although usually mild and resolving without treatment, AMS can progress to life-threatening illnesses that include high altitude cerebral and/or pulmonary edema. Individual AMS risk depends on home elevation, maximum sleeping altitude, latitude, intensity of exercise, arterial oxyhemoglobin saturation, acclimatization, rate of ascent, and preexisting diseases. Its prevalence varies widely and has been observed to be ∼25 to 40% in individuals ascending to moderately high elevations of 3000 to 3500 m.1-4
Adolescents often travel to high elevations to engage in such activities as snow sports, mountain climbing, and hiking. The National Park Service has tracked annual visitations to US National Parks since 1906, and annual recreational visits to all parks have increased substantially since 2009, possibly due to the influence of social media. 5 Youth at altitude lose body water and body mass more than adults. 6 These factors and others may contribute to a higher incidence of AMS in adolescents than in adults.
AMS research traditionally has focused on adult populations. One meta-analysis suggested that age may not play a role in AMS incidence, but the study was limited by heterogeneity of AMS study data, varied methods of ascent, and smaller sample sizes of both children and adolescent study participants. 7 Furthermore, only a minority of the studies included in this meta-analysis reflected the ascent method of trekking to higher altitudes, whereas the majority involved ascent via motorized vehicles (eg, train, bus, and plane). In a study of 107 subjects aged 11 to 12 years trekking from 2179 to 3886 m over Xue Mountain in Taiwan for 3 days, the incidence of AMS was 40.6%. 8 Researchers administered medications to study participants as symptoms arose, and because of this, the incidence and prevalence of AMS may have been underestimated. The difficulty in recruiting minors in high altitude settings often limits the sample sizes available for analysis, and recruiting minors in altitude research is a challenging endeavor.
Philmont Scout Ranch (PSR) is a Boy Scouts of America high adventure youth camp located in the Sangre De Cristo Mountains in Cimarron, New Mexico. PSR hosts multiday backpacking trips (commonly 7–12 days), and participants at PSR begin their trek at base camp (2011 m), where they obtain medical clearance (eg, recheck to ensure that participants meet PSR's requirements for height and weight) and orientation. The maximum reachable elevation while trekking at PSR is 3792 m. With thousands of adolescent participants trekking every year at PSR, the setting serves as an ideal environment to assess AMS in adolescents.
Our study's purpose was to evaluate the incidence of AMS and describe the risk factors attributed to AMS development in a large group of adolescents trekking from 2011 m to a maximum elevation of 3792 m in northeastern New Mexico.
Methods
This prospective observational study used convenience sampling and included 1285 participants between the ages of 14 and 19 years during the summer of 2021 (see Table 1). The study protocol was approved by the institutional review boards at the Mayo Clinic in Rochester, MN, and the Kansas University Medical Center in Kansas City, KS. There were 30 participants who did not consent to participate, 189 who did not complete the survey at high altitude, and 4 who completed the hike on horseback, all of whom were excluded. The remaining 1062 participants were included for analysis.
Responses to the pretrek survey (elevation 2011 m; n=1062).
