
Abstract
Background
The development of comorbidities has become increasingly relevant with longer-term cancer survival.
Objective
To assess the pattern of comorbidities among Australian women with breast cancer treated with tamoxifen or an aromatase inhibitor.
Design
Retrospective cohort study using Pharmaceutical Benefits Scheme (PBS) data (10% sample) from January 2003 to December 2014. Dispensing claims data were used to identify comorbidities and classified with the Rx-Risk-V model. The breast cancer cohort had tamoxifen or an aromatase inhibitor dispensed between 2004 and 2011 with no switching between types of endocrine therapy. Comparisons were made between the breast cancer cohort and specific control groups (age- and sex-matched at 1:10 ratio without any dispensing of anti-neoplastic agents during the study period) for the development of five individual comorbidities over time using Cox regression models.
Results
Women treated with tamoxifen had a higher incidence of cardiovascular conditions, diabetes, and pain or pain-inflammation, but a lower incidence of hyperlipidaemia compared with non-cancer control groups, as indicated by PBS data. Women treated with aromatase inhibitors were more likely to develop cardiovascular conditions, osteoporosis, and pain or pain-inflammation compared with non-cancer control groups. The risks of hyperlipidaemia and osteoporosis were significantly lower among tamoxifen users compared with aromatase inhibitor users.
Conclusions
Women with hormone-dependent breast cancer treated with an endocrine therapy had a higher risk of developing specified comorbid conditions than women without cancer, with different comorbidity profiles for those on tamoxifen versus aromatase inhibitors. Further research into the causes and mechanism of development and management of comorbidities after cancer is needed.
Keywords
Introduction
Breast cancer is the most common cancer reported among Australian women and around 70% of cases are hormone-responsive, requiring treatment with hormonal therapies, such as tamoxifen and aromatase inhibitors (AIs [anastrozole, letrozole, and exemestane]) [1,2]. The choice of endocrine therapy is determined by several factors including women's menopausal status, pre-existing comorbidity, differences in efficacy, and tolerance [3–5]. A recent Australian study has shown that tamoxifen was more often selected as an initial therapy in women with osteoporosis as the use of AIs has been associated with an increased risk of bone loss [5]. Conversely, the use of tamoxifen has been linked to an increased risk of thromboembolic events, and clinicians may hesitate to initiate tamoxifen in people with a history of deep vein thrombosis, pulmonary embolism, or stroke [4,6].
In addition to pre-existing comorbidities at the time of cancer diagnosis, breast cancer patients are also at risk of developing new chronic diseases, which may arise as a result of cancer treatment or cancer complications [7,8]. Using drug dispensing as a surrogate for the presence of comorbidities, we have previously shown that comorbid diseases, such as cardiovascular conditions, depression, diabetes, gastric acid disorders, osteoporosis, and pain or pain-inflammation, were more likely to develop after cancer in women with hormone-dependent breast cancer who have been exposed to one or more types of endocrine therapy compared with women with no breast cancer history [9]. However, there is limited comparative information on the differences in the pattern of comorbid diseases associated with the different types of endocrine therapy.
In the present study, we aimed to assess whether the development of new comorbidities varied according to the type of endocrine therapy received. We compared the development of five common chronic diseases over time: (i) between breast cancer women treated with any endocrine therapy (tamoxifen or AI) and women without cancer; (ii) between breast cancer women treated with tamoxifen and women without cancer; (iii) between breast cancer women treated with an AI and women without cancer; (iv) between breast cancer women treated with tamoxifen and breast cancer women treated with an AI.
Methods
Data Source
This retrospective cohort study used de-identified dispensing claims data from the Pharmaceutical Benefits Scheme (PBS), which represents a random 10% sample of Australians (approximately 3 million Australians) over a period of 12 years from 2003 to 2014. All PBS-subsidized medications are captured in the dataset and coded with the PBS schedule item codes and World Health Organization Anatomical Therapeutic Chemical code [10].
Breast Cancer Cohort
Women with hormone-dependent breast cancer were identified by the dispensing of at least one supply of endocrine therapy between January 2004 and December 2011. The use of dispensing records as a proxy measure for hormone receptor status has previously been validated in the Australian setting [11]. The following inclusion criteria were applied in the selection of breast cancer cohort: (i) incident users of either tamoxifen or an AI (anastrozole or letrozole) who had the first dispensing of endocrine therapy anytime from January 2004 onwards, with no switching between different types of endocrine therapy throughout the study period, as we were interested in assessing whether the development of new comorbidities varied according to the type of endocrine therapy received; (ii) concessional beneficiaries to ensure more complete capture of medicine use, given that dispensing records for medicines priced below the general co-payment level in the general beneficiaries were not available in the PBS dataset before April 2012. Concessional beneficiaries are individuals who are qualified to receive government benefits, including pensioners and people with lower incomes, and account for most medicine use in Australia. These patients entitle a lower co-payment threshold (AUD 6.40 per subsidized medicine in 2018). Women treated with exemestane were excluded as it is only subsidized for metastatic breast cancer. Details on the proportion of initial cohort lost due to the exclusion criteria are presented in Supplementary Figure 1.
