
Abstract
Ovarian cancer is the most lethal gynecological malignancy as it is diagnosed at a late clinical stage in more than 80% of patients. The development of diagnostic tests that can detect all types of ovarian cancers with high specificity and sensitivity, and at an early stage would improve survival rates. Serum inhibin is an ovarian hormone involved in the regulation of fertility, decreasing to undetectable levels after menopause. Certain ovarian malignancies, such as mucinous carcinomas and granulosa cell tumors, continue to produce inhibin, which is detectable in serum. A test for serum inhibin has been developed which is able to diagnose granulosa cell tumors and mucinous carcinomas with high accuracy. When the inhibin assay is used in conjunction with the CA125 test, which detects epithelial ovarian carcinomas, the two tests detect the majority of ovarian cancers with high sensitivity (95%) and specificity (95%). This article discusses the application of the inhibin test in ovarian cancer.
Keywords
Ovarian cancer is the fifth leading cause of cancer mortality of women in the USA, and is the most lethal gynecological malignancy [1]. Ovarian cancer comprises a variety of tumors arising from germ cells, stroma or surface epithelium. They can be divided into the following histological categories: epithelial cancers (e.g., serous, mucinous, endometrioid and clear cell), epithelial borderline tumors (e.g., serous, mucinous, endometrioid and clear cell), sex-cord stromal tumors (e.g., granulosa cell tumors [GCTs]) and germ cell tumors. The molecular and genetic events associated with the development of ovarian malignancy are still largely unknown, thus contributing to the lack of reliable biomarkers for detection of the disease. Diagnostic tests are available to detect most epithelial cancers, in particular serous carcinomas; however they do not detect all types of ovarian cancers, and in all instances they are limited by their sensitivity and specificity characteristics.
Serum inhibin in ovarian cancer
Our interest in the potential role of inhibin as an ovarian cancer tumor marker arose from earlier observations that serum inhibin levels are elevated in women with granulosa cell tumors [2] and mucinous ovarian cancers [3].
Inhibin plays an important role in the regulation of fertility [4]. It is produced by the ovaries and testes and secreted into the bloodstream to act as an endocrine factor. It specifically inhibits the secretion of the pituitary hormone, follicle-stimulating hormone (FSH), which has key actions in promoting ovarian folliculogenesis in the female, and spermatogenesis in the male. In turn, FSH stimulates inhibin production in the gonads thus forming a FSH–inhibin feedback mechanism for regulating fertility. An outline of its mode of action is presented in Box 1.
Inhibin is a member of the transforming growth factor-β superfamily of growth factors [5]. It is a heterodimeric hormone comprising a common α-subunit and one of two β-subunits (α-βA forming inhibin A, or α-βB forming inhibin B). In plasma, inhibin is present in precursor forms (>50 kDa), mature biologically active forms (30 kDa) and as a biologically inactive free α-subunit.
Research exploring the reproductive physiology of inhibins A and B in the ovary has shown that inhibin A is primarily produced by mature follicles and corpora lutea while inhibin B is predominantly formed by developing antral follicles. In fact, inhibin B is used as a marker of ovarian follicle reserve in assisted reproduction treatments [6]. Following menopause or oophorectomy the circulating levels of inhibin A and B, and free α-subunit fall to nondetectable concentrations. This observation has proven to be a useful low-level baseline, important in the development of a sensitive inhibin test for ovarian cancer.
Studies have examined which of the inhibin forms is the predominant ovarian cancer marker [7]. It was concluded that a measurement of all α-subunit-containing forms (i.e., inhibins A and B, and the free α-subunit) is the preferred end point in detecting all cancer types. For example, in some GCTs, dimeric inhibins, and in particular inhibin B, are the primary forms found in serum, whilst in mucinous carcinomas it is the free inhibin α-subunit that is primarily detected. It is interesting to note that the elevated dimeric inhibin levels observed in GCTs are matched by a corresponding decrease in FSH but not luteinizing hormone (LH), consistent with the presumed biological role of inhibin to differentially suppress FSH. Mucinous carcinomas show minimal FSH changes following surgery, consistent with the production of biologically inactive inhibin α-subunit by this malignancy.
