
Abstract
Rhabdomyosarcoma (RMS) is a common malignancy of soft tissue, subclassified as alveolar (ARMS), pleomorphic (PRMS), spindle cell/sclerosing (SRMS), and embryonal (ERMS) types. The Yes-associated protein (YAP) is a member of the Hippo pathway and a transcriptional regulator that controls cell proliferation. We have studied the immunohistochemical expression of YAP in different RMSs, arranged in tissue microarray (TMA) and whole slide formats. Pertinent clinical data including patient age, gender, tumor location, and clinical stage were collected. Out of 96 TMA cases, 30 cases (31%) were pleomorphic, 27 (28%) were embryonal, 24 (25%) alveolar, and 15 (16%) spindle cell. Positive nuclear YAP staining was seen in the PRMS (17/30, 56.7%), SRMS (7/15, 46.7%), ERMS (19/27 or 70%), and less in ARMS (37.5%). YAP nuclear staining was significantly more prevalent in ERMS than ARMS (p=0.02). Of the 41 whole slide cases, nuclear staining was detected in all ARMS but was restricted in distribution to <30% of the cells, in contrast to ERMS and SRMS, which had diffuse or >30% staining. These results highlight the role of YAP in RMS tumorigenesis, a fact that can be useful in engineering targeted therapy. Restricted nuclear YAP staining (<30% of cells) may be of value in the diagnosis of ARMS.
Introduction
Rhabdomyosarcoma (RMS) is a common soft tissue sarcoma and is the third most common solid tumor in children in general. It occurs at a rate of 4.5 cases per 1 million children. While patients with localized disease enjoy a good prognosis with chances of cure, patients with metastatic disease have dismal outcome with 5-year, event-free survival rate of less than 30%.1,2 RMS is clinically, genetically, and pathologically a heterogeneous disease with different histologic types, mainly alveolar RMS (ARMS), embryonal (ERMS), and pleomorphic types (PRMS). 3 Recognition of the spindle cell and sclerosing patterns within the embryonal RMS category has resulted in further subclassification of spindle cell sclerosing (SRMS) as a separate category. 3 Distinguishing these different histologic types is important in the management of patients as each type is associated with its distinctive genetic makeup and clinical outcome. Combination of immunohistochemical stains and molecular tests can help differentiate most cases.4,5 ARMS presents as small round cell tumor that is characterized by PAX3/7 and FOXO1 gene fusion in >80% of cases. 6 It is biologically an aggressive tumor with a low 5-year survival rate. Similarly, PRMS and SRMS exhibit aggressive biologic behavior, and patients have adverse clinical outcome. In contrast, the molecular and cellular origin of ERMS is incompletely understood.7,8 ERMS exhibits variable prognostic patterns from low- to high-risk tumors.
Recent studies have described several genetic events and increased expression of pathway molecules in RMS, including the Hippo pathway. The Hippo pathway is a tumor suppressor that controls cell proliferation, differentiation, and apoptosis in physiological and pathological conditions. Canonical Hippo transduction involves MST1/2 and LATS1/2 protein suppressor kinases, which, in conjunction with the adaptor proteins, SAV1 and MOB1, phosphorylate, and inhibit the Yes-associated protein (YAP) and the transcriptional co-activator with PDZ binding motif (TAZ). Dysfunction or suppression of the Hippo pathway leads to persistent activation of the unphosphorylated YAP, which often contributes to cancer development. Unphosphorylated YAP translocates to the nucleus where it binds the TEA domain-containing family of transcription factors (TEAD) and behaves as an oncogene activating target genes that are involved in cell proliferation, survival, and tissue growth. 9
Increased expression of YAP has been described in many human adult and pediatric cancers, and its expression was associated with high clinical stage and short overall survival in several tumors. 10 Recent studies have revealed YAP expression in RMS where it induces proliferation and oncogenesis of RMS by inhibiting the physiological function of the muscle-differentiating protein, MYOD1. In this article, we have studied the expression of YAP in different histologic subtypes of RMS through immunohistochemical experiments on TMA as well as whole slide sections.
Materials and Methods
A retrospective analysis of archived materials from patients with the diagnosis of RMS was approved by the Office of Research Integrity of Children’s Mercy Hospital under approval number 16010017.
Patients/Subjects/Samples
Two types of patients’ materials were used for the study.
TMA: RMS cases arranged in TMA format were purchased from US Biomax (Rockville, MD). The tumor cases are arranged in duplicate 1.5 mm paraffin-embedded core tissue sections. A total of 96 RMS cases are included in the array, and each case is accompanied by pertinent clinical data including patient age, sex, tumor location, and clinical stage.
