
Abstract
Tumor hypoxia is associated with more aggressive behavior and resistance to chemotherapy and radiotherapy. Carbonic anhydrase IX (CA9) level increases under hypoxia and is related to poor prognostic factors. The aim of this study was to evaluate the expression of CA9 and to identify its prognostic significance in small intestinal carcinomas (SICs). CA9 expression was observed in 36% (63/175) of SICs. CA9 expression showed significant correlation with well- and moderately differentiated tumors compared with poorly differentiated tumors (p=0.039), tumors with no lymph node metastasis (p=0.005), and lower stage carcinomas (p=0.009). CA9 expression showed an inverse correlation with perineural invasion (p=0.021) and lymphatic invasion (p=0.022). No significant correlation was observed between CA9 expression and gross type, histological type, pathological tumor (pT) classification, vascular invasion, pancreas invasion, and retroperitoneal seeding. SICs with CA9 overexpression showed better overall survival compared with those with no or weak CA9 expression (p=0.048). In the multivariate analysis, poorly differentiated SICs (p<0.001) and SICs with lymph node metastasis (p=0.002) were independent poor prognostic factors. CA9 expression in SICs is more frequently associated with good prognostic markers and better overall survival; however, it is not an independent prognostic factor.
Introduction
Tumor hypoxia has been widely studied for the identification of better treatment modalities and for improvements in patient outcome. Hypoxia regulates tumor growth-enhancing mechanisms, such as angiogenesis, cell proliferation, genomic instability, and tissue invasion, and induces a tumor with resistance to radiation and chemotherapy (Brizel et al. 1996). In addition, intratumoral hypoxia has been found to be a potent stimulator of metastasis and is considered an indicator of more aggressive tumor behavior (Bertout et al. 2008).
CA9 is a stable transmembrane zinc metalloenzyme and the CA9 gene contains a hypoxia response component within its promoter region that is activated by hypoxia-inducible factors (Robertson et al. 2004). CA9 is involved in cell–cell adhesion and plays key role in the growth and survival of tumor cells under hypoxia (Choschzick et al. 2011). CA9 expression has been shown in many human cancers: gastric, breast, rectum, head and neck, and ovarian cancer, and has shown correlation with aggressive malignant behavior and poor outcome in these tumors (Hui et al. 2002; Driessen et al. 2006; Hussain et al. 2007; Korkeila et al. 2009; Choschzick et al. 2011).
Small intestinal carcinoma (SIC), a very rare tumor with poor overall outcome, is usually detected at an advanced stage due to its rarity and nonspecific symptoms. Lymph node metastasis and the distal location of these tumors (in the jejunum and ileum) are reported to be the most important independent prognostic factors of SICs (Chang et al. 2010). Therefore, efforts have focused on the identification of better molecular targets for adjuvant chemotherapies following surgical resection and the identification of new biomarkers for early detection. However, because of its rarity, the molecular carcinogenesis of SIC is still poorly understood and survival rates have shown little improvement over the last decade. Despite the important role played by CA9 during tumor development and progression in many cancers, its prognostic significance in SIC has not been studied.
Therefore, the purpose of this study was to evaluate the prognostic significance of CA9 expression in a large series of SICs.
Materials and Methods
Case Selection
This study focused on primary solitary carcinomas originating in the mucosa of the small intestine. A total of 194 cases of surgically resected SICs (by excision, resection, and pancreas-preserving pancreatoduodenectomy) from 1995 to 2009 were collected from 22 institutions across South Korea. Tumors with solitary or predominant involvement of the mucosa, irrespective of extension into the serosa, were considered primary SIC. Metastatic tumors and carcinomas extending into the small intestine from surrounding organs of the gastrointestinal tract, including the ampulla of Vater, pancreas, distal common bile duct, cecum, or stomach were excluded from this study. Histology from all tumor specimens was initially evaluated by gastrointestinal pathologists from each institution and finally reviewed by MJG. Medical records and pathology reports were reviewed for determination of patient’s age, sex, most recent follow-up dates, survival status, presence or absence of disease in relation to the occurrence of SIC, and the use of additional prior or current treatment modalities, such as chemotherapy and/or radiation therapy. Microscopic characteristics that were evaluated included the depth of invasion; the degree of differentiation; the histological subtype; the presence of lymphatic invasion, vascular invasion, pancreas invasion or perineural invasion; retroperitoneal tumor seeding; or metastasis to the regional lymph nodes. This study was approved by the Human Ethics Review Board of Yeungnam University Hospital (YUH-13-0463-O71).