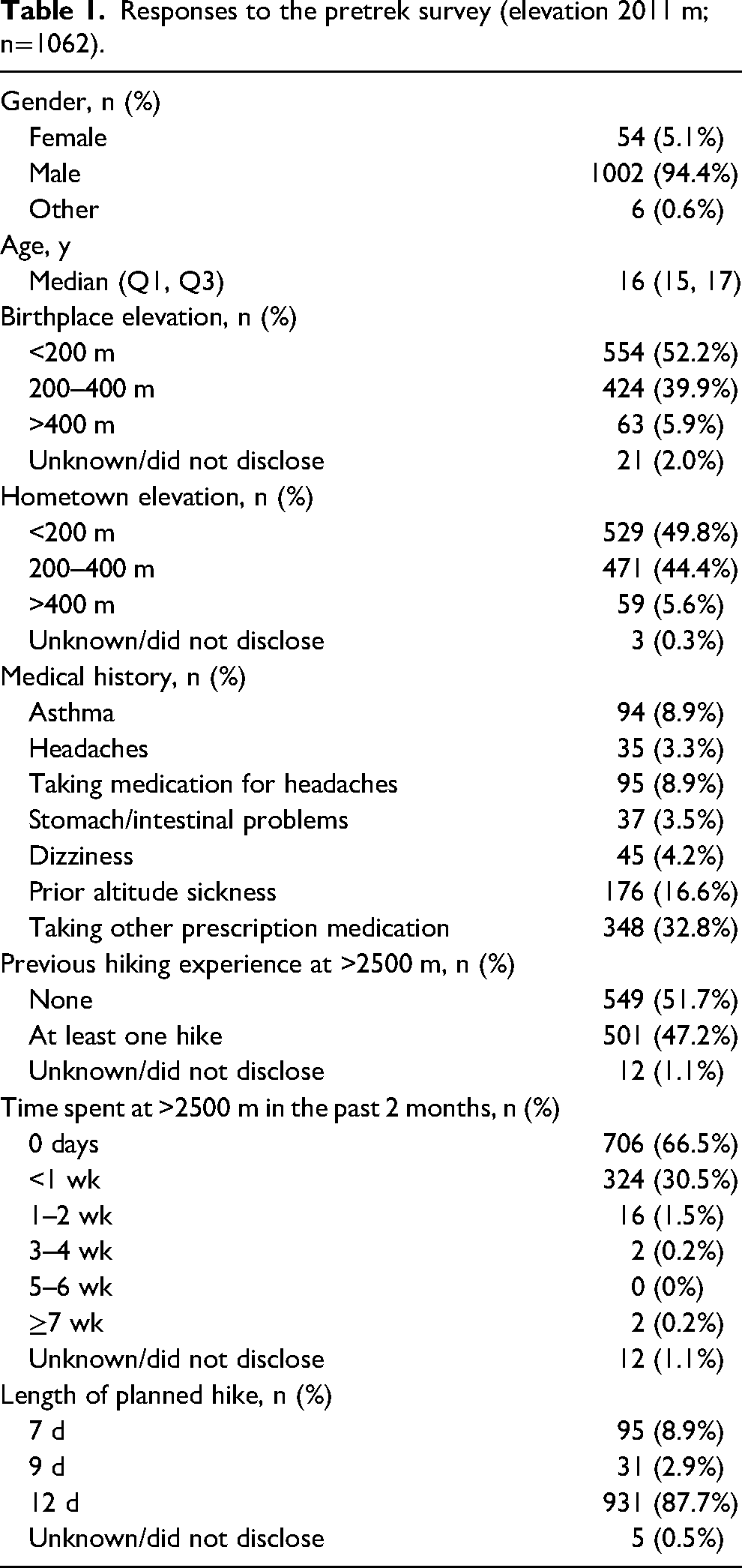
Researchers recruited potential subjects for participation shortly after they arrived at PSR's base camp (elevation 2011 m). After consent was obtained, participants were asked to complete a pretrek survey while at the base camp. The pretrek survey included questions pertaining to each participant's gender, age, past medical history (eg, history of asthma or lung disease; history of daily headaches; use of any medication for the prevention and/or treatment of headaches; and history of dizziness or light-headedness, prior altitude illness, and current medications), hometown, birthplace, experience at altitude >2500 m, and any recent (prior 2 months) exposure at altitude. Each participant was then given a unique numbered tag attached to their backpack for tracking. Researchers again met with study participants at a designated staffed camp called Baldy Town (elevation 3048 m). There they evaluated each subject for AMS using the Lake Louise scoring criteria. 9 Baldy Town was chosen as the location to administer the high altitude survey because it is a common destination for most treks at PSR, where participants can resupply and learn about local history. The Lake Louise scoring criteria were used to assess the incidence and severity of AMS. Participants also completed a high altitude survey at this time, which included questions pertaining to time spent at current altitude, medication use, and whether or not there were any changes to their preassigned trek itineraries and travel plans. Using each participant's unique numbered tag, survey responses obtained from base camp were matched to those from Baldy Town. Vital sign measurements (ie, blood pressure, pulse, respiratory rate, and oxygen saturation) were performed at the base camp and at Baldy Town. Oxygen saturation was captured using the FS20C Finger Pulse Oximeter (Hunan Accurate Bio-Medical Technology, Hunan, China). Survey data were transcribed into Research Electronic Data Capture Software and subsequently analyzed.
