
Abstract
Antimicrobial treatments are being incorporated into various military items, including T-shirts, socks, and sleeping bag liners, to address a variety of soldier hygiene issues such as odor, athlete's foot, and skin irritation. For any medical or hygiene issue, it is not known what performance constitutes an effective treatment, or if existing treatments are providing a benefit and positive return on investment. The effect of prolonged wear of treated textiles on the skin has not been examined. While treatments provide perceived benefits, existing methods to assess efficacy in military-relevant environments are lacking. Current Army efforts are underway to define the magnitude of soldier hygiene issues, determine performance for an effective treatment, and investigate test methods to acquire meaningful data.
Introduction
There is a long history of skin-related medical problems within the military population, dating back to World War I and evolving through Operations Iraqi and Enduring Freedom (OIF and OEF). According to a recent review, about 27% of dermatologi-cal diagnoses recorded in theater correlated with a bacterial or fungal infection. 1 Most infections were exacerbated in hot and humid climates, such as in Vietnam, while other conditions, for example, eczema, were more prevalent in dry climates, such as in Iraq and Bosnia. There is a high morbidity of dermatological problems in theater, as illustrated by the 883 evacuations of military personnel over a three-year time period during OIF/OEF, accounting for a significant decrease in operational readiness. 1 Better prophylaxis for skin conditions needs to be explored and implemented for warfighters who serve in a variety of regions around the world.
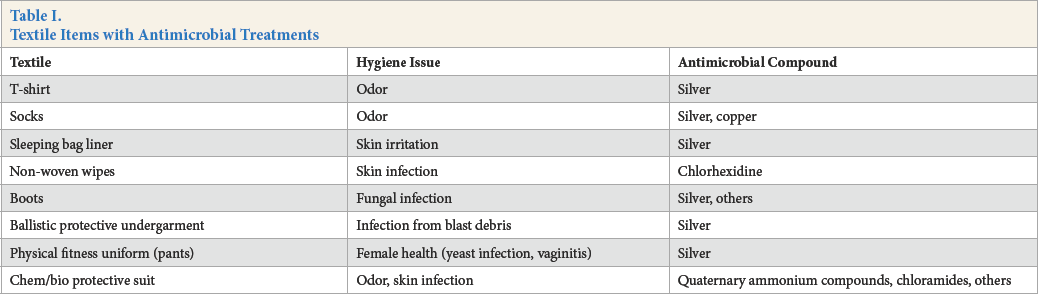
Recent widespread use of anti-odor, antifungal, and antibacterial technologies within the civilian population has led to the incorporation of such products into materiel for distribution to military personnel. Currently, there is no official specific requirement for an antimicrobial textile (AMT) in clothing or equipment. However, within the last decade, a number of textile items were fielded that incorporated antimicrobial functionality (Table I). These items have performance specifications associated with them; for example, “textile XYZ will have a treatment that exhibits 99% reduction of Staphylo-coccus aureus.” In many cases, it is unclear how performance specs were determined. In some instances, the antimicrobial functionality was removed from an item. Reasons for this include questions as to whether the treatment was providing any benefit and difficulties in determining if performance specifications were being met (variability observed when conducting standard test methods).
Textile Items with Antimicrobial Treatments
Field Studies
After the initial request that antimicrobial functionality be included in textile items, several field trials were conducted starting in 2005. Items fielded to soldiers included the Army Combat Uniform (ACU), tan T-shirts, and green boot socks. To ensure safety and avoid potential toxicity issues, each antimicrobial component passed a health hazard analysis (HHA) completed by outside labs and the Army's Public Health Command (PHC).2,3 Natick Soldier Research Development and Engineering Center (NSRDEC) subsequently completed human user evaluation studies, as well as lab analyses for efficacy of antimicrobial capabilities. Overall, those tests were inconclusive and subsequently no further evaluation was conducted.
Considerations for AMT Design
Knowledge of the skin microbiome and its physiology is important in relation to AMTs, because ideally an antimicrobial formulation would possess the ability to kill or inhibit growth of pathogenic or undesirable organisms while maintaining the integrity of the normal skin flora. The impact of the body's physiology and environmental parameters on skin barrier homeostasis should also be considered. The effects of long-term AMT wear on the normal skin microbiome and potential microbial resistance has not been well studied. In addition, the type and performance of a treatment will be determined by the intended application, with performance ranging from bacteriostatic to bactericidal (Fig. 1).

Antimicrobial performance is application dependent.
