
Abstract
Objective
There have been few studies evaluating snakebite mortality in Venezuela and South America. In this study we evaluate trends in fatal snakebites occurring in Venezuela between 1995 and 2002.
Methods
Epidemiological data for this study were retrieved from the records of the Ministry of Health of Venezuela. Using these data, we analyzed the impact of snakebites in Venezuela during the study period.
Results
During the study period, there were 266 reports of death due to snakebite; 79.7% were males, and 20.3% were females (P < .01). Annual mean deaths numbered 33 per year. Of total deaths, 24.1% occurred in victims 55–70 years old. Deaths in young children (<5 years old) accounted for 7.1% of the total. Mortality rate by age showed an age-dependent rate, with higher rates in older ages (P = .038).
Conclusion
Snake envenomations are an important cause of injury and deaths in Venezuela as in many American countries. Surveillance of envenomations is essential for establishing guidelines, planning therapeutic supplies, and training medical staff on snakebite treatment, as well as assessing risk zones for travelers.
Introduction
Venomous and poisonous animals are a significant cause of global morbidity and mortality. 1 In the case of venomous snakes, these are found throughout most of the world, including many oceans, and have evolved a variety of highly effective toxins and methods of delivery.1,2 Their impact on humans is considerable, most current data suggesting they cause in excess of 3 million bites per year, with more than 150,000 deaths. Particularly in the rural tropics, snakebite morbidity and mortality is a significant human medical and economic burden. The major groups of snakes causing bites are the vipers (family Viperidae), the elapids (Elapidae, eg, cobras), the sea snakes (Hydrophidae), the side-fanged vipers (Atractaspidae), and the back-fanged colubrids (Colubridae).1,2 Although snakebites are rare in some countries, they present challenging and growing problems in many others. In Venezuela, as well as in other countries of South America, bites occur more commonly in jungle regions than in other ecological regions (Figure 1). Like many other tropical and wilderness traumatic illnesses, snakebites are reported more commonly in males living in risk areas, but the incidence in travelers has increased in recent years.3,4
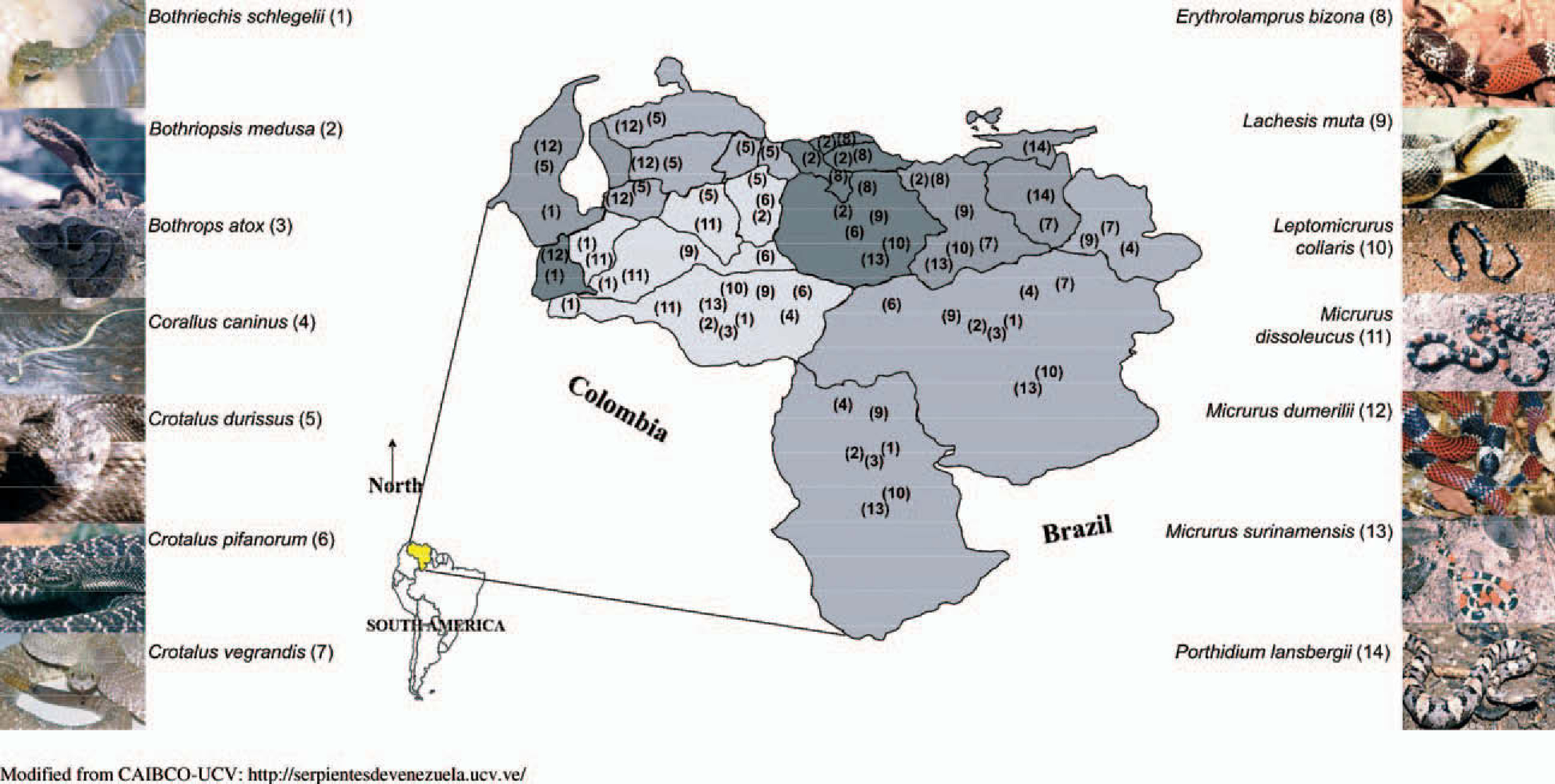
Relative position of Venezuela and a list of most important snake species distributed in the country