Inhibin's mode of actioin
The mode of action of inhibin is complex and still far from resolved. Inhibin is a very effective antagonist of activin and bone morphogenetic proteins (BMPs) (co-members of the transforming growth factor [TGF]-β family of growth factors [28,29]), in conjunction with an accessory binding protein called β-glycan and thus inhibin's role is viewed as that of an antagonist of these proteins rather than as an independent activator. The role of inhibin in regulating follicle-stimulating hormone (FSH) can be explained by its ability to antagonize activin's stimulation of FSH production.
However, inhibin may act through other mechanisms as it has been shown that:
In mice in which the inhibin α subunit gene has been deleted [30], ovarian and testicular cancers are generated with almost 100% penetrance. This cannot be simply explained by a concomitant increase in activin levels as activin has not been shown to be tumorigenic.
In mice with inactivating mutations to an oocyte growth factor, GDF9 [31], ovarian follicles are unable to progress beyond the primary stage. However, in mice in which both the inhibin α subunit and GDF9 genes are inactivated, ovarian folliculogenesis proceeded well beyond the antral follicle stage. These data suggest that ovarian folliculogenesis is normally heavily suppressed by inhibin and that folliculogenesis proceeds when this suppression is released in an appropriate setting. The basis for this suppression by inhibin is unclear. One possibility is that inhibin may be inhibiting the action of activin and or other TGFβ members such as BMP which are critical for folliculogenesis. Another possibility is that the inhibin α subunit may exhibit a specific but unknown tumor/growth suppressive action, perhaps at the level of its interaction with a specific receptor; however, as yet no such receptor has been identified.
Based on these observations, we have developed a total inhibin enzyme-linked immunosorbent assay (ELISA) that detects all α-subunit-containing forms of inhibin [8–11]. This test consists of paired monoclonal antibodies directed against two non-overlapping epitopes on the carboxy-terminal region of the inhibin α-subunit (αC region). The test has been applied to serum of healthy postmenopausal women and posmenopausal women with ovarian cancer [9] or benign ovarian tumors [11]. The vast majority of inhibin values for healthy women were at, or below, the sensitivity of the inhibin ELISA, with clear elevations in women with mucinous ovarian carcinomas and GCTs. In contrast, serum inhibin levels in other ovarian carcinomas were low or nondetectable (Figure 1).

Serum inhibin as determined by total inhibin ELISA and serum CA125 in normal postmenopausal women and postmenopausal women with ovarian and non-ovarian cancers.
A number of studies have been undertaken to address the following questions regarding the strengths and weaknesses of the total inhibin test in application to ovarian cancer, which shall be discussed below.
Does the total inhibin test detect benign ovarian disease?
A range of benign ovarian tumors were examined (Figure 2 [10]). With the exception of thecomas where high inhibin levels were observed, other benign forms had on average low or nondetectable levels.