Requirements
Currently, no requirement exists for antimicrobial textiles. The US Army Training and Doctrine Command (TRADOC) and Maneuver Center of Excellence (MCoE) are responsible for requirements determination by analyzing gaps in current capabilities, projecting future threats and operational environments, and codifying requirements as mission needs that will allow industry to propose appropriate materiel solutions. Determination of soldier hygiene issues will be used by TRADOC and MCoE as part of the pool of information referenced to determine if an antimicrobial requirement is necessary. Incident rates, costs, and effects on operational impact are all factors to be considered.
This study was conducted at the request of TRADOC and MCoE to review the information necessary for generating specific requirements and standards when incorporating antibacterial, antifungal or anti-odor properties into military textiles. Secondly, it depicts the particular health and medical issues that potentially necessitate use of AMTs. Medical cost analyses will also be described to illustrate the monetary impact of bacterial and fungal complications. The issues are then grouped and ranked according to surveillance and cost analysis data to determine the nature of importance. Recommendations for future testing and evaluation are also discussed.
Methods
Identification of reportable soldier hygiene issues, including incidence rates and demographic information were determined from the following sources: literature, the Defense Medical Epidemiological Database (Armed Forces Health Surveillance Center) and the Total Army Health and Injury Outcome Database (US Army Research Institute for Environmental Medicine). Cost analysis of identified issues was conducted using the Medical Cost Avoidance Model (US Army Public Health Command). Hygiene issues were then ranked by incident rate and cost to determine the highest priority to recommend for further investigation. Non-reportable, quality of life issues were determined via online survey in conjunction with the Consumer Research Team at NSRDEC.
In addition to defining the extent and prioritization of soldier hygiene issues, gaps in the use of AMT solutions were also identified, as well as recommendations for future research and testing efforts.
Results and Discussion
Reportable Hygiene Issues
Medical surveillance data can be used for epidemiological analyses of relevant medical and health conditions associated with bacteria and fungi. Information from the Defense Medical Epidemiological Database (DMED), which is the largest repository for military medical data, as well as information from Total Army Injury and Health Outcome Database (TAIHOD), will be used in this report.
A large part of the current risk versus benefit analysis of AMTs are assessing the monetary consequences for treat-ment of the medical conditions associated with bacterial and fungal infections. Briefly, the Medical Cost Avoidance Model (MCAM) uses ICD-9 code billing information and estimates costs such as lost time, clinical visits, and hospitalization for the specific diagnosis. A full explanation of the model can be found in a paper by Smith et al. 4
Bacterial Skin and Soft Tissue Infections
Background and Military Relevance
Skin complications ranging from irritation to secondary infections can account for significant lost time and negative operational impact. 1 Skin and soft tissue infections (SSTI) are an important public health issue during military training and deployment, and can be exacerbated by close living quarters and communal contact.5–7 Many warfighters don't find it necessary to report all skin irritations to medics or physicians; however, problems can arise when proper prevention and treatment techniques are not used. Any breaks in the skin, such as open blisters, lesions, scratches or burns, can instigate development of infection, or even have systemic effects causing fever (Fig. 2). 8
Summary of bacterial skin infections.
Infection Rates
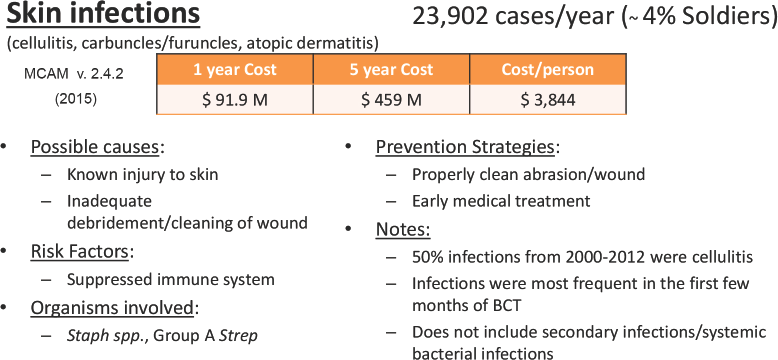
In 2013, the Medical Surveillance Monthly Report (MSMR) summarized SSTI rates among active US troops from 2000 to 2012 to specifically include the following diagnoses: cellulitis, carbuncle/furuncle, erysipelas, and other conditions. 8 Most notably, the study found that half of the infections were diagnosed as cellulitis and, of these cases, 40% were in the lower extremity. It was also found that most SSTI cases occurred frequently during first few months of basic combat training.