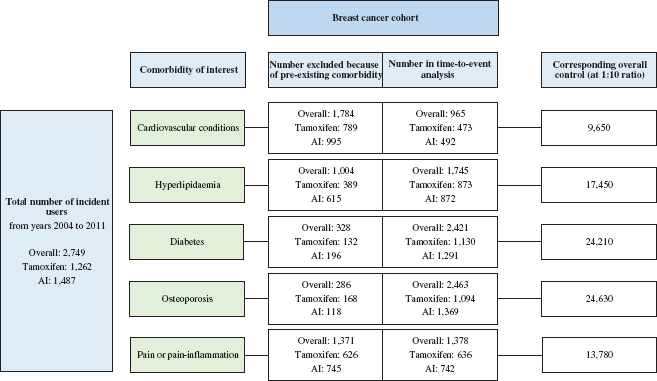
Number of women with breast cancer and their corresponding control groups for each type of comorbidity evaluated. AI, aromatase inhibitor.
The index date was defined as the first dispensing date of endocrine therapy. The breast cancer cohort was split into two groups based on the endocrine therapy received: (i) tamoxifen; (ii) AI (anastrozole or letrozole).
Comorbidity Score and Individual Comorbidities
The Rx-Risk-V model [12] was chosen as the comorbidity index. The Rx-Risk-V model was calculated using up to 40 general drug categories (Supplementary Table 1) as determined by the World Health Organization Anatomical Therapeutic Chemical Code classification. The Rx-Risk-V model was employed using pharmaceutical dispensing records as surrogate for the presence of comorbidity, given that the information of diagnoses in the outpatient settings is not usually available in Australia. It has previously been validated in the Australian setting with the prediction of 1-year mortality shown to be comparable to predictions using the Charlson Comorbidity Index [13,14]. Baseline comorbidities (i.e. measured over a 12-month period before the index date) for each study population were determined and a score was assigned using the Rx-Risk-V model.
Five individual comorbidities were assessed, given their significant contribution to the burden of disease in Australia: cardiovascular conditions (identified through medications indicated for arrhythmias, heart failure, hypertension, ischaemic heart disease, angina, anticoagulant, and antiplatelet medicines), diabetes, hyperlipidaemia, osteoporosis, and pain or pain-inflammation. The analysis involved the creation of five datasets – each for a specific comorbidity of interest where the comorbidity of interest was not present at baseline. Women with the presence of the individual comorbidity of interest at or before the initiation of endocrine therapy were excluded from the time-to-event analysis for that particular individual comorbidity evaluated as an outcome.
Control Group
For each of the five datasets of interest, a separate control group (women without the individual comorbidity of interest measured over a 12-month period before the assigned index date and without any medication dispensing records of anti-neoplastic agents and endocrine therapy throughout the study period identified from the PBS sample) was matched by age at a 1:10 ratio. This means that there were five independent non-cancer control groups selected for the five individual comorbidity datasets evaluated (Figure 1). Women included in the control groups were concessional beneficiaries with at least one medication dispensing record for the year where the index date was assigned matching with the year of endocrine therapy initiation of the corresponding case.
All the eligible cases and controls were followed up to 31 December 2014, which is the end of study period for the assessment of the development of comorbidity of interest over time. People who developed the individual comorbidity of interest were considered to have an event, while those who did not have the event were censored at their last dispensing record available (up until 31 December 2014). As the date of death was not available in this dataset, the last dispensing record was used as the follow-up end date.