Whole slide sections: Archival paraffin-embedded tissue blocks from the Pathology files of Children’s Mercy Hospital (Kansas City, MO) were sectioned for IHC. All patients up to 18 years of age at the time of the diagnostic surgery (between January 2008 and December 2016) with the histopathologic diagnosis of RMS were enrolled. Availability of adequate tissue from diagnostic specimens for IHC staining was the main inclusion criterion. Pathology records were reviewed to confirm the diagnosis including H&E slides, previous immunohistochemical stains, and cytogenetic test results. The diagnoses were established through characteristic morphology and positive staining for desmin, myogenin, and/or MYOD1 staining. ARMS cases were previously tested for FKHR (FOXO1) gene rearrangement with fluorescence in situ hybridization (FISH) analysis of interphase nuclei from paraffin-embedded tumor using the Vysis FKHR gene (13q14) DNA break-apart probes. Positive signal indicates PAX3 or PAX7 fusion transcripts, which are the hallmarks of ARMS. Pertinent clinical information from all cases including patient age, sex, and tumor location was collected.
IHC Procedures
A monoclonal antibody against YAP (Santa Cruz Biotechnology; Dallas, TX), was used in automated IHC. According to the manufacturer, this antibody was raised against a recombinant protein sequence mapping near the N-terminus of human YAP and binds both phosphorylated and non-phosphorylated proteins. The antibody specificity has been previously determined by published experiments. 11 After optimization of working conditions, immunostaining was performed with a Leica instrument (Leica; Buffalo Grove, IL) utilizing a detection system that gives a brown color staining. After heat antigen retrieval in a citrate buffer at pH 6.0 for 20 min, the deparaffinized tumor microarray and whole slides were incubated with the primary antibody at a dilution 1:100 for 15 min. This was sequentially followed by incubation with secondary antibody, a polymer conjugate, and a coloring reagent. Separate positive controls were made from breast and prostate carcinomas and medulloblastoma, all of which were previously shown to exhibit expression of the studied protein. External negative controls were stained similarly except for omission of primary antibodies. Staining of blood vessels and stromal cells served as positive internal control while absence of staining in the lymphocytes served as negative internal control.
Measurements and Analysis
YAP staining in the TMA and whole slides was recorded in the cytoplasm and the nucleus. In the TMA slide, any nuclear staining was considered positive. For whole slides, the percentage of positive cells was also determined. Low (weak staining less than the positive control) is regarded as negative. Positive staining of 80–100% tumor cells was classified as score 3, staining in 30–79% of tumor cells as score 2, and less than 30% as score 1. The immunostained slides were independently reviewed by two pathologists, and any discrepant scores were reconciled. Statistical analysis of significant differences was performed with chi-square and Mann-Whitney U tests.
Results
Microarray Study
Of the total RMS cases (n=96), 30 cases (31%) were pleomorphic, 27 (28%) were embryonal, 24 (25%) alveolar, and 15 (16%) spindle cell/sclerosing subtypes. Ages ranged from 1 to 91 years (median age 36) with 18% of patients being less than 18 years of age. The Male/Female ratio is approximately 1.8:1. Tumors were located in the extremities (n=44), head and neck (n=11), testis and paratesticular areas (n=11), abdominal cavity (n=10), chest (n=6), prostate and bladder (n=6), and other genitourinary areas (n=8). Patients were assigned stage 2 (n=15), stage 3 (n=78), and 4 (n=3); no stage 1 patients were included.
Nuclear YAP staining was variably present in all RMS subtypes and was proportionately associated with cytoplasmic staining (Fig. 1). Positive nuclear staining was seen in the PRMS (17/30, 56.7%), SRMS (7/15, 46.7%), and ERMS (19/27 or 70%) subtypes and was least common in ARMS (9/24, 37.5%; see Table 1). Significantly more ERMS cases showed positive staining compared with ARMS (p=0.02). Positive staining was present in 7/15 (46.7%) of stage 2 and 44/78 (56%) of stage 3 tumors. Only 1 patient (1/3) of stage 4 had positive staining. Of the non-alveolar subtypes, positive staining was noted more in stage 3 than stage 2 tumors but the difference was not statistically significant (30% vs. 13%; p=0.20). Staining was present in 9/11 (82%) of tumors in the head and neck, 7/11 (64%) in the testis and paratesticular areas, and 24/45 (53%) of tumors in the extremities. No YAP staining was seen in tumors from the genitourinary organs, except for the bladder where it was noted in 3/3 (100%). There was no significant difference of YAP staining in tumors from adult versus pediatric (<18-year-old) patients (Table 2).