Statistics
Numerical survey questions are summarized with means, standard deviations, medians, and interquartile ranges. Multiple-choice questions are summarized with frequency counts and percentages.
Potential risk factors for AMS were assessed using the pretrek survey. Participant demographics, significant past medical history, and altitude experience were compared between participants who experienced AMS on their hikes and participants who did not experience AMS. Continuous features were compared using Wilcoxon rank-sum tests, and categorical features were compared using χ2 tests or Fisher’s exact tests. Differences are expressed using risk ratios (RRs) with 95% CIs.
Additionally, the association between pretrek risk factors and AMS was assessed using multivariable least absolute shrinkage selection operator (LASSO)–penalized logistic regression. Participant demographics, medical history, medications, hiking experience, and pretrek vitals all were included for analysis. This penalized regression approach allows us to minimize the risk of overfitting our data when considering many predictors, which is a concern for standard regression approaches. Model results are reported as odds ratios with 95% CIs.
Participant vital signs obtained at the base camp and at Baldy Town were compared using paired-sample Wilcoxon signed-rank tests. Tests were two sided, and P values of <0.05 were considered significant. All analyses were performed using R version 4.1.2.
Results
Most study participants identified as male (94.4%, n=1002) and reported their hometown elevation as <400 m (94.2%, n=1000). The incidence of asthma, chronic headaches, and prior altitude illness was 8.9% (n=94), 3.3% (n=35), and 16.6% (n=176), respectively. Table 1 summarizes responses to the pretrek survey. Table 2 summarizes responses to the Baldy