Statistical Analysis
Descriptive analyses and Cox regression models with effect estimates expressed as hazard ratios (HRs) with 95% confidence intervals were presented for the two groups: the overall cancer group and non-cancer control group. Analyses were repeated by comparing the breast cancer groups based on the type of endocrine therapy (tamoxifen versus AI) and with their corresponding non-cancer control group. We used the stratified Cox regression models to account for the matched pairs given that matching was done with respect to age at index date between cancer and non-cancer control group. The models were adjusted for selected individual baseline comorbid conditions and number of baseline comorbidities (measured over a 12-month period before the assigned index date) identified through the Rx-Risk-V model. Adjustment for age using a late-entrant Cox model was applied for the comparison between breast cancer women treated with tamoxifen and breast cancer women treated with an AI. We also assessed the proportional hazard assumption by including the interaction between study groups and follow-up time in the Cox regression model. When the HR varied over time, HRs were computed separately for each year since cohort entry. All analyses were performed using SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Cohort Characteristics
A total of 2,749 women, who had been dispensed with an endocrine therapy for the first
time between 2004 and 2011 and with no switching between the types of endocrine therapy
throughout the study period up to 31 December 2014, were identified (Figure 1). Of those, 1,262 were treated with tamoxifen
and 1,487 with an AI. The most prevalent comorbidities identified at baseline were
cardiovascular conditions (65%,
The breast cancer cohorts included in the time-to-event analysis were followed up for a median ranging from 2.6 years (quartile range [QR]: 1.0–4.6) for pain or pain-inflammation to 4.9 years (QR: 3.2–7.2) for diabetes (See Supplementary Table 2). Similarly, the control groups were followed up for a median ranging from 3.0 years (QR: 1.3–5.0) for pain or pain-inflammation to 5.0 years for diabetes (QR: 3.2–7.2) and osteoporosis (QR: 3.0–7.0). The majority (ranging from 75% to 88% depending on the types of comorbidity) of women with breast cancer were aged 55 years and older.
Comorbidity
Cardiovascular Conditions
The risk of developing new cardiovascular conditions was higher in the overall cancer group, tamoxifen, and AI subgroups, when each was compared with the non-cancer control groups (Table 1, Figure 2). The risks of cardiovascular conditions (in the overall cancer group and AI subgroup) were highest in the first year and declined thereafter. The result became non-significant from the fifth year onwards in the AI subgroup. There was no significant difference between the types of endocrine therapy (tamoxifen compared with AI).
Hazard ratios (95% confidence intervals) for the incidences of selected types of comorbidity in four settings

AI, aromatase inhibitor; HR, hazard ratio (comparison vs. control group).
Adjusted for number of baseline comorbidity and selected comorbid condition at baseline: (i) cardiovascular conditions, adjusted for presence of diabetes and hyperlipidaemia at baseline; (ii) hyperlipidaemia, adjusted for presence of cardiovascular conditions at baseline; (iii) diabetes, adjusted for presence of cardiovascular conditions at baseline.
Adjustment of age using late-entrant Cox model.
Significant p<0.05.
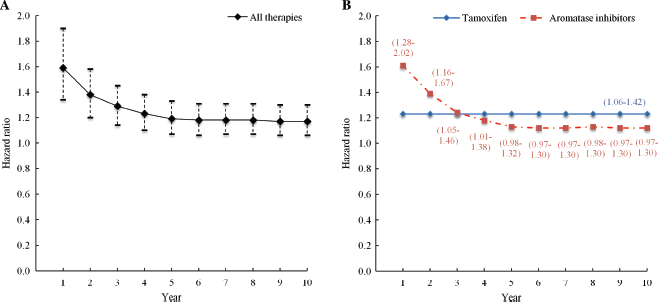
Incidence of cardiovascular conditions in women with breast cancer versus non-cancer control group over time since cohort entry. A: Incidence in overall cancer group. B: Incidence stratified by type of endocrine therapy. Data are hazard ratios with 95% confidence intervals shown by dotted lines (A) or in parentheses (B). Data were adjusted for number of baseline comorbidities and presence of diabetes and hyperlipidaemia at baseline.
Hyperlipidaemia
The risk of developing hyperlipidaemia was lower in the tamoxifen subgroup compared with the non-cancer control group and AI subgroup, respectively.
Diabetes
The risk of developing diabetes was higher in the overall cancer group compared with the non-cancer control group. Women treated with tamoxifen had a significantly higher risk of developing diabetes compared with the non-cancer control group, but there was no statistically significant difference between the types of endocrine therapy (tamoxifen compared with AI).
Osteoporosis
The risk of developing osteoporosis (Figure 3) was higher in the overall cancer group and AI subgroup, when each was compared with the non-cancer control group. The risks of osteoporosis in the overall cancer group and AI subgroup declined over time, while the risk was significantly lower in the tamoxifen subgroup compared with the AI subgroup.