Construction of Tissue Microarray Blocks
We constructed tissue microarrays (TMAs) of SIC cases from archival formalin-fixed, paraffin-embedded tissue blocks. We selected a representative tumor block containing adjacent normal mucosa for each case. Four or five 1-mm diameter tissue cores (two or three tumor cores, one normal small intestine mucosa, and one from a concurrently excised metastatic lymph node) were retrieved from each tumor block and transferred to the recipient block, as previously described (Chang et al. 2010). Tumor areas underlying ulcers or containing extensive necrosis were avoided for the construction of TMAs. Controls included normal liver, spleen, kidney, placenta, and colorectal adenocarcinoma. Among the 194 cases, 175 cases were finally available, the reduction in number due to tissue loss.
Immunohistochemistry and Interpretation
TMA sections were subjected to immunohistochemistry with CA9 (1:250, clone EPR4151, rabbit monoclonal antibody, Epitomics, CA). Staining was performed on an automated BenchMark® platform (Ventana Medical Systems, Tucson, AZ) using the onboard heat-induced epitope retrieval method in high-pH cell conditioning (CC)-1 buffer (Ventana Medical Systems) at 99C for 1 hr. Slides were then incubated with antibody CA9 at room temperature for 40 min. The UltraView™ universal DAB detection kit (Ventana Medical Systems), which included a hydrogen peroxide substrate and a 3,3’-diaminobenzidine chromogen solution, was used for visualization of staining. The slides were subsequently counterstained with hematoxylin.
We assessed CA9 expression using a four-step scoring system, as previously described (Choschzick et al. 2011). Scoring was as follows: negative = 0 (no staining or membranous staining <10% of tumor cells), weak = 1 (partial membrane staining >10% of tumor cells), moderate = 2 (weak to moderate complete membrane staining in >10% of tumor cells), and strong = 3 (strong and complete membrane staining in >10% of tumor cells). Finally, CA9 expression was considered positive if the score was greater than 2.
Statistical Analysis
Statistical comparisons were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL). The Chi-square test and Fisher’s exact test were performed to examine associations between clinicopathological factors and CA9 expression. Overall patient survival was defined as the time from surgical resection of SIC to death or last follow-up. The Kaplan-Meier method was used to calculate survival rate. The Cox proportional Hazard Model was used for evaluation of the association between clinicopathological parameters and survival. We determined the hazard ratio (HR) and associated 95% confidence interval (CI) for each factor. A p value of less than 0.05 was considered statistically significant.
Results
Characteristics of Patients
A total of 109 male and 66 female patients with a median age of 58.3 years (range, 23-85 years) were included in this study. Tumors were located in the duodenum in 95 cases (54.3%), the jejunum in 54 cases (30.9%), and the ileum in 26 cases (14.9%). Regarding growth features, there were 31 cases of polyploid (18.6%), 10 cases of nodular (6.0%), and 126 cases of infiltrative (75.4%) SIC. Tumor size ranged from 0.8 to 16 cm (mean, 4.4 cm). The time interval between the date of surgical resection and the date of death or last follow-up (overall survival) ranged from 1 to 128 months, with a median survival time at last follow-up of 24.9 months.
Regarding histological subtypes, there were 160 tubular adenocarcinomas (91.4%), 8 mucinous carcinomas (4.6%), 3 signet ring adenocarcinomas (1.7%), and 4 undifferentiated (2.3%) carcinomas. Regarding differentiation, there were 37 well-differentiated (21.1%), 98 moderately differentiated (56.0%), 36 poorly differentiated (20.6%), and 4 undifferentiated (2.3%) SICs. Vascular and lymphatic invasion were observed in 44 (25.1%) and 84 (48.0%) cases, respectively. Pancreatic invasion was observed in 62 cases (35.4%). Eighty-two (50.9%) cases showed metastasis to regional lymph nodes. Retroperitoneal tumor seeding was observed in 13 cases. Regarding pTNM (pathological Tumour, Node, Metastases) staging, pTis (carcinoma in situ) was observed in 4 cases (2.3%), pT1 (level 1) in 6 cases (3.4%), pT2 in 9 cases (5.1%), pT3 in 56 cases (32.0%), and pT4 in 100 cases (57.1%). A pN0 was observed in 78 cases (48.4%), pN1 in 55 cases (34.2%), and pN2 in 28 cases (17.4%). None of the patients showed distant metastasis. Regarding the American Joint Committee on Cancer (AJCC) staging system, there were two cases in stage 0 (1.2%), 12 cases in stage I (7.5%), 65 cases in stage II (40.4%), and 82 cases in stage III (50.9%). Regarding predisposing conditions, there were 17 cases with sporadic adenoma, three cases with Peutz-Jeghers syndrome, two cases with Meckel diverticulum, and 1 case with Crohn’s disease. Seventy-four patients underwent chemotherapy and 25 patients received radiotherapy after surgical resection.