Town survey, including the results of the Lake Louise scoring. The most common medications taken prior to the hike were cetirizine (7.3%, n=77), ibuprofen (5.6%, n=59), albuterol (2.5%, n=27), and acetaminophen (2.4%, n=26). The overall incidence of AMS in our study population was 13.7% (n=146).
Responses to the Baldy Town survey (elevation 3048 m; n=1062).
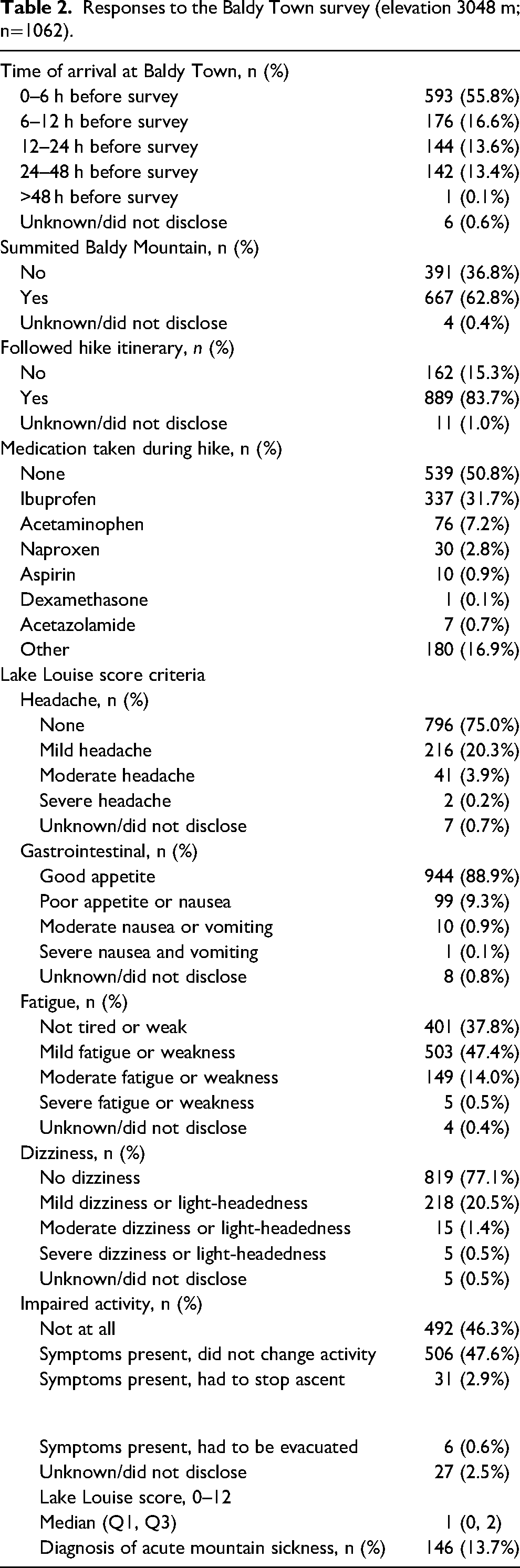
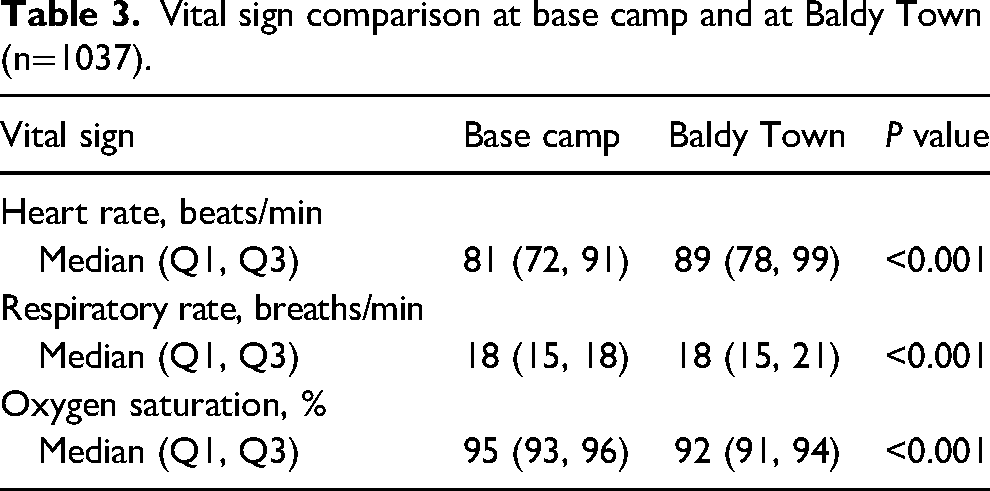
Table 3 compares vital sign measurements at the base camp and at Baldy Town. There was an eight-point increase in heart rate (measured in beats per minute) and a three-point drop in the arterial hemoglobin oxygen saturation. Of the 1285 participants in our study, only 1037 with complete vital signs measured at the base camp and at altitude were included in this comparison.
Vital sign comparison at base camp and at Baldy Town (n=1037).
A total of 146 participants (13.7%; 95% CI, 11.8–16.0%) met Lake Louise scoring criteria for AMS during their hikes, as shown in Table 2. Table 4 assesses potential risk factors for AMS by comparing participant demographics, medical history, and altitude experience between participants who experienced AMS on their hikes and participants who did not experience AMS. Participants reporting daily headaches had more than three times the risk of AMS compared with participants without headaches (RR=3.35; 95% CI, 1.97–5.27; P<0.001). Similarly, participants reporting a history of gastrointestinal problems had twice the risk of AMS (RR=2.47; 95% CI, 1.37–4.46; P<0.001), and a history of AMS increased the risk of developing AMS by 47% (RR=1.47; 95% CI, 1.01–2.16; P=0.035). History of asthma (RR=0.92; 95% CI, 0.51–1.66; P=0.77) and dizziness or light-headedness (RR=1.66; 95% CI, 0.87–3.15; P=0.093) did not affect the risk of developing AMS during the hike.