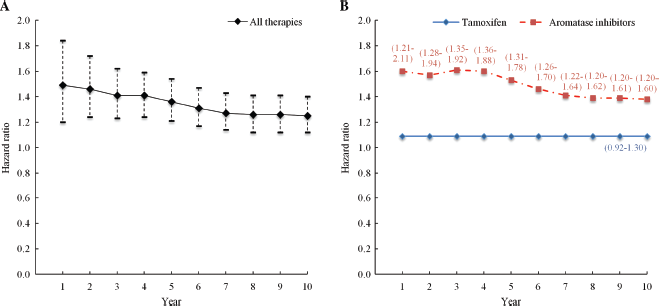
Incidence of osteoporosis in women with breast cancer versus non-cancer control group over time since cohort entry. A: Incidence in overall cancer group. B: Incidence stratified by type of endocrine therapy. Data are hazard ratios with 95% confidence intervals shown by dotted lines (A) or in parentheses (B). Data were adjusted for number of baseline comorbidities at baseline.
Pain or Pain-Inflammation
The risk of developing pain or pain-inflammation was higher among the overall cancer group, tamoxifen, and AI subgroups, when each was compared with the non-cancer control groups. There was no significant difference between the types of endocrine therapy (tamoxifen compared with AI).
Further details on the incidence rates by types of comorbidities in women with and without breast cancer included in our study are presented in Supplementary Table 3.
Discussion
Our results show that the risks of developing cardiovascular conditions, diabetes, osteoporosis, and pain or pain-inflammation were higher in the breast cancer cohorts compared with the control groups. These results are similar to those of our previous study, which included all women irrespective of the endocrine therapy received (monotherapy or switch between endocrine therapies) [9]. This study provides further insights into the differences in the pattern of development of comorbid conditions associated with the use of AIs or tamoxifen. AI users were more likely to develop cardiovascular conditions, osteoporosis, and pain or pain-inflammation than women without cancer. Tamoxifen users had a higher incidence of cardiovascular conditions, diabetes, and pain or pain-inflammation than women without cancer. The risks of osteoporosis and hyperlipidaemia were significantly lower among tamoxifen users compared with AI users.
Cardiovascular conditions
The development of cardiovascular conditions is a major concern for breast cancer survivors as they are the primary cause of death in older women with breast cancer [15]. Although the risk of developing cardiovascular conditions was higher in both the AI and the tamoxifen groups compared with the control groups, we found no significant difference between the AI and tamoxifen subgroups. These results differ from those observed in clinical trials, where AIs have been found to be associated with a 19% higher risk of cardiovascular diseases than tamoxifen in the adjuvant setting [16]; but they are consistent with those of a recent large population-based study that did not find a higher risk of serious cardiovascular events (myocardial infarction, angina, stroke) in AI users than in tamoxifen users [17]. In both observational studies, women had no prior cardiovascular disease and might have been at lower risk than women enrolled in clinical trials. Comparisons with other studies are also limited by the differences in the definition of cardiovascular conditions. In our study, the dispensation of cardiovascular medicines was used as a surrogate measure of cardiovascular comorbidity, but we were not able to further differentiate the subtype of conditions, such as cerebrovascular disease, thromboembolism, or coronary heart disease.
Differences in the cardiovascular impact of AIs and tamoxifen may be explained either by a reduction in the protective effect of oestrogens on the cardiovascular system by AIs or by the protective effect of tamoxifen, possibly through alterations in serum lipid levels and a reduction in low-density lipoprotein cholesterol [18–20]. Confirming these findings, our results show that women in the tamoxifen subgroup had a lower risk of hyperlipidaemia compared with both the control group and the AI subgroup.
A higher risk of cardiovascular conditions in breast cancer survivors may also be due to the common risk factors shared between breast cancer and cardiovascular disease, such as physical inactivity, obesity, and excessive alcohol consumption [1,8,21]. A higher incidence may also be caused by cardiotoxicity from selected breast cancer treatments, such as anthracyclines, trastuzumab, and radiotherapy [22], or increased detection resulting from enhanced healthcare provided to cancer survivors [23,24].
Diabetes
The risk of starting an antidiabetic medicine was higher in both AI and tamoxifen users than in the control groups, but it was not statistically significant for the AI subgroup. We found no significant difference between the tamoxifen and AI subgroups. There were mixed results found in the literature. A Canadian case–control study and a cohort study conducted in Taiwan showed an association between the use of tamoxifen and an increased risk of diabetes [25,26]. However, an American study found no evidence of increased risk of diabetes associated with the use of AI or tamoxifen [27]. The underlying mechanism and the effects of endocrine therapy on diabetes onset remain to be explored. A higher risk of diabetes among the breast cancer survivors may be due to common risk factors [28] and increased healthcare use coinciding with care of breast cancer [23,24]. A Canadian study showed that incidence of diabetes among breast cancer survivors may be increased, particularly in those who received adjuvant chemotherapy [29]. Greater diabetes screening and prevention among breast cancer survivors may therefore be warranted.
