
Abstract
Background
Hypothermia is a frequent complication of cold weather exposure and/or wilderness injuries. Anecdotal reports have postulated that patients suffering from acute hypothermia are at significantly increased risk of developing lethal cardiac dysrhythmias secondary to the physical stimulation from moving and transporting patients.
Objective
To develop a model to attempt to determine if rough handling and sudden movement can induce lethal cardiac dysrhythmias in a controlled animal study of mild to severe hypothermia.
Methods
Ten anesthetized swine had continuous cardiac and invasive blood pressure (BP) monitoring. Core body temperature (CBT) was measured with an esophageal probe. Animals were secured to a backboard in a supine position for the duration of the study and their CBT was serially lowered by external cooling measures. At preset intervals (every 3°C lowered from the baseline CBT of 38°C), the animals were lifted via the backboard and rolled 90 degrees to the left and held for 5 seconds and then rolled to the right and held for 5 seconds. After rolling, the swine were lifted via the backboard 6 inches off the surgical table and dropped back onto the table, and after 15 seconds this was repeated at 12 inches. If no signs of dysrhythmia were noted, external cooling was continued. Data were analyzed by tests of proportion on mortality associated with hypothermia and mechanical stimulation. To determine whether hypothermia and mechanical stimulation were independent effects, a one-sided McNemar's test of matched pairs was employed.
Results
No animal developed a dysrhythmia at a CBT > 25°C with or without stimulation. Fifty percent of the animals developed fatal dysrhythmias (3 ventricular fibrillation, 2 asystole) with no stimulation but at CBT ≤ 25°C (average CBT 22.7°C). Twenty percent (2/10) developed fatal dysrhythmias (ventricular fibrillation) during mechanical stimulation. For hypothermia, a binomial test of the observed proportion 0.70 (fatality during hypothermia) against a hypothetical proportion of 0 (no fatality in the absence of hypothermia) yielded P < .001 with power = 1.00. For mechanical stimulation, a binomial test of the observed proportion 0.20 (fatality from mechanical stimulation); against a hypothetical proportion of 0 yielded P < .001 with power = 1.00. The test of matched pairs yielded P < .037, indicating that the variables of mechanical stimulation and hypothermia jointly caused mortality.
Conclusion
Profound hypothermia induces fatal dysrhythmias both with and without mechanical stimulation in a swine model.
Introduction
Hypothermia is a frequent comorbid condition of patients treated in the Emergency Department. Cardiac rhythm disturbances are a frequent complication of acute hypothermia and a source of significant morbidity and mortality in this patient population. 1 –4 Mechanical trauma occurring during the movement or treatment of hypothermic victims has long been implicated as an etiology of ventricular dysrhythmias, most notably ventricular fibrillation, but the evidence is anecdotal and observational. 5 –9 As a consequence, it has become common practice to exercise caution when transporting and providing emergency care to hypothermia victims in order to provide as little physical stimulation as possible to the patient. This may impact the efficiency and effectiveness of care provided.
The belief that the hypothermic heart is susceptible to a fatal ventricular dysrhythmia with mechanical stimulation from patient movement or transport has been preserved in the textbooks and the literature since it was first put forth by Negovskii in 1962. 10 It gained wider support in 1973 when Lloyd alluded to the association in his report on hypothermic patients caused by cold weather exposure. 11 The article explicitly urged extreme caution when handling hypothermia victims to avoid inducing cardiac arrest, though no supporting rationale was offered.11,12 From a review of the literature, it appears that the association of physical stimulation with life-threatening cardiac dysrhythmias in hypothermic patients has never been studied. We attempted to develop a controlled animal model of mild to severe hypothermia to determine whether rough handling and sudden movement induces lethal cardiac dysrhythmias.
Methods
This study protocol was approved by the US Naval Medical Center Animal Care and Use Committee. The care and handling of animals was in accordance with National Institutes of Health guidelines for ethical animal research.
A porcine model of hypothermia was chosen for this study because swine have previously been used as a model for the human cardiovascular system and have also been employed to simulate human physiologic responses to hypothermia.13,14
Ten immature swine weighing 33–38 kg were sedated with a 5 mg/kg intramuscular injection of a 1:1 ratio of xylazine (100 mg/kg) and a combination of tiletamine and zolazepam (Telazol: 100 mg/kg). The animals were endotracheally intubated, and mechanical ventilation was initiated at a rate of 8 breaths/minute, with a tidal volume of 15 mL/kg. These parameters were adjusted to maintain an end-tidal P
Central venous access was obtained through the external jugular vein to allow intravenous fluid administration. The common carotid artery was cannulated with a 16-gauge catheter and used to measure mean arterial pressure. Pulse rate was continuously monitored by a lead II electrocardiogram. An esophageal temperature probe was placed for continuous core temperature monitoring. Each animal received 15 mL/kg of normal saline intravenously over a 30-minute period before baseline variables were obtained.