In a recent study done in Goias, Brazil, from 1998 to 2000, the authors reported 3261 accidents caused by venomous snakes, with a case fatality rate of 0.46%. 5 In a previous study in the same country, between 1989 and 1996, the authors found a total of 1576 accidents in the state of Amazonas, with a mortality of 1%. 6 In another Brazilian study in Rio Branco, Acre, based on an evaluation of 144 patients admitted with snakebites in the year 2002, no deaths were recorded. 7 During 1999, 17 704 snakebites occurred in this country, corresponding to a rate of 10.4 cases per 100 000 population. 5 –7
In the setting of few studies about mortality due to snakebites in other countries of South America, the objective of this report was to evaluate the trends in fatal snakebites in Venezuela between 1995 and 2002.
Methods
Epidemiological data for this study were retrieved from the records of the Ministry of Health of Venezuela. With these data, an analysis of snakebite impact in Venezuela during the study period was performed. Morbidity data were inadequate at the national level to perform further analyses beyond the primary analysis, and the objective of this report was to evaluate the trends in snakebite mortality in Venezuela between 1995 and 2002. We reviewed all mortality records from the Ministry of Health of Venezuela, using ICD-9 and ICD-10 codes to search for all deaths due to snakebites during the study period. Mortality records were compiled from the regional records of the whole country (24 states). Each of these records integrated information from the municipalities’ health offices (the basic level of administrative health reporting). Each death due to snakebite was classified in the record according to the age and gender of the individual.
In Venezuela, snakebites are officially reportable, but, in practice, it is more of a voluntary registry, a cause for underreporting of morbidity. Conversely, all cases of deaths are specifically and obligatorily reportable, and mortality information is more available and accurate.
Data were statistically processed to assess the importance, features, and trends of fatal snakebites in Venezuela, a country with considerable diversity of snake species (Figure 1). Chi-square and F tests were used for comparison of quantitative and qualitative variables, respectively, and P values less than .05 were regarded as significant.
Results
For this period, 266 patients died from snakebites in Venezuela. The mean number of annual deaths was 33.3 ± 7.5 per year. This figure did not vary significantly during the study period (r2 = .1628, F = 1.17, P = .322). The mortality rate ranged from 0.1 deaths per 100 000 population (in 1997) to 0.2 deaths per 100 000 population (in 2001) (Figure 2a).