MSMR creates a good picture of infection rates within troops in training and garrison using data retrieved by the Military Health System, however, there is less data concerning troops in theater. May et al. (2011) did discuss incidence of SSTI in deployed US troops, but used self-reported scales. 7 Questionnaires were voluntarily completed by approximately two-thousand soldiers who came through a medical clinic in Qatar over the course of approximately one year; about 5% reported one or more SSTI during their most recent deployment. This rate was higher than expected based on previously published incidence rates among active duty service members. This is evidence that many warfighters do not report these conditions, most likely because the irritation or infections are uncomplicated and medical treatment is not necessary. Of the soldiers who reported SSTI, 95% of conditions were uncomplicated, meaning they did not need extensive treatment from a medical provider; however, about 20% reported missing at least one day of work due to their condition, which could significantly impact any military mission. 7
Cost Analysis
We can assess approximate medical costs for different diagnoses associated with skin-related infections presented in active duty soldiers at Military Treatment Facilities (MTF) by using MCAM (version 2.4.2) and associated ICD-9 codes. This dataset does not include medical facilities in operational environments (Iraq, Afghanistan, and so forth). According to the model, the average number of cases per year (between Fiscal Year 2010-2012) of SSTI was 23,902, for an approximate yearly medical cost of US$91.9 million or US$459.4 million over 5 years (inflation is accounted for in the MCAM model). Analysis of SSTI used ICD-9 codes for carbuncles/furuncles, cellulitis, and atopic dermatitis.
If the assumptions are made that AMT uniform components were to be fielded and used, and that they are effective against some or all of these medical conditions, we can estimate medical cost avoidance over specific time periods. Table II displays an example of the monetary savings if diagnoses are decreased by 10%, 25%, and 50%, over time spans of 1 year and 5 years. Not only do SSTI affect a significant number of soldiers, but there is an expensive medical cost per case at almost US$4,000 which includes associated costs for lost time, clinic and hospital visit hours, and potential disability compensation. 4
Medical Cost Avoidance for SSTI Based on Data from the MCAM v. 2.4.2
Summary
There is a large amount of research regarding the use of antimicrobials in textiles to reduce overall bacterial colonization on the skin surface. However, less is known about how AMTs could prevent or treat SSTI, and even the probability of secondary infections after trauma during military exercises. Clinical data shows the possibility of a particular AMT using silver technology helping with treatment of certain skin conditions such as atopic dermatitis;9–12 however, there is limited research regarding prevention of SSTI, or treatment within a military population. Longitudinal surveillance studies would be needed to determine if AMTs would reduce incidence rates of SSTI or secondary infections. A cost-benefit analysis utilizing the MCAM and pricing of purchasing/ distributing pieces of the uniform/equipment with antimicrobials should be done.
Fungal Skin Conditions
Background and Military Relevance
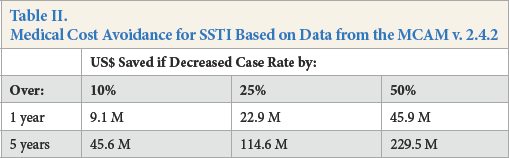
There is a long history of fungal skin conditions, such as athlete's foot and jock itch among the military and a moderate amount of data regarding fungal growth and infections, especially in the feet. 5 Tree known species of fungi are specifically responsible for the majority of infections: Trichophyton rubrum, Trichophyton mentagrophytes and Epidermophyton floccosum.5,13
Warfighters are exposed to increased risk factors during field training exercises or deployment including hot and humid ambient weather, poor skin hygiene, and close-quarter living, 14 potentially causing increased rates of infection. Despite the many fungal conditions and infections, most are likely unreported to medical personnel and are therefore undocumented and sometimes untreated (Fig. 3).
Summary of fungal skin conditions.
Infection Rates
A 2001 study in MSMR looked at a two-year surveillance period of cutaneous fungal infections throughout the US Army and found that of over 66,000 visits to MTF for fungal-related issues, 19.1% were foot infections. 12 Locations of infection on the body are important for researching ways to minimize fungal growth by the addition of antimicrobial/antifungal formulations into textiles. In addition to the feet, where we find the highest rate of fungal accumulation and infection, it may be beneficial to focus on the groin as well to assess benefits from AMTs.