Associations between potential risk factors and acute mountain sickness.
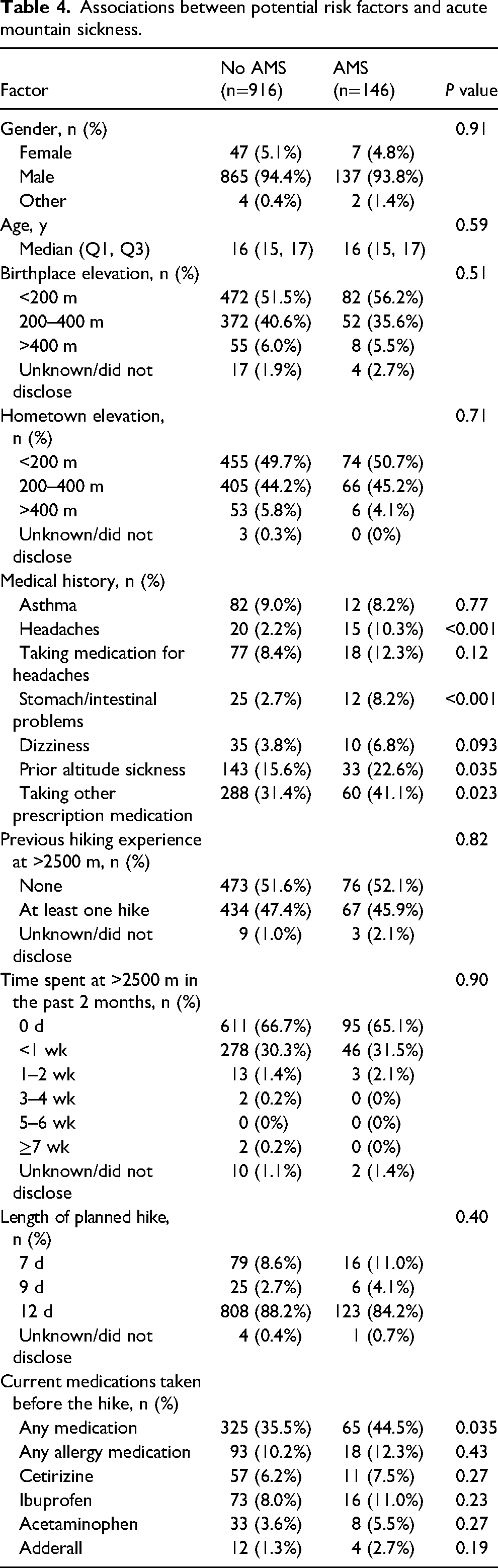
Hikers taking any prescription medications or medications for headache were at higher risk for developing AMS (RR=1.38; 95% CI, 1.00–1.92; P=0.035). However, no specific medication affected the risk for AMS. Additionally, previous experience with hikes above 8200 m (P=0.82), recent time spent over 8200 m (P=0.90), and length of trek (P=0.40) did not change the risk for AMS.
Using a LASSO-penalized logistic regression model accounting for all potential risk factors, we found that a history of daily headaches (odds ratio [OR]=5.34; 95% CI, 2.57–11.12; P<0.001) or stomach or intestinal problems (OR=2.23; 95% CI, 1.02–4.87; P=0.045) and prior diagnoses of altitude sickness (OR=1.62; 95% CI, 1.04–2.50; P=0.31) were statistically significant predictors of developing AMS on the hike. All other predictors were not statistically significant at P>0.05.