Each pig was secured to a backboard in a supine position for the duration of the study. Baseline core body temperature (CBT) for the study was defined as 38°C. Baseline parameters including cardiac rhythm, heart rate (HR), mean arterial pressure (MAP), and pH were obtained. The animals were then lifted via the backboard and rolled 90 degrees to the left and held for 5 seconds and then rolled to the right and held for 5 seconds. After rolling, the swine were lifted via the backboard 6 inches off the surgical table and dropped back onto the table, and after 15 seconds this was repeated at 12 inches. Observations were made at each position for alterations in cardiac rhythm. If no signs of dysrhythmia were noted within 2 minutes of the completion of the stimulus, external cooling was begun. External cooling was accomplished with a cooling blanket placed between the animal and the backboard and surrounding the animal with bags filled with ice and water. At preset intervals (every 3°C lowered from the baseline CBT of 38°C), the procedure was repeated and data recorded. Cooling was continued until the animal's CBT reached 20°C or upon the development of a fatal dysrhythmia. Upon completing the protocol at 20°C or upon development of a terminal rhythm the swine were euthanized.
As this was a pilot study, it was not possible to perform antecedent power analysis to determine optimal sample size. Hypothetical calculations employing tests of proportion on mortality associated with hypothermia and mechanical stimulation indicated that a sample size of 10 should be adequate to find a result of statistical significance. To determine whether hypothermia and mechanical stimulation were independent effects, a one-sided McNemar's test of matched pairs was employed.
Results
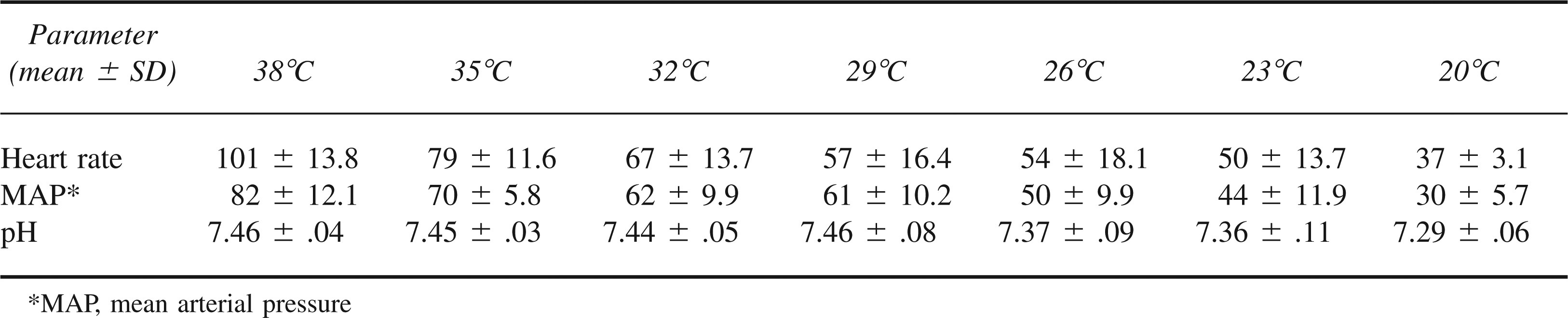
The weight (mean ± SD) of the animals was 36 ± 1.8 kg. Heart rate, MAP, and pH over time are represented in Table 1. Length of time to cool the swine before reaching the next data collection point along with the number of surviving swine at that point are presented in Table 2.
Heart Rate, Mean Arterial Pressure, and pH (mean ± SD) for Preset Temperature Intervals
The amount of time (mean ± SD) needed to cool the animals from one preset core body temperature to the next. The number of surviving animals after reaching each preset temperature is noted in parentheses

No animal developed a dysrhythmia at a CBT > 25°C with or without stimulation. Fifty percent of the animals developed fatal dysrhythmias (3 ventricular fibrillation, 2 asystole) while lying supine between data collection points and not in a temporal association with mechanical stimulation. All of these animals were severely hypothermic with a CBT ≤ 25°C (average CBT 22.7°C). Twenty percent (2/10) of the swine developed fatal arrhythmias (ventricular fibrillation) during mechanical stimulation but not until CBT was 20°C. Both animals were noted to be in ventricular fibrillation after the final 12-inch drop. Three animals survived to the conclusion of the study without developing a fatal rhythm.