It is also important to note that three of the four US geo-graphical locations for highest incidence rate of fungal infections included Basic Combat Training facilities (Forts Knox, GA; Leonard Wood, MO; and Benning, GA). 14 Assessing geographic location of incidence is important in determining which soldiers are at higher risk, for instance, if rates are different between soldiers at initial entry training locations (e.g., Fort Benning) versus other installations (e.g., Joint Base Lewis-McChord, WA). Environmental conditions, such as ambient temperature, humidity, wind speed, and sunlight, should also be taken into account when analyzing the prevalence of fungal foot infections, along with other odor or hygiene issues. Potential correlation with incidence and ambient environments of higher average temperatures and humidity may be observed.
Research
Athlete's foot (Tinea pedis) is a common problem not only among the military, but also the civilian population; at any given time, up to 25% of the population may be affected. 15 Data was collected among military personnel from numerous countries outside of the United States to assess the incidence and risk factors associated with fungal foot infections. It was found that the military lifestyle imposes additional susceptibilities for infections such as high intensity training, excessive sweating, prolonged shoe/boot wearing, and decreased frequency of sock changes.13,15–18Another factor to consider is the repetitive pressure and constant friction the feet endure on a daily basis, causing blisters and open wounds that can increase the risk for infection. 16
Cost Analysis
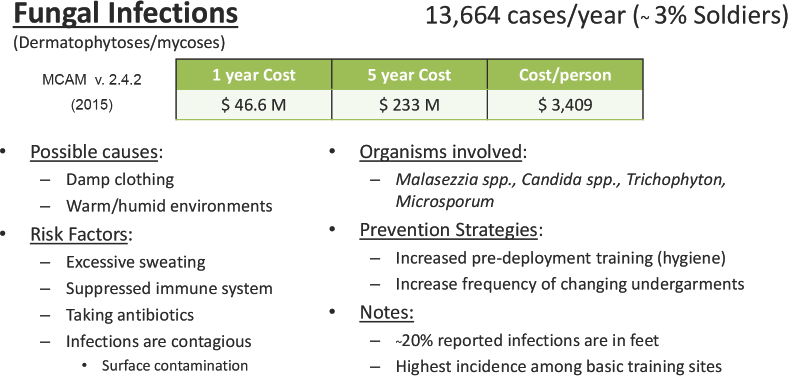
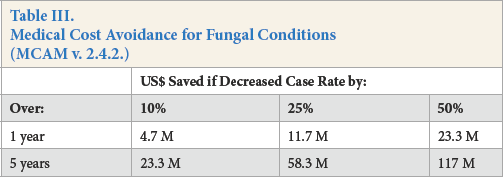
Medical costs associated with reported fungal associated conditions at MTF were assessed with the MCAM and associated ICD-9 codes. Between Fiscal Year 2010-2012, there were approximately 13,664 yearly diagnoses, costing about US$47 million per year. Table III displays the monetary savings if diagnoses are decreased by 10%, 25%, and 50% over time spans of 1 and 5 years.
Medical Cost Avoidance for Fungal Conditions (MCAM v. 2.4.2.)
Summary
Medical issues pertaining to fungal outgrowth are important to consider along with bacteria-related conditions. While infections of the feet only explain 26% of total fungal infections among American warfighters, foot infections account for almost 50% of the medical costs. Potential interventions worth exploring for infection prevention could include an AMT sock or sock liner, and/ or better training and education of foot and skin health while in the field or on deployment, especially in warm and temperate environments. Because it is assumed that a majority of fungal problems go unreported and untreated, antimicrobial products effective against fungi could be beneficial for the warfighter.
Female Health Issues
Background
Females comprise about 15% of the Armed Forces and their anatomy creates particular hygiene and health issues, which either do not happen as frequently or cannot occur in males. There is a significant prevalence among females of urinary tract infections (UTI) and other genitourinary and gynecological related-issues in garrison as well as in theater. UTI results from bacteria, namely Escherichia coli, ascending up into the urethra, and if left untreated, into the ureters and eventually the bladder, causing cystitis. 19 Vaginitis is typically caused by an imbalance of vaginal pH and normal bacterial flora. 20 Yeast infections, or Candidia-sis, are normally caused by Candida albicans, but can be from other yeast as well. All of these conditions affect up to 75% of women at least once during their lifetime and while all have similar predisposing factors, each are treated in a different manner (Fig. 4).
Summary of female health issues.