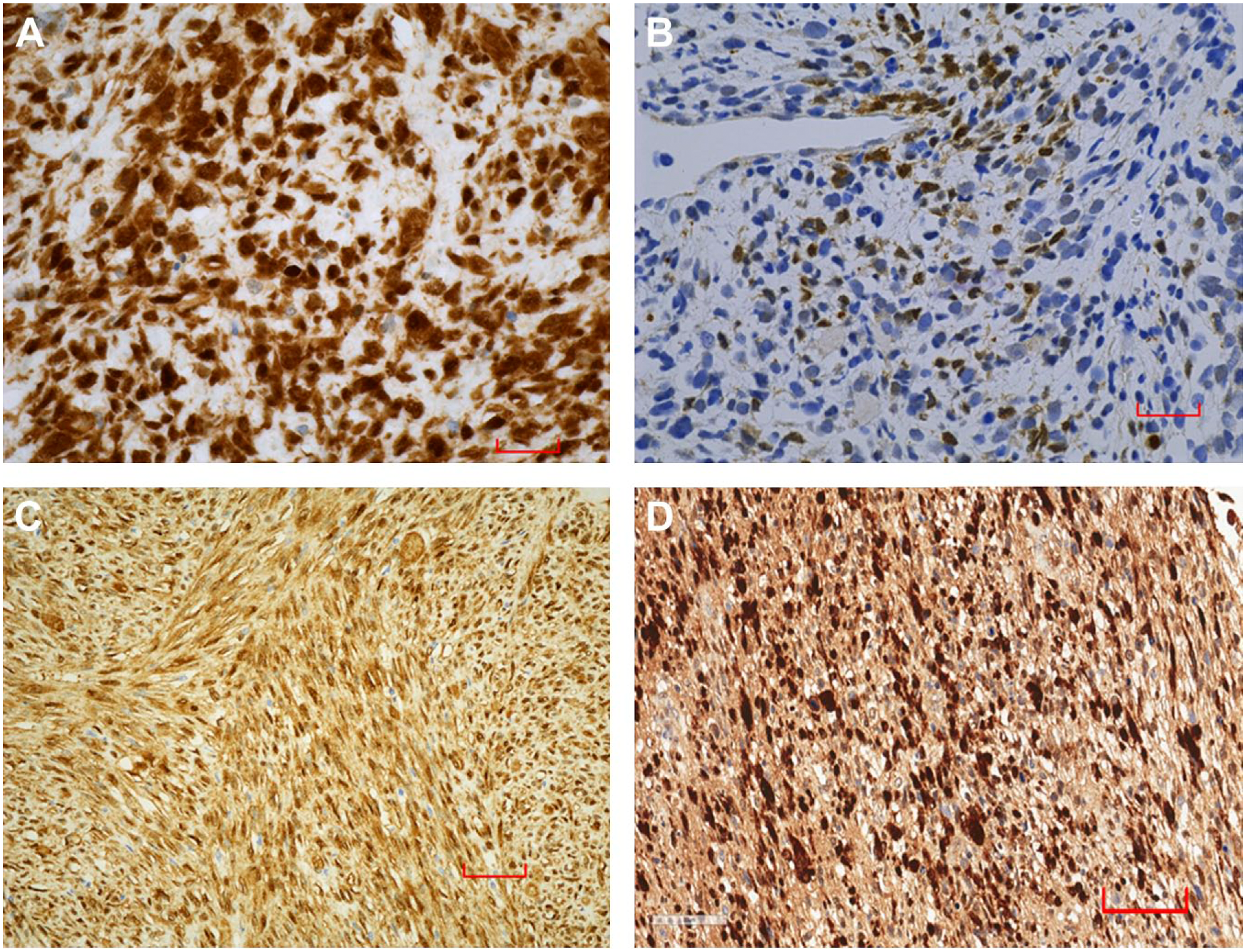
Nuclear and cytoplasmic YAP staining was present diffusely in all the tumor cells (A: ×400) and focally (B: ×400) in two different cases of embryonal rhabdomyosarcoma. Spindle cell sclerosing (C: ×200) and pleomorphic (D: ×200) also revealed diffuse staining.
Results of Positive Nuclear YAP Staining in the TMA Versus Whole Slides.