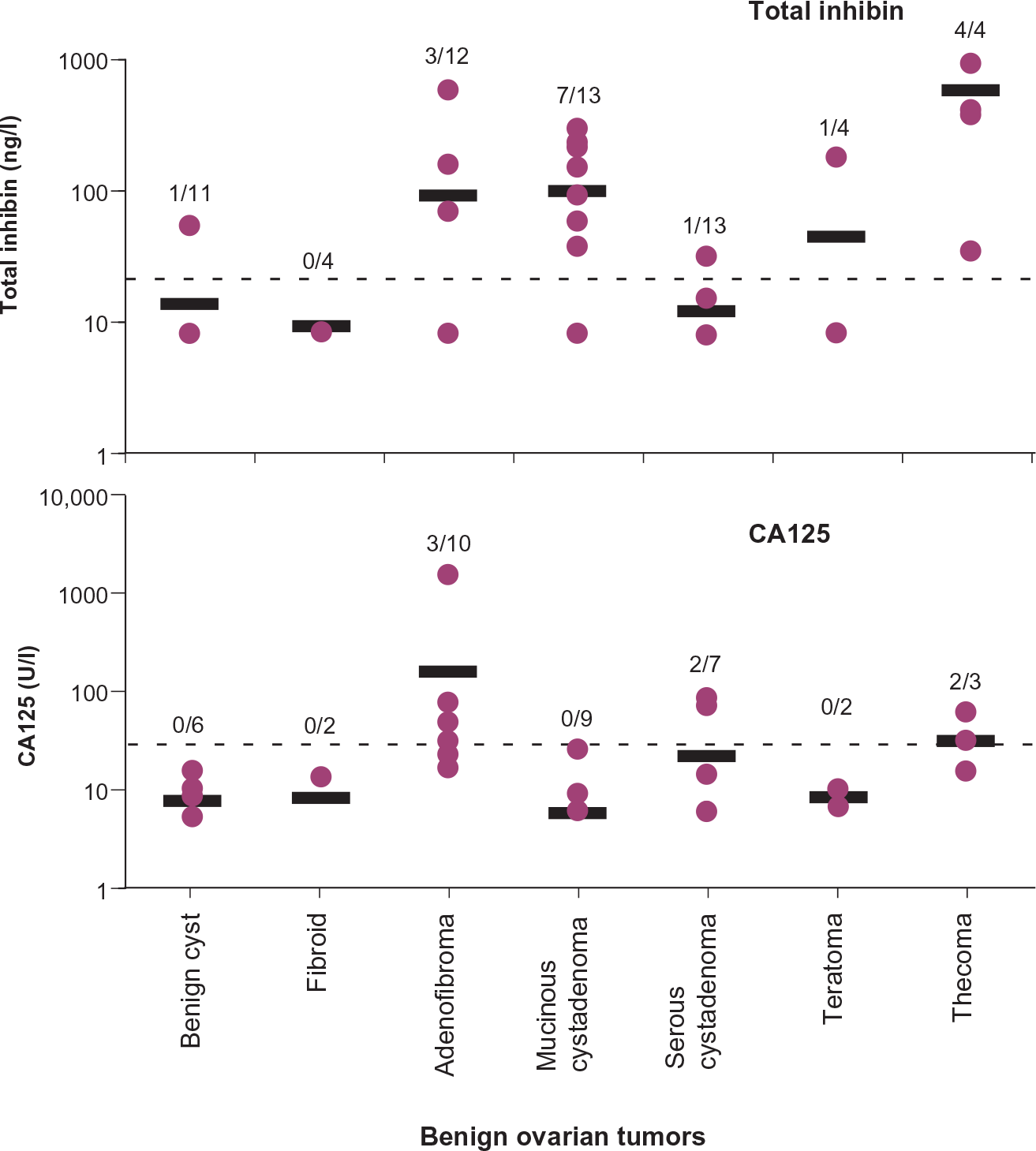
Serum inhibin as determined by total inhibin ELISA and serum CA125 in normal postmenopausal women and postmenopausal women with benign ovarian tumors.
Does the total inhibin test detect other cancers?
Serum inhibin levels were very low or nondetectable in postmenopausal women with either breast or bowel cancer [9] (Figure 1).
Is the total inhibin test applicable to women during their reproductive life?
The test was initially applied to postmenopausal women, comparing serum inhibin levels from these women with cancer to the nondetectable baseline concentration seen in healthy women of this group. During reproductive life, total inhibin concentrations demonstrate a pattern over the menstrual cycle with low values during the first 5 days following the initiation of menstruation, increasing to separate peaks in the late-follicular and mid-luteal phases [11]. By allocating the first 5 days of the cycle as a stable low baseline, the inhibin values for this period can be compared with GCT values. On this basis, 13 of 16 GCT values were significantly elevated compared with 16 of 16 values after menopause, indicating that the inhibin test has utility, at least for GCTs, during this period. However, mucinous carcinomas cannot be distinguished due to the lower inhibin levels produced by these malignancies.
Does the total inhibin test detect early stage invasive & borderline disease?