Infection rates
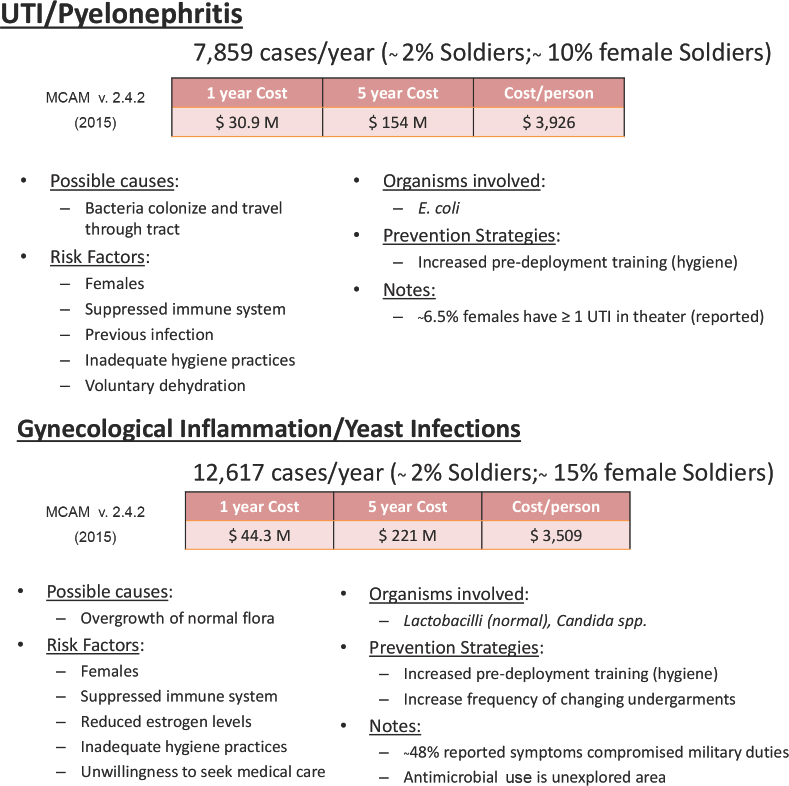
Two recent studies published in MSMR specifically analyzed UTI among all branches of active US Armed Forces between 2000 and 2013, as well as in deployed personnel between 2008 and 2013.21,22 For all active duty service members, it was found that 30.4% of females had at least one medical UTI encounter and 12.5% had recurrent UTI. 21 It should be noted that one soldier may have been diagnosed more than one time in a given year. During a six-year surveillance of about 111,000 deployed females, it was found that 6.5% had at least one UTI, 22 2.6% were diagnosed with a yeast infection, 23 and about 9.7% with a gynecologic disorder (vaginitis). 24 A separate study randomly surveyed 841 female service members who had deployed and found higher incidence rates of UTI (18%), vaginitis (30.1%), and yeast infections (10.4%). 25 It is important to note that 48% of service members who reported symptoms of vaginitis and cystitis were put on limited military duties during deployment and 27.4% of these females lost duty time.24,26
Cost Analysis
Costs associated with genitourinary and gynecological medical conditions were assessed with the MCAM and associated ICD-9 codes. Total medical costs per year related to UTI, yeast infections, and vaginitis were about US$81 million. About US$31 million of which was for UTI alone, coming out to almost US$4,000 per case, mainly due to the fact that hospitalization costs are very expensive. Table IV displays the monetary savings if diagnoses are decreased by 10%, 25%, and 50%, over time spans of 1 and 5 years.
Medical Cost Avoidance for Female Health Conditions (MCAM v. 2.4.2.)

Summary
UTI and other gynecological issues are prevalent among female service members at a similar frequency to the civilian population. The high incident rate is a problem leading to lost work time, possible duty limitations, and even hospitalization. A few methods of intervention are being assessed, but several studies discuss the need for additional or improved pre-deployment training in regards to female personal hygiene and health assessment.26–28 Whether it is increased training for better hygiene, or incorporating an antimicrobial into undergarments of uniforms, decreasing rates of the particular female medical issues mentioned above by just 10% would save the military roughly US$36 million in medical costs over 5 years.
Ranking/Stratification of Issues
To determine the significance rank of the aforementioned medical conditions, several different factors were taken into consideration. We used surveillance data, as well as medical cost analysis data, for each condition and stratified the data into the three groups: bacterial SSTI, female health issues, and fungal infections (Table V).
Ranking of Reportable Hygiene Issues

Rankings were based on 1) average number of cases per year (from 2010 to 2012), 2) associated total medical cost, 3) cost per case, and 4) cost of lost time per case. Within each of the three main condition groups, the top three or four specific diagnoses (by ICD-9 code) were selected and ranked based on the same data (Appendix A). Because the number of cases does not necessarily correlate with total associated medical cost, all four categories were taken into account when ranking the conditions.