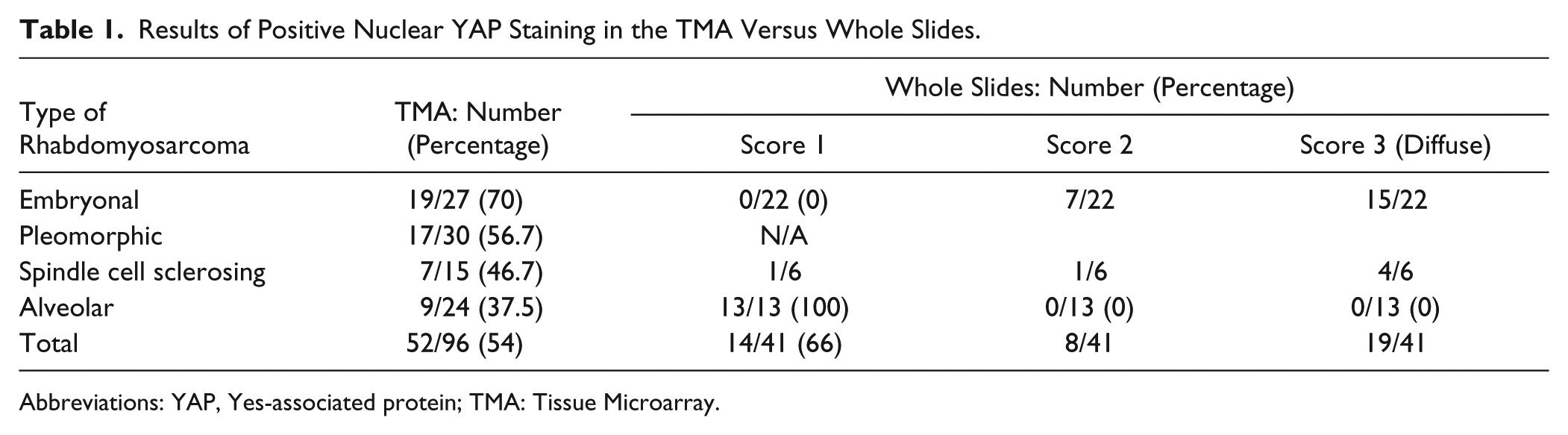
Abbreviations: YAP, Yes-associated protein; TMA: Tissue Microarray.
Clinical Characteristics and Staining Patterns of Cases in TMA Versus Whole Slides.
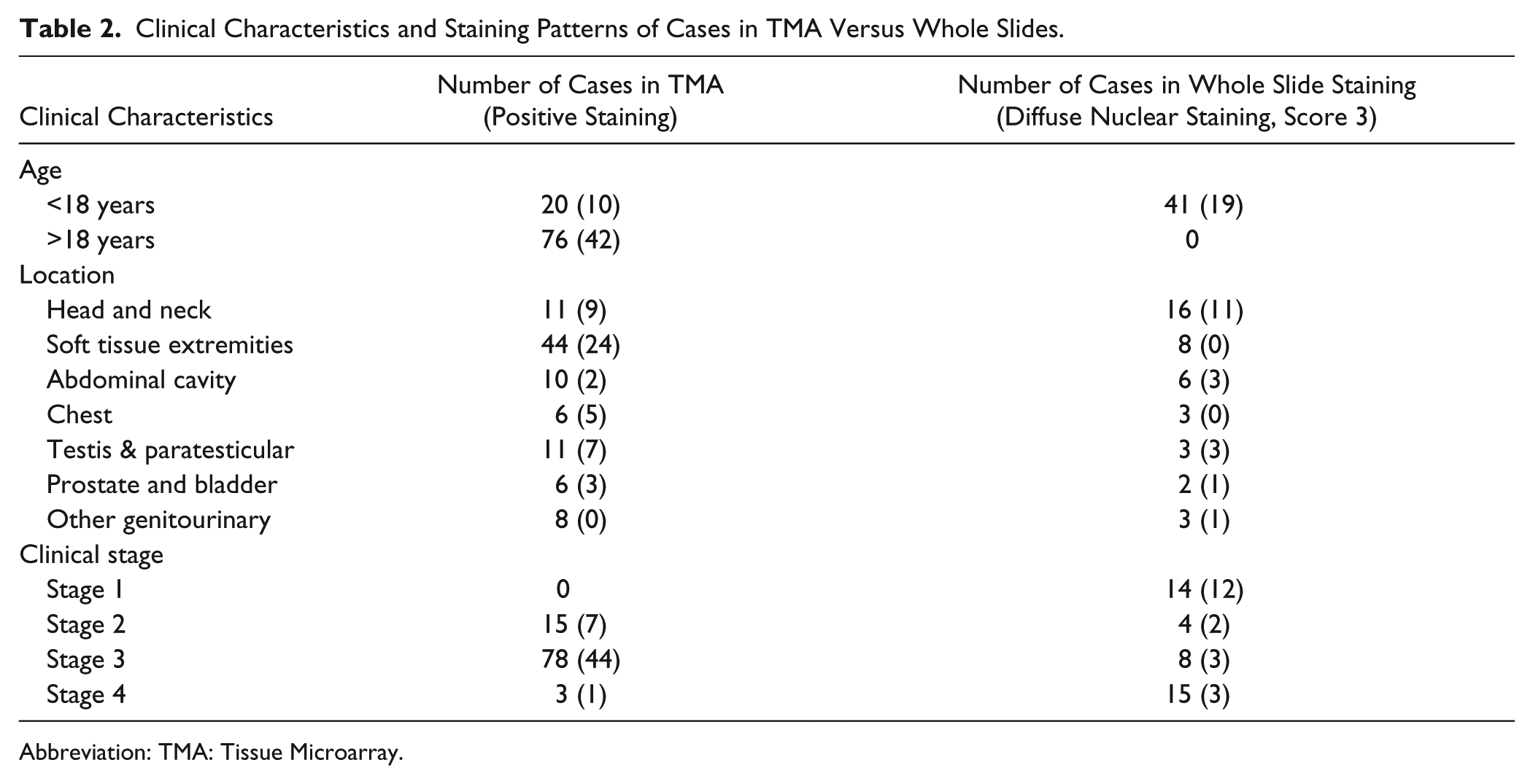
Abbreviation: TMA: Tissue Microarray.
Whole Slide Study
A total of 43 cases was selected for whole slide staining; all patients were <18 years at the time of the diagnosis. Diagnoses included 13 cases of ARMS, 24 cases of ERMS (including 7 with anaplasia), and 6 cases of SRMS. No PRMS cases were present, and 2 ERMS cases were excluded afterward because of inadequate tissue. Tumors were located in the head and neck (n=18, of which 16 were ERMS), soft tissue (n=8; all ARMS), abdominal cavity (n=6), testis and paratesticular areas (n=3), chest (n=3), prostate and bladder (n=2), and other genitourinary areas (n=3). The PAX3/PAX7 gene transfusion status was positive in 12 cases of ARMS and was unknown in 1 case.
Of the non-alveolar RMS (i.e., ERMS and SRMS), positive staining for YAP was seen in 27/28 (96%) cases (Table 1). The staining was strong nuclear with proportionate cytoplasmic staining (Fig. 1). Diffuse nuclear staining (score 3) was seen in 19/28 cases, and 8 cases showed score 2 staining (mostly 50–79%) with no preferential distribution in any particular histological subtype, age, gender, or tumor location (Table 2). Only 1 case of the SRMS category was negative. In contrast, ARMS cases had significantly lesser degree of nuclear staining, and cytoplasmic staining was more predominant (Fig. 2). Although nuclear staining was present in all the cases, it was restricted to <30% of tumor cells (score 1), and 6 cases had only minimal (1% or less) staining. For the diagnosis of ARMS, YAP staining of <30% has a 100% sensitivity, specificity of 96.6%, and a positive predictive value of 93% (Table 3). In ARMS, YAP staining showed a tendency to negatively correlate with myogenin staining, which was diffuse in all cases (Fig. 3).