The serum inhibin data available at this stage applies only to mucinous ovarian tumors. In Stage I carcinomas (disease confined to the ovary) 9 of 15 (60%) of the malignancies were detectable compared with 7 of 8 (88%) in advanced Stage III disease. Mucinous borderline tumors showed elevated inhibin levels in 13 of 20 (65%) of the cases. Since granulosa cells express high levels of inhibin it would be anticipated that inhibin is a suitable marker for early GCTs. Clinical studies to establish the role of inhibin in early detection of GCTs have yet to be performed.
How effective is the total inhibin test for monitoring recurrence of the disease following treatment?
Recurrence of ovarian cancer following treatment is a likely prospect, particularly in late-stage disease. Retrospective studies with GCTs have shown that serum inhibin rises with recurrent disease. In some cases, increasing serum inhibin was observed up to 2 years before the recurrence was detectable. Therefore, serum inhibin appears to play an important role in the follow-up of patients with GCTs [12]. It is unknown to date if inhibin is similarly effective with mucinous carcinomas.
Combined serum inhibin & CA125 as a diagnostic test in ovarian cancer
CA125 (MUC 16) has been used as a serum tumor marker for 20 years [13]. It is a surface glycoprotein found on the epithelium of cancerous ovaries but absent in healthy ovarian tissue. The CA125 test is a valuable tool for identifying epithelial cancers (particularly the serous and endometrioid subtypes) but is less effective in non-epithelial tumors. Furthermore, CA125 is less effective in the detection of early disease when compared with advanced stages (Table 1). Serum levels of CA125 are also elevated in other diseases of the peritoneal cavity, such as endometriosis, thus limiting its specificity.
List of recently published serum markers assessed for detecting ovarian cancer.
Sensitivity is defined as the proportion of cancer patients correctly identified: (true positives). Specificity is defined as the proportion of control patients correctly identified: (true negatives).
Serous sera versus controls.
apolipoprotein A1, transthyretin, a- trypsin inhibitor fragment.
The observation that CA125 is readily produced by ovarian epithelial malignancies suggests that the combination of the inhibin and CA125 tests in serum would be complementary, leading to an overall higher proportion of ovarian cancers detected by the combined test. Using several statistical approaches we were able to show (Table 2) that the percentage of cancers detected with the combined inhibin–CA125 approach was significantly higher (95%) than with the CA125 (82%) alone [9].
Percentage of cancers detected at 95% specificity for total inhibin and CA125 assays and combination of assays.
p < 0.05 versus inhibin or CA125
Incidence of the various cancers is also presented. See [9] for further details.
A comparison of the total inhibin test with other ovarian cancer tests, as outlined in Table 1, shows that the combination of the total inhibin and CA125 tests provides the highest specificity: sensitivity values (95%:95%) although other markers approach these values (e.g., prostasin + CA125). The advantage of the inhibin test is that it compliments the CA125 test by providing a specific marker for granulosa cells tumors and improves the detection of mucinous cancers. These advantages apply primarily in the treatment of women after menopause.
Inhibin α-subunit as an immunocytochemical marker of GCTs
Antisera to the inhibin α-subunit has been widely used as an immunocytochemical test for identifying sex-cord stromal tumors [14–17], in particular GCTs, supporting the elevated plasma levels found in women with GCTs [11]. Studies using either polyclonal or monoclonal antibodies to the NH2-terminal region of the αC region of the inhibin α-subunit have shown over 95% positive response with these tumors [14–17]. Inhibin, in conjunction with nonspecific markers, has been used to differentiate between different stromal tumors (e.g., germ cell tumors) and poorly differentiated carcinomas.
The use of inhibin α-subunit antisera to detect mucinous tumors is controversial. Based on immunocytochemical analysis and inhibin α-subunit expression of microdissected epithelial and stromal tumor tissue, it was shown that the stromal cells, but not the epithelial cells, were positive for the presence of the α-subunit [16]. These results suggest that the stromal tissue, rather than the epithelium, is the source of inhibin and as an extension the source of serum inhibin in women with mucinous carcinomas. However, there is also evidence that employing the α-subunit antiserum (designated R1) on fixed tissues results in immunoreactivity detected in stromal tissue of mucinous tumors, while in frozen tissues the immunoactivity was localized to the epithelial cells [18]. These conflicting data have not yet been satisfactorily resolved.