Non-Reportable/Quality of Life Hygiene Issues
Background and Military Relevance
Malodor production from the body and odor on clothing and equipment is a significant quality of life concern among the warfighter population. Considering training and field environments, several external factors contribute to this hygiene issue. Among them are constrictive clothing and/or layering techniques that protect warfighters from elements of the environment. The clothing or uniforms can inhibit normal physiological mechanisms that cool the body when overheated such as normal sweat evaporation from the skin. In addition, warmer environments, heavy load carriage, and training exercises at high intensity and for longer durations cause increased sweat rates. The skin and innermost layer of clothing, when saturated, essentially become a substrate for increased bacterial and fungal growth, correlating with increased malodor.
Military personnel are at high-risk for poor hygienic behaviors, especially when they live and work closely together for extended periods of time. 29 Poor hygiene combined with additional environmental factors (e.g. temperature/humidity) lead to increased bacterial and fungal growth, odor, and even subsequent infection. Additionally, training in the field or conducting lengthy missions result in lack of access to laundry facilities, resulting in bacteria and fungi growth and increased odor production on the textile. Even when using detergents, washing clothing at temperatures lower than 40 °C (104 °F) does not effectively kill skin microflora, and malodor accumulates further when clothes are re-worn. 30
The perception is that problems of odor, foot odor, and general hygiene throughout the military presumably arise during long training exercises in the field or during deployment. Odor issues may seem to rate as a low priority since it is typically temporary and not of medical importance, however, there are extreme circumstances, such as in special operations missions, where simple significant body odor could give away fighting positions or affect relationships with local nationals.
Research
There have been a number of field evaluations of AMTs to determine if the antimicrobial treatments would manifest itself in ways perceivable to the warfighter. Subjective and self-reported data were collected before, during, and after soldiers wore treated ACU, T-shirts, and socks during a field training exercise at Fort Bliss, TX. Questionnaires were developed with the assistance of dermatologists to assess skin problems and conditions that soldiers typically face in the field. Laboratory testing was also done on items worn during field trials to determine effectiveness against specific organisms. 31 Overall results of these studies were inconclusive; however, there was a perceived benefit with the treated items by some, but not a majority, of the soldiers. The self-reported surveys indicated that there may have been some diminished incidence of skin medical conditions, but more importantly, that there was an interest in having AMTs as part of the uniforms. 31 Inconclusive data is caused in part by interpersonal variability; to overcome this, a large amount of data is required. However, numerous limitations of current test methods prevented sufficient data from being collected.
A new Army survey was recently developed by the NSRDEC Consumer Research Team to address the limitations of previous surveys in exploring the incidence of odor and certain skin conditions/irritations, and current use and expectations of using antimicrobial products, as well as any operational impact. Results described perceived problems regarding odor and personal hygiene. Occurrence of hygiene issues and impact on quality of life and job performance was also assessed (Fig. 5, A and B respectively). Almost half of the soldiers use an antimicrobial product to help control foot and/or body odor. Foot odor itself was a prevalent condition among the soldiers, with 63% reporting having the issue within the past year. Soldiers also reported that while in the field, most found it difficult to avoid body odor, but using over the counter remedies or changing clothes more frequently helped minimize the issue.
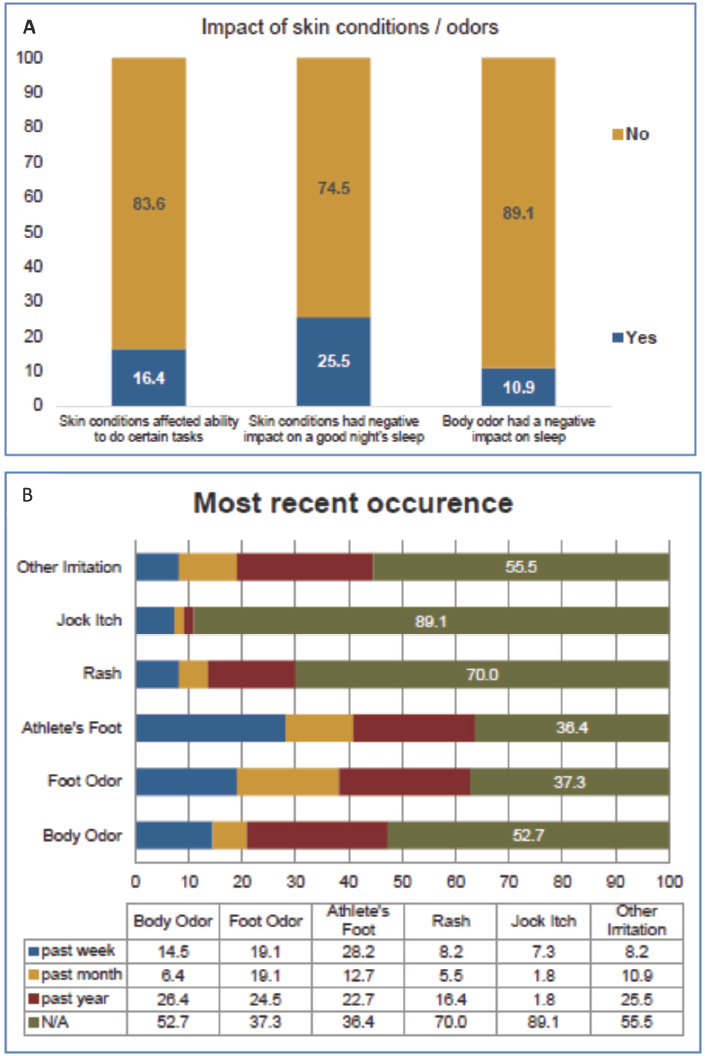
Online survey results. (A) Impact on quality of life and job performance and (B) occurrence of hygiene issues.