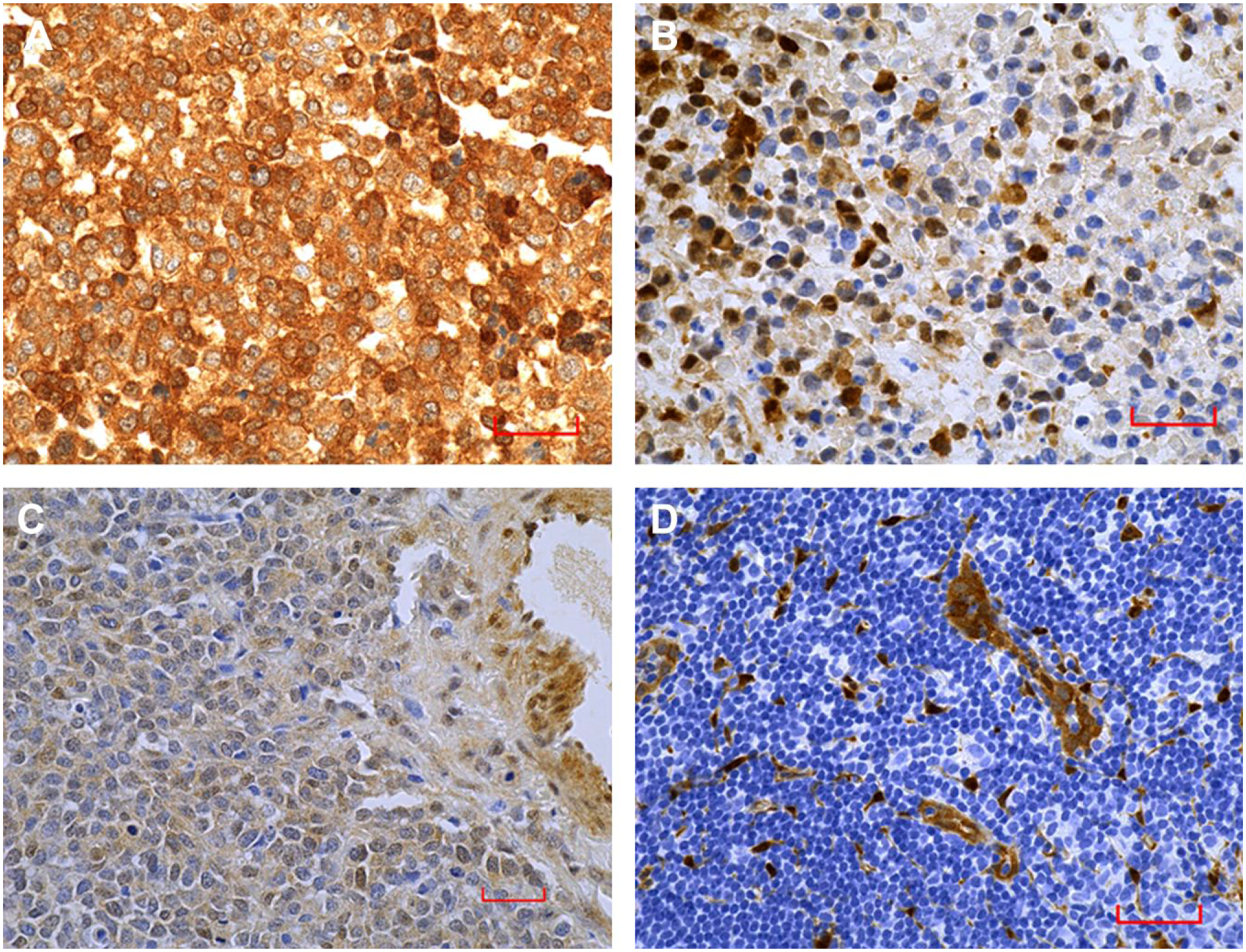
Alveolar rhabdomyosarcoma cases showed prominent cytoplasmic staining with only scant (A: ×400) or restricted (<30%) staining (B: ×400). Weak staining that is less intense than internal positive control was considered negative (C: ×400). Positive staining in blood vessels and negative staining of lymphoid cells and inflammatory cells served as internal positive and negative controls, respectively (D: ×200). Scale bar = 200 µm.
The Value of Restricted YAP Staining (Score 1) in Differentiating ARMS From Other Subtypes.
