
Abstract
Objective
The duration of tick attachment is related to the likelihood of disease transmission. To be able to locate and remove an attached tick is important.
Methods
Sixty-seven patients presenting with tick bites to the Karadeniz Technical University emergency department and 3 different first-stage health institutions between April and July 2006 were investigated to determine the distribution of the bites.
Results
Tick attachment site distribution was determined as follows: 9% head-neck, 5% arm, 24% stomach-groin, 7% back, 18% chest-shoulder, 25% leg-foot, and 12% hip.
Conclusions
According to the results of our study, 20% of ticks attach to regions of the body that patients cannot themselves see. After travel in endemic areas, a complete inspection of the entire body surface is required to achive early tick removal
Introduction
Tick bites are becoming an increasing source of visits to emergency departments and first-stage health clinics in Turkey. Bites by tick species from the genus Hyalomma have recently led to widespread and fatal cases of Crimean-Congo hemorrhagic fever (CCHF). Ticks are arthropods, with an external skeleton and jointed legs. Within this phylum they are arachnids, which belong to the subclass acari and are related to mites. There are 2 main tick families that have been discovered. 1 There are 700 species of Ixodidae, or hard ticks, and 185 species of Argasidae, or soft ticks. 1
Tick bites may result in the transmission of diseases to humans. In North America, the following diseases are caused by tick bites: Lyme disease, human granulocytic and monocytic ehrlichiosis, babesiosis, relapsing fever, Rocky Mountain spotted fever, Colorado tick fever, tularemia, Q fever, and tick paralysis. In Europe, the list is similar, but the occurences of other diseases have been reported as well. 2 These include boutonneuse fever (caused by a less virulent spotted fever rickettsial organism, Rickettsia connori) and tick-borne encephalitis. 2
CCHF has now also become a major tick-borne illness causing significant mortality and morbidity in the Balkans, including a part of Turkey. CCHF also occurs in the Caucasus, the Central Asian republics, Iran and Middle Eastern countries, as well as various African countries, including the Democratic Republic of Congo. 3 According to data from the Turkish Ministry of Health, 500 cases of CCHF in Turkey between 2002 and 2005 were reported, with a 5.2% mortality rate. 3
The duration of tick attachment is related to the likelihood of disease transmission. 4 –6 Finding the site of tick attachment is indispensible in the diagnosis and treatment of tick paralysis. 7
It was the goal of this study to evaluate patients presenting with tick bites to the Karadeniz Technical University (KTU) emergency department and 3 first-stage health clinics to determine the relative order of attachment sites on patients’ bodies.
Methods
Physicians at the KTU Emergency Department and 3 different first-stage health clinics in the province of Maçka completed forms on each patient presenting with a tick bite between April and June 2006. Physicians at the local medical clinic and at the emergency departments completed forms given to them reporting age, gender, and bite sites. We determined by subsequent chart review whether or not the patients developed tick-related diseases.
Results
During the study period, 67 patients presented with tick bites. Thirty-six (53.7%) of the patients were female, and 31 (46.3%) were male. Mean age ± SD was 41.43 ± 18.9 years, ranging from 4 to 82.
The distribution of attachment sites in cases presenting to the 3 medical facilities for the 4 months between April and July 2006 was as follows: 9% head-neck, 5% arm, 24% stomach-groin, 7% back, 18% chest-shoulder, 25% leg-foot, and 12% hip (Figure). Three of the patients who presented with tick bites were later admitted to a hospital with a diagnosis of CCHF. There were no deaths.
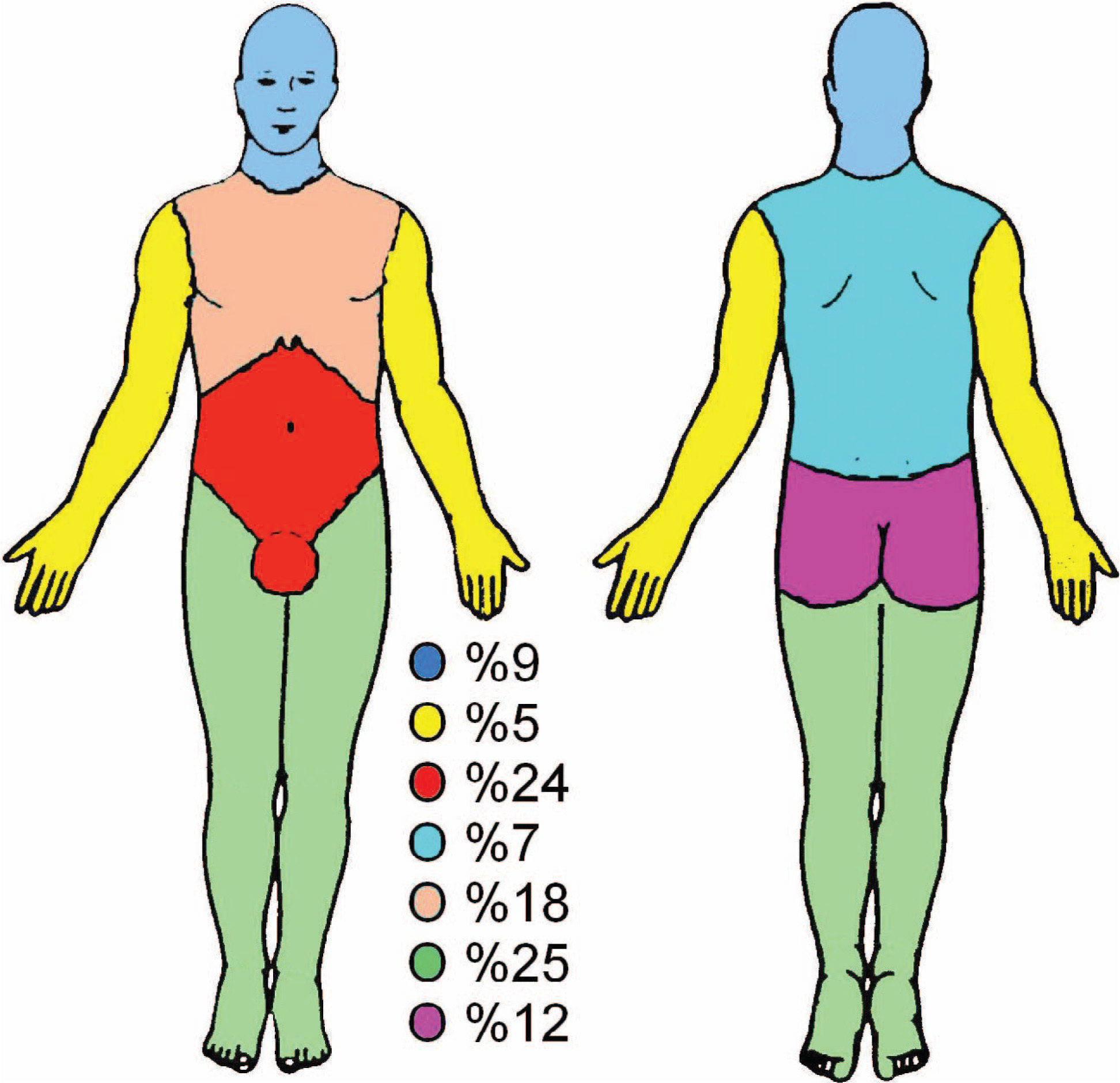
Distribution over the body of tick attachment sites.
Discussion