Conclusions
Serum inhibin is a useful diagnostic test for GCTs and mucinous ovarian carcinomas with limited sensitivity for non-mucinous epithelial ovarian carcinomas in postmenopausal women.
A combination of serum inhibin and CA125 is able to diagnose the majority of ovarian carcinomas with 95% sensitivity and 95% specificity.
The inhibin test is viewed as useful for the diagnosis of GCTs, but not mucinous epithelial ovarian carcinomas, in premenopausal women.
The inhibin test is suitable for following up patients with treated GCTs.
Future perspective
Ovarian cancer presents at a late clinical stage in more than 80% of patients, with only a 35% 5-year survival rate. In contrast, the 5-year survival for patients with organ-confined Stage I ovarian cancer exceeds 90%, and most patients are cured of their disease. Detection of the early stages is therefore the best way to improve survival rates [19,20], warranting the development of a highly sensitive and specific diagnostic test or biomarker for early detection of ovarian cancer.
However, there are difficulties in the development of a suitable screening test. First, ovarian cancer has a very low incidence (1:47 lifetime risk or 1:2000 across a population of postmenopausal women [101]) and therefore a high accuracy in terms of specificity and sensitivity is required for an effective screening test. A blood test, for example, with a false-positive value of 5% (sensitivity of 95%) would result in 100 false-positive cases for every ovarian cancer case detected. A test with a sensitivity of at least 99.5% is therefore warranted. A number of blood cancer tests have been developed or proposed, as outlined in Table 2. Despite the relatively large number of tests available to date, CA125 is the only established marker in clinical use, mainly due to a high false-positive rate of all other tests. It is conjectured that a combination of tests may result in higher sensitivity values (Table 2), although these studies are still limited. Overall however, the positive predictive values of these tests for ovarian cancers are low (< 1%).
Second, identifying new cancer-specific markers in blood, most likely at very low concentrations, is a daunting task, stretching the currently available technologies. Plasma protein concentrations of known cancer markers (e.g., inhibin, CA125 or prostate-specific antigen) are in pg–ng/ml concentrations while the total protein concentration of plasma is about 70 mg/ml, a considerable swamping by non-cancer proteins. One would anticipate that other (new) cancer-specific markers in blood would be at similar low concentrations. Their identification would require the ability to differentiate between serum proteins from cancer and control groups in order to identify the cancer-specific protein. There are however, major technical difficulties involved in the separation and identification of trace proteins in blood. The technology is only now evolving using new proteomic methodologies linked to mass spectrometry. Some progress has been made but these approaches are still in the development stage [21].
Executive summary
Of women diagnosed with ovarian cancer, 60% die of the disease, hence there exists a need for new diagnostic tests with sufficient sensitivity and specificity to detect this malignancy.
Inhibin is produced by ovarian follicles, with a key role in regulating fertility. Serum inhibin levels are undetectable in postmenopausal women when ovarian follicular activity ceases.
Inhibin is elevated in the serum of postmenopausal patients with granulosa cell tumors (GCTs) and mucinous carcinomas of the ovary. Inhibin levels in other epithelial ovarian carcinomas (serous, endometrioid) are low or nondetectable.
Serum inhibin in conjunction with serum CA125, detects the majority of ovarian carcinomas in postmenopausal women at 95% sensitivity and 95% specificity. It is therefore a good diagnostic test for ovarian cancer.
Serum inhibin is viewed as a useful test for detecting GCTs during reproductive life, although less sensitive in the detection of ovarian mucinous carcinomas due to elevated inhibin during the menstrual cycle.
Serum inhibin is low or nondetectible in women with benign ovarian tumors (except for thecomas) and low in malignancies like breast or bowel cancer.
The role of inhibin as an early cancer marker (i.e. as a screening test) has yet to be determined, although it is viewed as a likely candidate in GCTs.