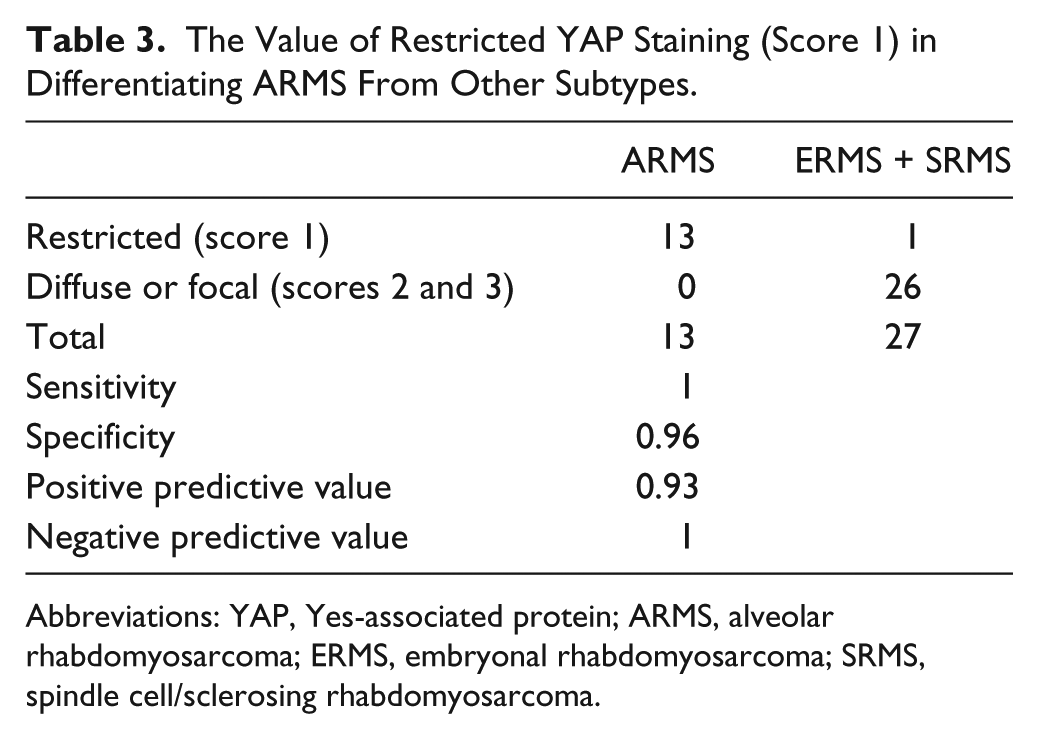
Abbreviations: YAP, Yes-associated protein; ARMS, alveolar rhabdomyosarcoma; ERMS, embryonal rhabdomyosarcoma; SRMS, spindle cell/sclerosing rhabdomyosarcoma.
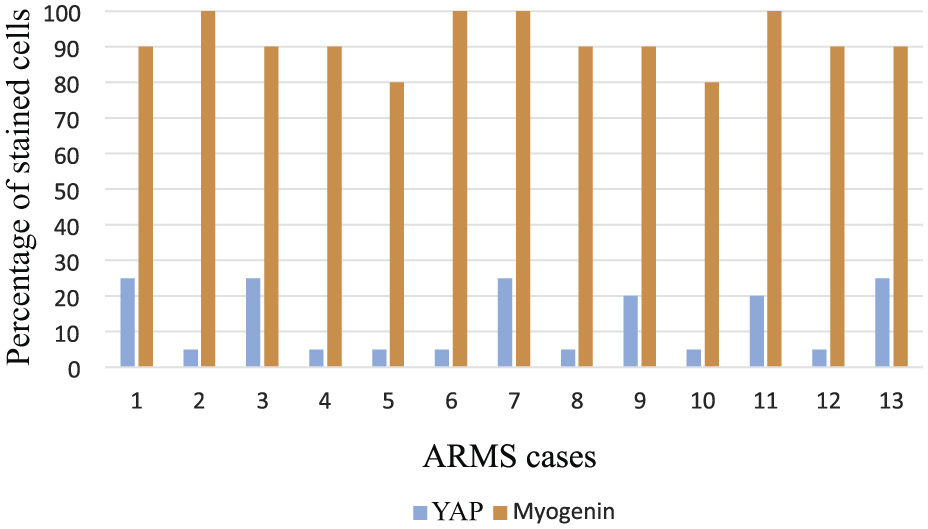
A column chart comparing the staining of ARMS cases with YAP and myogenin. The x-axis represents percentage of cells with nuclear staining. Abbreviations: ARMS, alveolar rhabdomyosarcoma; YAP, Yes-associated protein.
Table 2 shows that tumors with lower clinical stages (stage 1 and 2) have more diffuse YAP staining than patients with higher clinical stages (stage 3 and 4), and the difference is statistically significant (p=0.001). This difference reflects the influence of histology on the clinical stage; the clinically aggressive ARMS cases present mostly with stages 3 and 4 while tumors in early stages are more likely to be ERMS.