Amblyomma, Dermacentor, and Ixodes are the three genera of hard ticks that transmit diseases to humans in the United States. These ticks generally feed for many days, a fact that has some bearing on the treatment of tick bites. 2 Some ticks secrete an adhesive material to fasten themselves to the host. In addition, Ixodes ticks secrete anticoagulant, immunosuppressive, and anti-inflammatory substances into the area of the tick bite. These substances presumably help the tick to obtain a blood meal without the host becoming aware of the bite. There may only be a little redness around the area of the bite. These same substances also help any pathogens carried by the tick to cause an infection in the host. 2 The species of biting ticks were not identified in our study; however, we know from other studies that the ticks present in this part of Turkey are of the family Ixodidae, genus Hyalomma (Hyalomma marginatum Koch., H. anatolicum Koch., H. margintum rufipes C. L. Koch., H. impeltatum Schulze & Schlottke, H. impressum Koch., H. truncatum Koch.). 8
Tick paralysis is a disease in which the site of tick attachment is of paramount importance. The diagnosis of tick paralysis is made by a combination of clinical features including finding a tick embedded in the skin and observing clinical improvement after tick removal. There are no other diagnostic tests that directly confirm the diagnosis of tick paralysis. The species most often associated with tick paralysis in the United States and Canada are Rocky Mountain wood tick (Dermacentor andersoni) and the American dog tick (D. variabilis); however, 43 ticks species have been implicated in human disease around the world. 7
Tick paralysis is thought to be caused by a toxin secreted in tick saliva during feeding that reduces motor neuron action potentials and the action of acetylcholine. Symptoms usually occur after 4 to 7 days of tick feeding. Ascending flaccid paralysis progresses over several hours or days; there are no sensory changes, and there is no pain. The paralysis usually resolves within 24 hours of tick removal. When the tick is not removed, the mortality rate resulting from respiratory paralysis is approximately 10%. 7
While ticks may be recovered from anywhere on the body, the distribution of the blacklegged tick is more uniform, while most American dog ticks (Ixodes scapularis) are removed from the head and neck. Over one third of I. scapularis have been recovered from the legs and arms. Another third were removed from the back, shoulder, neck, and head. 5
In our study, the most common attachment sites were the lower extremities, followed by the lower abdomen-genital region, then the posterior wall of the thorax, and the gluteal region in that order. The attachment site was in a location not visible to the victim in around 20% of cases.
In studies regarding Lyme disease, which is transmitted through tick bites, a significant correlation was found between tick attachment duration and risk of contracting that disease. 5 It was reported that the risk of Borrelia burgdorferi from an infected feeding nymph of I. scapularis increases dramatically after 48 hours of attachment. 4 –6,9,10 Early removal of an attached tick will reduce the likelihood of transmission of Lyme disease. During the first 24 hours of tick attachment, there is no transmission. By 48 hours of feeding, the transmission rate in one study was only 12.5%, although by 72 hours the transmission rate increased to 75%. Transmission rate by an infected tick is almost 100% after 4 days and full engorgement.4,6,9,10
Conclusions
In conclusion, attached ticks cause very few acute symptoms and are largely identified by direct visual detection. According to our study, attachment to regions of the body not visible to the victims themselves occurred approximately 20% of the time. For this reason, physical inspection of individuals who have been in areas of possible contact with ticks in endemic regions is important. The body should be scanned using a mirror or with the assistance of another person to inspect areas the at-risk individual cannot see directly.