Immunohistochemical Results for CA9 and Its Clinicopathological Significance
Overall, 63 (36.0%) of the 175 SICs were positive for CA9 (Fig. 1). CA9 expression showed significant correlation with better differentiation, absence of lymph node metastasis, lower stage, and absence of perineural and lymphatic invasion (Table 1). CA9 expression was evident in well- and moderately differentiated SICs compared with poor and undifferentiated SICs (p=0.039), and showed an association with no lymph node metastasis (p=0.005) and lower stage (p=0.009). CA9 expression showed an inverse correlation with perineural invasion (p=0.021) and lymphatic invasion (p=0.022). No significant correlation was observed for CA9 expression with gross type, histological type, pT, vascular invasion, pancreas invasion, or retroperitoneal seeding. SICs with CA9 expression showed better overall survival than those without CA9 expression (p=0.048, 66.5 months vs. 26.3 months) (Fig. 2).
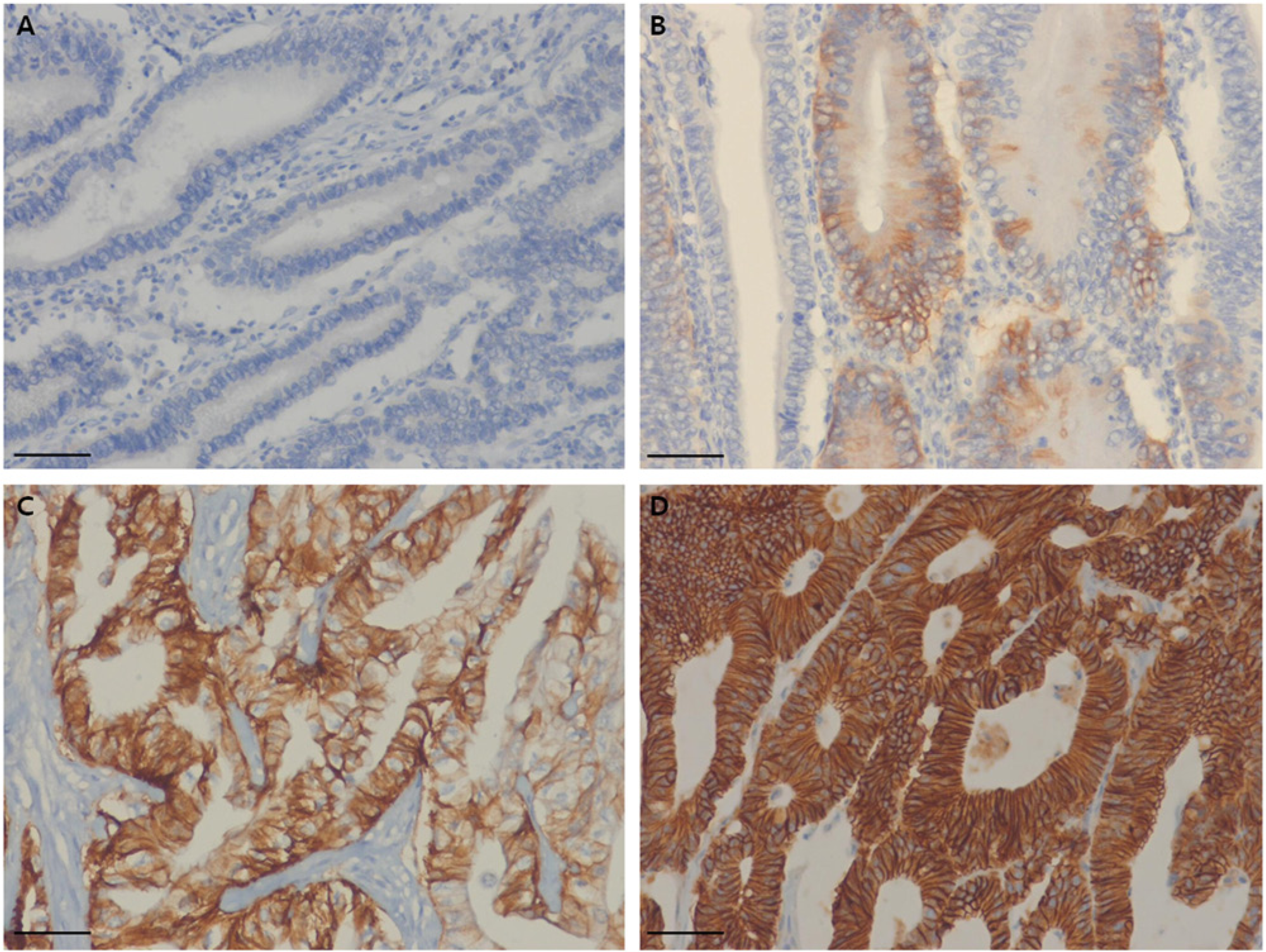
Immunohistochemical results for CA9. (A) Negative (no staining or membranous staining <10% of tumor cells), (B) weak (partial membrane staining >10% of tumor cells), (C) moderate (weak to moderate complete membrane staining in >10% of tumor cells) and (D) strong (strong and complete strong membranous expression). Scale Bars =100 µm.