Discussion
This immunohistochemical study revealed the variable expression of YAP in different subtypes of RMS where it can be identified in the cytoplasm and the nucleus. Despite the heterogeneity of the patients’ populations and sampling methods, YAP nuclear staining is clearly more prevalent in embryonal than ARMS, thus, suggesting different roles and mechanisms of tumorigenesis. While YAP mutations have not been identified in this tumor, the increased protein expression most likely results from cross-talk with other activating pathways.10,12 Preclinical studies have shown that Hippo pathway suppression and subsequent YAP activation can occur through interaction with various members of the RAS proteins family, which are implicated as tumor suppressors in many cancers. In embryonal RMS, the upregulation of YAP protein is caused by interaction with the activated MAPK/ERK, Notch, and PI3K/AKT pathways, all of which, in addition to RAS mutations, have been described in this tumor.13,14 The increased YAP translocates to the nucleus where it binds TEADs family and activates proliferation genes. Of interest to note is that TEAD fusion with the transcriptional co-activator for steroid and nuclear hormone receptors (NCOA2) was found in an SRMS tumor tissue removed from a 4-week-old child. 15
However, PAX3/FOX01 fusion in ARMS leads to the upregulation of the RAS-association domain RASSF4, which in turn leads to the suppression of Hippo pathway and overexpression of YAP. 16 In view of our results, it seems that YAP, unlike in ERMS, does not significantly translocate to the nucleus and is retained in the cytoplasm. Thus, ARMS may upregulate other nuclear mechanisms of growth and proliferation. Clearly, further studies are needed to highlight the mechanism and the role of YAP upregulation in ARMS.
Recent studies have shown that YAP may be more important in the pathogenesis of ERMS than other subtypes. YAP copy number and protein expression were significantly increased in ERMS subtypes compared with ARMS.13,17 Using multiple genetically engineered mice, it was shown that YAP protein overexpression could transform activated satellite cells leading to the development of embryonal RMS-like tumors. 17 This suggests that YAP upregulation in ERMS is critical for its initiation.13,17 Immunohistochemical expression of YAP was increased in embryonal compared with ARMS. In concordance, our study has revealed that the nuclear YAP is more prevalent in ERMS than ARMS. This finding may have important implications in planning effective targeted therapy against YAP.
In a previous study based on TMA slides, YAP expression in ERMS was associated with higher clinical stage and poor survival. 17 A similar trend was also revealed in our TMA cases. However, the whole slide study has shown that nuclear YAP expression is more universal in all non-ARMS variants (i.e., ERMS and SRMS) without any predilection to a certain clinical stage or a specific prognostic subtype. This difference might also be attributed to different staining protocols and different antibodies procured from different companies (Santa Cruz vs. Cell Signaling), yielding unstandardized staining. Because of our limited whole slide sample size, more studies are needed to clarify the association of YAP staining with the prognosis.
Lack of significant nuclear YAP staining in ARMS cases may offer a diagnostic value in the sense that restricted staining (<30%) favors ARMS rather other ERMS. The histology of RMS may not be clearly indicative of the subtypes, and morphologic overlap may exist. In most cases, the presence of small round tumor cell morphology and the molecular demonstration of fusion transcripts is diagnostic of ARMS. 18 However, up to 20% of ARMS may be negative for the PAX3 or PAX7 translocations, and ERMS may exhibit a dense histological pattern, thus, resembling ARMS. 19 In such cases, where there is difficulty in the accurate classification of RMS, minimal or restricted YAP staining may offer diagnostic help, especially if combined with diffuse myogenin expression.20,21 Differences in the nuclear staining of alveolar versus embryonal subtypes was also noted in the previous study of Tremblay et al. 17
Our results also highlight the staining difference between TMA and whole slides. While only 37.5% of ARMS had staining in the TMA slide, all of the whole slide cases had nuclear staining. However, the staining was more restricted in distribution where it was seen in <30% of the cells. This emphasizes the importance of adequate sampling and tissue representation. Differences in formalin-fixation and differences in the size of two different sampled populations (96 versus 43) were additional factors that could have exaggerated the apparent discrepancy. However, the general conclusion that YAP nuclear staining is less prevalent in ARMS compared with other RMS types could still be achieved with either method.
In conclusion, YAP protein is widely expressed in RMS tumor cells, reflecting its role in sarcomagenesis. YAP nuclear staining is broadly present but is more prevalent in ERMS than ARMS, where the staining is noted in less than 30% of tumor cells. This fact is potentially helpful in differentiating ARMS from ERMS. Further standardization of the YAP antibody to detect only the unphosphorylated nuclear protein will offer more chances for better discriminatory studies in the future.
Footnotes
Acknowledgements
We would like to acknowledge the work of Joan Whiting in performing the IHC experiments and thank the Department of Pathology at Children’s Mercy Hospital for letting us use their resources.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have contributed to this article as follows: provided essential clinical information (NW, CC), designed the research (AAA), provided statistical analysis (AKS), analyzed the data (AAA, SSH, SQY), finalized the manuscript (AAA, MGT), and all authors have read and approved the manuscript as submitted.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.