A sensitivity analysis excluded all participants who reported a history of headaches or gastrointestinal issues prior to the hike. Following the same LASSO-penalized procedure as before, we again found that a prior diagnosis of altitude sickness was a statistically significant predictor of developing AMS during the hike (OR=1.66; 95% CI, 1.04–2.67; P=0.035). No other risk factors were significantly associated with AMS (P>0.05 for all).
Discussion
This study sought to evaluate the incidence of AMS in adolescents hiking at high altitudes and to identify characteristics that might increase the risk for developing AMS. Previous studies evaluating AMS in adolescents have been smaller and over shorter durations.10-17 This study expands on both of those factors.
Our study found the overall incidence of AMS in adolescents hiking at high altitudes to be 13.7%. The difference between our study and prior studies may be due to a larger sample size, better acclimatized participants, or overall lower altitudes encountered by participants. PSR participants are acclimatized by hiking to higher altitudes rather than by vehicle transportation to high altitude, as previous studies have described.18-20 Also, PSR participants are strongly encouraged to complete pretrek physical conditioning before arriving at PSR. They receive education and guidance pertaining to proper hydration and adequate nutrition. They are acclimatized to an altitude of 2000 m while spending 2 to 3 days at a base camp prior to their hike. Individuals who have a prior medical history of headache and preexisting gastrointestinal problems may have a greater likelihood of scoring positive for AMS using the Lake Louise score. Furthermore, individuals who have a prior self-reported history of AMS also have an increased likelihood of developing AMS again. These factors might be classified as preexisting conditions. It is difficult to determine whether this may represent an exacerbation of a chronic problem or the creation of a new problem. Nevertheless, an individual who is experiencing the symptoms of AMS may have a limited ability to hike at high altitude without the development of new or worsened symptoms. We did not assess whether such symptoms impact the individual’s quality of life. In other words, we did not ask participants if they still enjoyed hiking despite having symptoms.
Limitations
This study has several limitations. First, our base camp and Baldy Town surveys were completed by each participant, and inevitably, recall bias is introduced with any self-assessment tool. The same is true of medication use, and it is possible that some participants may not have recalled or wished to disclose all the medications available to them. We did not ask participants questions regarding medication adherence or dosing regimens and are therefore unable to comment on the effects of medication or dosing on the likelihood of any of the events we observed. Our question pertaining to stomach/intestinal problems on the survey was purposely worded in a vague manner to permit a broad range of responses, but it may not have captured all the gastrointestinal ailments in our study population.
Second, although we believe that the number of participants with severe symptoms who left the trail without completing their treks and the Baldy Town survey was small, we were unable to assess the number of participants who did so. These participants were excluded from our analysis.
Third, although our research did not account for longer acclimatization periods that may have occurred, we believe that some groups may have spent additional time at the base camp elevation to allow for a greater acclimatization period prior to the onset of their treks. As a result, it is possible that we may have missed an important variable that may have decreased the incidence of AMS in our study population. We evaluated many other factors that did not appear to impact the development of AMS. For example, individuals who self-reported a prior history of asthma, dizziness, or vertigo and specific medication use did not change the likelihood of any individual's development of AMS. Understanding factors that do and do not contribute to the development of AMS is equally important in targeting which youth participants need guidance in preparing to hike at high altitudes.
Conclusions
Most adolescent participants in our study did not develop AMS while hiking at high altitude. For individuals with headaches, gastrointestinal problems, or a prior history of AMS, there may be an opportunity to prepare them prior to hiking at high altitude to reduce the risk of developing AMS. Further study should focus on specific interventions that may reduce the development of AMS for these individuals and may include lifestyle modifications such as longer acclimatization, use of specific medications for preemptive treatment of symptoms, hydration strategies, or rest strategies. In addition, further study could focus on managing AMS symptoms once they develop such that participants can continue to hike successfully at high altitude.
Footnotes
Acknowledgments
We thank Nate Lay, Rich Barth, Steve Nelson, and the Philmont Infirmary and backcountry staff for their assistance and support.
Author Contribution(s)
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was supported by Grant Number UL1 TR002377 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.