Osteoporosis
The risk of developing osteoporosis, as shown in our study by the increased dispensing of an antiresorptive treatment as the surrogate for osteoporosis, was higher in the AI subgroup compared with the non-cancer group and with the tamoxifen subgroup. This suggests a bone-protective effect associated with tamoxifen compared with AIs. Tamoxifen is known to stabilize the bone mineral density in post-menopausal women [30], while the use of AIs has been associated with an increased risk of bone loss and fractures [4,30]. It has been postulated that a reduction in the protective effect of oestrogens by AIs leads to an increase in markers of bone resorption. Bone loss occurs at a higher rate (by 2–3 fold) among AI users compared with the healthy age-matched postmenopausal controls [30,31]. The findings of our study further support the policy of periodic assessment of bone mineral density among postmenopausal women receiving AIs for fracture prevention [4,32]. It must be noted that the increased risk of osteoporosis with AIs compared with tamoxifen was observed even though women with pre-existing osteoporosis might have been less likely to commence anastrozole as shown in a recent Australia study [5].
Pain or Pain-Inflammation
The cancer groups in our study had a higher risk of being dispensed a medicine for pain or pain-inflammation compared with the non-cancer groups. Musculoskeletal symptoms, such as arthralgia, are common side effects affecting 33% to 74% of AI users [33] and are more common than with tamoxifen. We found no significant difference in analgesics use between the tamoxifen and AI subgroups. However, the PBS dataset excludes painkillers purchased over the counter, which may cause an underestimation of the pain medicine use in our study. Furthermore, women with musculoskeletal symptoms may be more likely to discontinue AIs or switch to another endocrine therapy that was excluded from our study.
Limitations
Our study has some limitations. Firstly, dispensing claims data were used as the surrogate for the presence of comorbidity. Medications purchased over the counter and health conditions without the initiation of pharmacotherapy may be missed, such as diabetes and hyperlipidaemia managed with diet alone. We were not able to differentiate between the specific subtypes of conditions as one medicine may be indicated for several conditions falling under the same Rx-Risk-V category, such as the use of antiplatelet and anticoagulant for both cardiovascular and cerebrovascular diseases. As dispensing claims data were also used to ascertain the occurrence of the study outcomes, patients with pre-existing comorbidities had to be excluded from the related analysis. Thus, the results observed cannot be generalized to the whole relevant population that may be at higher risk than patients selected in our study. Secondly, the use of dispensing data as proxy measure would fail to identify patients with breast cancer who were not dispensed endocrine therapy (i.e. hormone-dependent breast cancer patients who do not receive endocrine therapy). However, this issue is unlikely to substantially alter the trends observed in our study, given the high sensitivity and specificity of using dispensing data alone to infer hormone receptor status, as shown in an Australian study [11]. Thirdly, the study was limited by the use of a single dataset as we were not able to obtain data on family history, date of death, other sociodemographic characteristics, and clinical factors, such as radiotherapy and chemotherapy regimen, which may be associated with the development of selected comorbidities of interest. Information on cancer stages was not available and the severity of health conditions was not taken into account using the Rx-Risk-V model as the comorbidity index. Fourthly, the study population was restricted to concessional beneficiaries that account for most medicine use in the Australian population. We did not include general beneficiaries in the analysis as the dispensing of under co-payment general prescriptions (about 18% of medicine use in Australia) were not captured before April 2012 [34,35]. Concessional beneficiaries tend to be older and at higher risk of chronic diseases than general patients. Therefore, the generalizability of our research findings to the general beneficiaries remains to be explored. Finally, we cannot rule out channelling bias [36] as tamoxifen and AIs may have been prescribed selectively according to the baseline comorbidity profile.
In conclusion, the results of this Australian population-based study demonstrated a modest increase in the incidence of specified comorbidities among women with hormone-dependent breast cancer treated with an endocrine therapy compared with women without cancer. The difference in comorbidities between tamoxifen and AIs reflected the side-effect profile of the two drugs. The development of comorbidities has become increasingly relevant with longer-term cancer survival. Understanding the incidence (i.e. a slightly higher risk of comorbidity development with HR ranges 1.15–1.36) is therefore important for the planning and implementation of better models of care to effectively address multiple chronic conditions experienced by the breast cancer population. Further research into the causes, mechanism of development, and the management of comorbidities after cancer is needed. As our study was limited by the use of a single dataset, additional data linkage would help to obtain more comprehensive comorbidity profiles in cancer survivors.
Footnotes
None declared.
Huah Shin Ng is supported by an Australian government research training programme scholarship. The funders had no role in the design or conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation or approval of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.