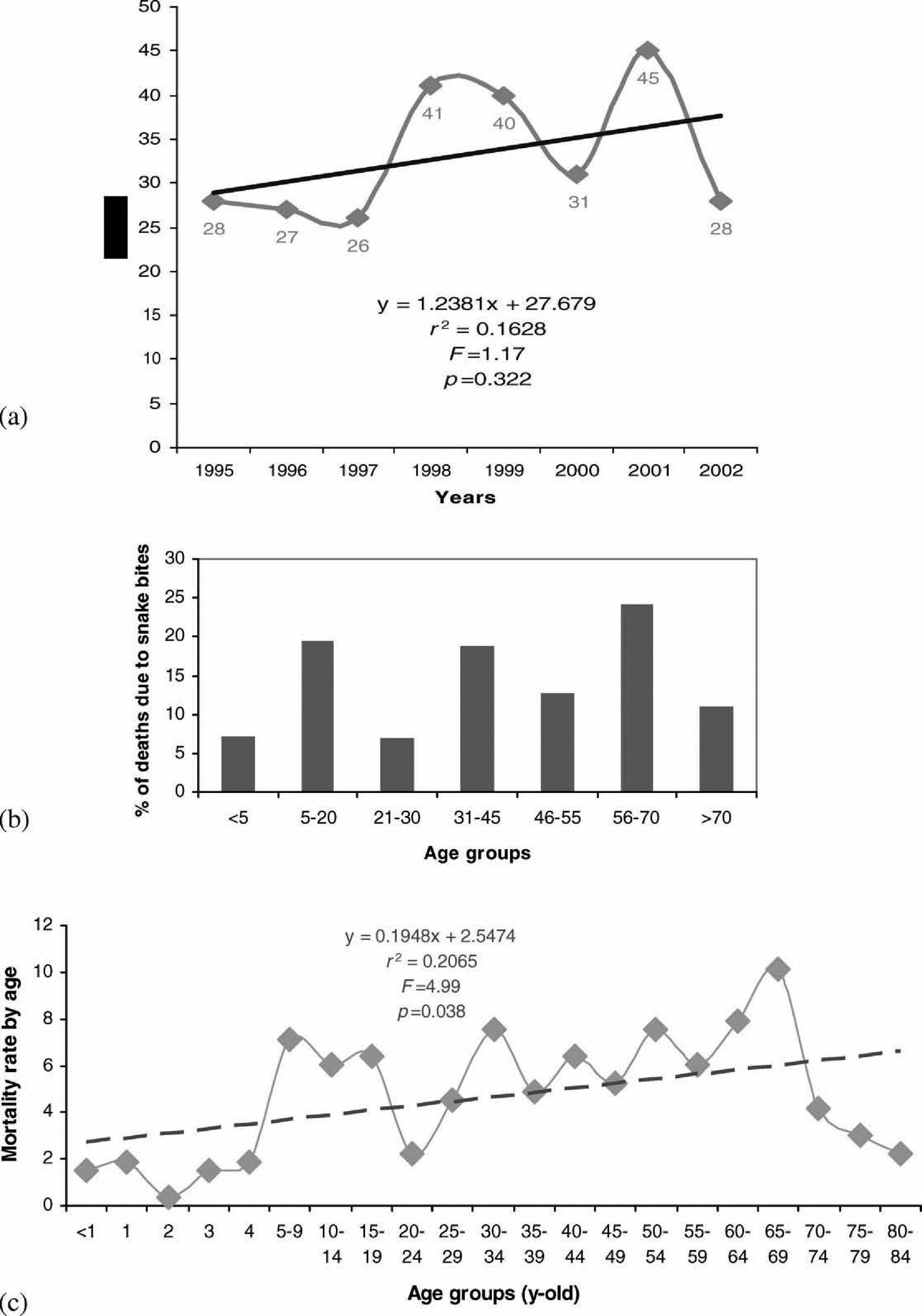
Deaths due to snakebites in Venezuela during years 1995-2002.