The effects of hypothermia and mechanical stimulation on fatality were analyzed using tests of proportion. For hypothermia, a binomial test of the observed proportion 0.70 (fatality during hypothermia) against a hypothetical proportion of 0 (no fatality in the absence of hypothermia) yielded P < .001 with power = 1.00. For mechanical stimulation, a binomial test of the observed proportion 0.20 (fatality from mechanical stimulation) against a hypothetical proportion of 0 yielded P < .001 with power = 1.00. A one-sided McNemar's test of matched pairs yielded P < .037, indicating that the variables of mechanical stimulation and hypothermia jointly caused mortality.
Discussion
Accidental hypothermia is a frequent comorbid condition in patients presenting to the Emergency Department. 17 These patients are often treated with extreme care to minimize rough handling secondary to the belief that such handling might induce a fatal dysrhythmia. Although there are hypothetical reasons that support this concept,5,14 there has never been a study specifically addressing the hypothesis.
Hypothermia has been defined as a CBT below 35°C.1,18,19 Severity of hypothermia is somewhat arbitrary but has been broken down to mild (35°C to 32°C), moderate (32°C to 28°C), and profound (≤28°C). The physiologic manifestations of hypothermia are pervasive, with progressive cardiovascular, neurologic, and respiratory changes as the body cools.1,2,4,19 The body's initial response to falling CBT is to increase the metabolic rate, clinically manifested by tachycardia, tachypnea, and shivering as temperatures fall below 36°C. However, as cooling continues, shivering ceases by 31°C and progressive bradycardia and respiratory depression predominate. Progressive depression of the central nervous system also leads to dysarthria, ataxia, stupor, and eventual loss of electrical brain activity below 20°C. The most common fatal endpoint is a cardiac dysrhythmia, most notably ventricular fibrillation. 4
In our controlled porcine model, we found that profound hypothermia directly leads to fatal dysrhythmias in at least 50% of the animals. Further, we noted fatal dysrhythmias immediately following mechanical stimulation during profound hypothermia in another 20% of the animals. Interestingly, no dysrhythmias were noted in any of the animals until they reached temperatures of 25°C, whether they were undergoing intense mechanical stimulation that we defined as rough handling or not. Although our numbers were small, this suggests that animals with mild to moderate hypothermia are not at risk for developing fatal dysrhythmias either from the direct effects of the hypothermia or from the rough handling applied at these temperatures. For profoundly hypothermic patients, our study lends preliminary support to anecdotal reports that mechanical stimulation, in conjunction with low CBT, may induce fatal dysrhythmias.
The question of why profoundly hypothermic myocardium is subject to the induction of these dysrhythmias remains unclear. We followed HR, MAP, pH, and cardiac rhythms over time to see if they would correlate with the susceptibility to dysrhythmia. We noted progressive bradycardia and a marked decrease in MAP and pH over time, all of which could have predisposed the animals to the development of dysrhythmias. On the cardiac rhythm strips, there were flattened/inverted T waves and widening of the QRS intervals that might indicate changes in Na+/K+/Ca++ gradients. These changes may have been exacerbated by the progressive acidosis noted as the animals became increasing hypothermic. However, in none of our animals was there any evidence of increased automaticity or premature complexes prior to the development of the fatal rhythm.
Given the results of our pilot study, and until a more definitive study is done, we would recommend that emergency services personnel continue to treat profoundly hypothermic patients with the utmost care and try to limit the amount of mechanical stimulation prior to rewarming. As patients become increasingly hypothermic, the susceptibility of the myocardium to dysrhythmias may increase.
Limitations
There are multiple limitations to this study, including the possibility that our animal model might not reproduce the human effects of mild to severe hypothermia. We chose the swine model because it has been used in previous investigations of hypothermia and assessment of cardiovascular function.14,20 The rate of temperature change that we employed may not represent cases of hypothermia in humans secondary to exposure but was comparable to other studies and anecdotal reports of hypothermia. We also chose to use external cooling to try to mimic what may be seen in the wilderness. However, swine skin and its response to a cold stimulus may be different than in humans and may have worsened the acidosis seen in this model. The small sample size limits any definitive conclusions or extrapolation. The fact that 20% of the animals developed dysrhythmias temporally related to rough handling during profound hypothermia supports our current practice and limited anecdotal evidence for gentle handling of the profoundly hypothermic patient. In addition, the animals were anesthetized with isoflurane which may increase cardiac sensitivity. We chose the anesthesia based on previous studies that demonstrate minimal cardiac effects but could not rule this out as a potentiator for cardiac dysrhythmias.
Conclusions
Hypothermia induces fatal dysrhythmias. Mechanical stimulation in conjunction with profound hypothermia in a swine model may induce fatal dysrhythmias.
Footnotes
*
The Chief, Bureau of Medicine and Surgery, Navy Department, Washington, DC, Clinical Investigation Program, sponsored this report #S-02-104 as required by NSHSBETHINST 6000.41B. The views expressed in this article are those of the authors and do not reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. government.