The limited data regarding odor among military personnel is qualitative; however, there are several methods for odor research to be accomplished in the lab. Studies have looked at both in vivo (in or on the body) and in vitro (outside the body) methods for determining odor production. While these methods work well in a laboratory setting, they may not directly translate to realistic situations. In-vivo analyses include sampling of sweat and skin swabs, and use of a panel of trained individuals who assess odor level by sniffing either samples or the test subject themselves. 32 This method of evaluation is simpler to conduct, but difficult to validate due to inter-rater variability. Rennie et al. found a significant association between the number and density of bacteria cells and underarm odor presence. 32 Therefore, in-vitro assessment of sweat, skin-swabs, or sweaty garments, using quantification of bacterial population, may be valid once a standard method is established.
Summary
Most of these soldiers reported that they use antimicrobial products for cleanliness and health benefits, in the field or during deployments, as well as to sanitize objects and other surfaces. Many use them to control personal odors (e.g., body and foot). The majority experienced athlete's foot within the past year, and many had foot odor. Some reported that their conditions had impacted their ability to complete their duties. Most have some difficulty avoiding developing body odor while in the field. Most responded to conditions (odor, itch, and irritations) by changing their clothing more often.
Recommendations for Future Evaluation and Testing
Reportable vs. Non-Reportable Hygiene Issues
Soldier hygiene issues can be stratified into two categories: reportable and non-reportable. Reportable issues can be tracked by medical diagnosis to yield incidence rates and cost avoidance calculations, as well as demographic data including geographic location, gender, and military occupational specialty (MOS). Non-reportable issues, such as odor and skin irritation, are described anecdotally and difficult to quantitate. It is also challenging to assess these “quality of life” issues and the use of AMTs as possible solutions. The survey-based data collected during field trials indicated that soldiers reported some benefit for the items with AMTs, although this was purely subjective. 31
In collaboration with the NSRDEC Consumer Research Team, an online military and civilian-wide survey was con-ducted to gain information on quality of life issues. The goals were to 1) define the magnitude of the problem, 2) ascertain attitudes toward antimicrobials, and 3) determine impacts on quality of life and job performance. The data gives a baseline of soldier perceptions related to antimicrobial use and the impact of odor and hygiene as guidance to using AMTs as potential solutions to these issues. Future field studies correlating detailed survey results with laboratory analysis would provide additional data on quality of life issues.
Data was presented in this report on a variety of reportable issues, including incidence rates (DMED and TAIHOD data) and calculated medical cost savings by prevention (MCAM). Data regarding incidence rates for reportable hygiene issues need to be further investigated in detail; a breakout of the data related to demographics (e.g., age and occupation) as well as geographic location may better inform the potential need for AMTs and generation of treatment requirements. DMED and TAIHOD databases can further define rates based on demographics and may offer a more tailored solution. Additionally, operational impact and lost time are not adequately addressed by the data in this report and data from within theater is lacking. This data would be needed to fully understand the magnitude of these hygiene issues as they affect operational readiness.