The gender distribution was 79.7% males and 20.3% females (P < .01). The age distribution showed that deaths occurred in 24.1% of the group of 55- to 70-year-olds, 19.5% of the group of 5- to 20-year-olds, and 18.8% of the group of 30- to 45-year-olds (P = .27) (Figure 2b). Deaths in young children (<5 years old) were recorded in 7.1% (Figure 2b). Mortality rate by age showed an age-dependent tendency, with higher rates in older ages (r2 = .2065, F = 4.99, P = .038) (Figure 2c).
Discussion
Envenomations, particularly due to snakes, are a significant cause of injury in Venezuela, as in many American countries. As we see here, the year-to-year number of deaths due to snakebites appears to be slightly increasing, perhaps indicating better reporting of deaths caused by this problem. It is possible, however, that there is still significant underreporting of this condition.
Venomous-snakebite mortality in Venezuela varies in different age groups, with the highest peak in the group of 55- to 70-year-olds, representing a quarter of deaths due to this cause. This may be related to significant occupational exposure in the rural Venezuelan environment for older farmers still working in the fields. Also, although not reported herein, cardiovascular diseases in this age group are a significant comorbidity that may contribute to mortality when envenomations occur.
In Venezuela the main causes of death are cardiovascular diseases, which represent 21.33% of the causes for the year 2002, followed by cancer with 15.65% and violent deaths (suicides and homicides) with 7.96%.
Although data collected for this report lack specific information related to morbidity caused by snakebite, due to problems in the surveillance and recording of nonfatal injuries, this is the first study showing an analysis of mortality due to snakebites in the country, and one of the few reports from the region, other than Brazil, Ecuador, and Colombia.8,9 In Ecuador, each year 1200 to 1400 cases of snakebites are reported in 19 of the 21 provinces, which is why new epidemiological and therapeutic studies are being conducted in that country. 8 In Colombia, approximately 3000 snakebites are reported every year. 9 In other countries, such as Peru and Costa Rica, snake envenomations are considered a public health problem, but there is a paucity of specific data and epidemiological reports. 10 A preliminary report from Venezuela previously described the mortality due to invertebrate and vertebrate envenomations in one eastern state (Monagas State) and reported 20 deaths due to snakebites during the period 1980–2000. 11 In Venezuela, antivenom is widely availabile, particularly in the north-central capital region and the southern jungle region, but knowledge related to its proper use is variable due to a lack of uniform criteria for the management of snakebites in rural areas.
The true global incidence of envenomation, and the severity thereof, remains largely misunderstood, except for a few countries where these accidents are rare or are accurately reported. 12 We acknowledge, based on other sources of information (personal communication with physicians in rural areas), that presented data are only a partial record of mortality due to snakebites, and that venomous snakebite likely causes a high burden in terms of morbidity and even mortality that deserves further evaluation. Nevertheless, this information is the basis for further morbidity and mortality surveillance studies. Currently, in some states of the country, surveillance and further attention to these cases are being applied in order to reduce snakebite-related mortality. Nevertheless, more epidemiological evaluation and patient health education, as well as training of medical providers, regarding the prevention and management of snakebite-related morbidity and mortality are necessary.
Additionally, it is essential that more data be collected in order to develop guidelines for dealing with snakebites; plan drug supplies, particularly antivenom; and train medical staff on snakebite treatments, including supportive care. Antivenom offers a specific therapy that can significantly reduce the effects of envenomation and reduce mortality in severe cases. Largely neglected to date is the impact of snake envenomation as a cause of significant long-term disability in developing countries. 13 Furthermore, given the increased incidence of snakebites in travelers in recent years,3,4 snakebite epidemiology studies will provide important information for travel medicine practice and pre-trip advice to travelers.
Since the comprehensive review by Swaroop and Grab in 1954, no global, systematic survey has been carried out on snakebite epidemiology. 12 For this reason, studies on morbidity and mortality related to venomous snakebite must be continued.
Footnotes
*
This work was previously presented in part at the XVIth International Congress for Tropical Medicine and Malaria, the IVth European Congress on Tropical Medicine and International Health, and the VIIe Congrès International de la Société de Pathologie Exotique, September 11–15, 2005, Marseille, France (Oral presentation, O-042, pp 38).