Safety Testing
The effect of prolonged exposure of AMTs directly on skin bacteria is not known. Systematic longitudinal studies of the short- and long-term effects on skin microbiota would be required to fully understand the effect. This could entail collection of skin swabs from volunteers wearing an AMT, followed by identification of the bacteria present by lab analysis. NSRDEC has discussed the possibility of inclusion in future studies conducted by organizations within the Army Medical Command such as the US Army Research Institute of Environmental Medicine (USARIEM) to collect samples for analysis. This would allow NSRDEC to potentially determine skin populations and a warfighter-specific baseline microbiome and would allow evaluation of changes in skin population to prolonged exposure to AMTs. Negative effects, such as skin irritation, could also be evaluated as another factor in safety.
AMT Performance
The performance an AMT needs to effectively counter hygiene issues has not been systematically determined. In-vivo (human) testing has been used to examine the effectiveness of particular treatments, but those studies were difficult to conduct and the data to date is inconclusive. Laboratory analysis would allow studies to be conducted under controlled conditions and would overcome the variability and limitations experienced in field evaluations. Studies using artificial skin models could be useful and is a more controlled system than in-vivo testing. These models are currently used in place of animal studies to determine skin irritation caused by chemicals. However, there is little research establishing a skin microbiome in these systems. NSRDEC is currently considering these methods to determine safety and the performance needed for an effective AMT. In previous NSRDEC field evaluation studies, microbe reduction was seen on the items (fabrics) themselves using in-vitro lab testing. However, due to the difficulty of performing the study (limitations of lab test methods) and the inherent variability of the subjects, the data was inconclusive and at best demonstrated trends in performance effective-ness. Environmentally-controlled chamber tests and/or field tests can be completed using subjects who are in an established protocol where they undergo typical soldier tasks and drills while being exposed to varied environmental conditions (heat, cold, and altitude).
New test methods would allow repeat testing on AMT items already fielded or tested, or on new technologies. The intent is to analyze performance of these textiles on a human, to assess specific variables related to the health and hygiene issues previously mentioned, and specifically, to test potential resistance and changes in microbiota of the skin in particular regions of the body. The information on medical and hygiene issues would be used to determine how and where AMT use should be focused. Prioritizing medical issues based on cost analysis and incidence rates would make the most sense. In contrast, body odor has no costs associated as it is more of a quality of life issue. There should be a focus on which soldiers are having the greatest number of medical encounters, (e.g. initial entry training (IET) or deployed) and where most of these issues occur (e.g., training sites, field, and garrison) There should also be consideration for the ambient environment. Products should not only include AMTs, but should also consider moisture wicking capabilities to make the environment less conducive to microbial growth.
Conclusions
There is a large knowledge gap between what is known regarding AMTs—the direct effects on skin bacteria and fungi and the medical conditions related to such organisms. This gap is related to the fact that humans, and their variable skin microbiota, are affected differently by AMTs.
The warfighters’ exposure to specific external factors may also impact if and how an AMT's efficacy holds against pathogenic organisms. The risk factors associated with the medical conditions previously discussed cannot be completely prevented by one product; however, components made with AMTs could potentially prevent and/or treat some of these diagnosable, reportable conditions, or at least mitigate a portion of odor issues.
Hygiene and medical issues related to bacterial and fungal outgrowth fall into reportable (known incidence rates and cost savings based on modeling) and non-reportable (quality of life with no statistics) categories. The magnitude of the problem for reportable issues can be somewhat determined by creating a ranking system based on incident rates and medical cost savings (Appendix A). This ranking system is more difficult to do with non-reportable issues, therefore comparison with reportable issues is difficult. The best course of action may be to evaluate them separately.
Regardless of the hygiene issue, the performance of an effective AMT has not been systematically determined and warrants further investigation. Questions of the effects of long term wear of AMTs remain and require additional investigation. Lab analysis under controlled conditions may be preferable to field evaluation. Once a treatment performance has been identified, the effectiveness needs to be determined and the treatment costs need to be weighed against cost savings of preventing the hygiene issue. A combination of testing under lab conditions and field evaluations are likely to be needed to fully determine AMT performance.
Research and knowledge gaps include:
The magnitude and operational impact of the non-reportable conditions within the military population
Effects of various AMTs on skin flora over time: safety and potential resistance
Correlation between the use of AMTs and reduction of medical and hygiene issues related to bacteria and fungi growth during warfighter training and deployments
Footnotes
Acknowledgements
The authors wish to thank the staff at the US Army Public Health Command, Aberdeen Proving Grounds, MD, USA, the US Army Research Institute of Environmental Medicine, Natick, MA, USA, and the Consumer Research Team, NSRDEC, Natick, MA, USA.
Appendix A
Top medical conditions within each group ranked according to number of cases per year, medical costs associated per year and per case, and cost of lost duty time per case.