Relationship between Clinicopathological Factors and CA9 Expression.
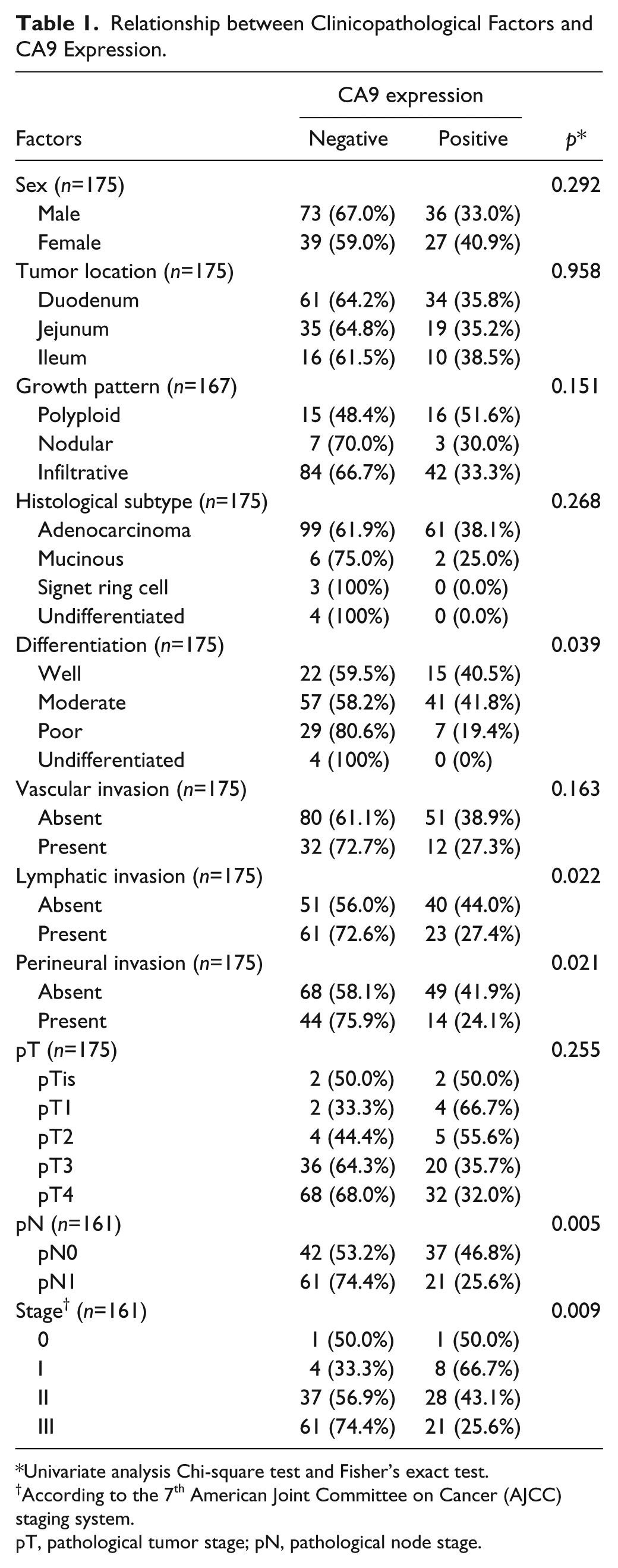
Univariate analysis Chi-square test and Fisher’s exact test.
According to the 7th American Joint Committee on Cancer (AJCC) staging system.
pT, pathological tumor stage; pN, pathological node stage.
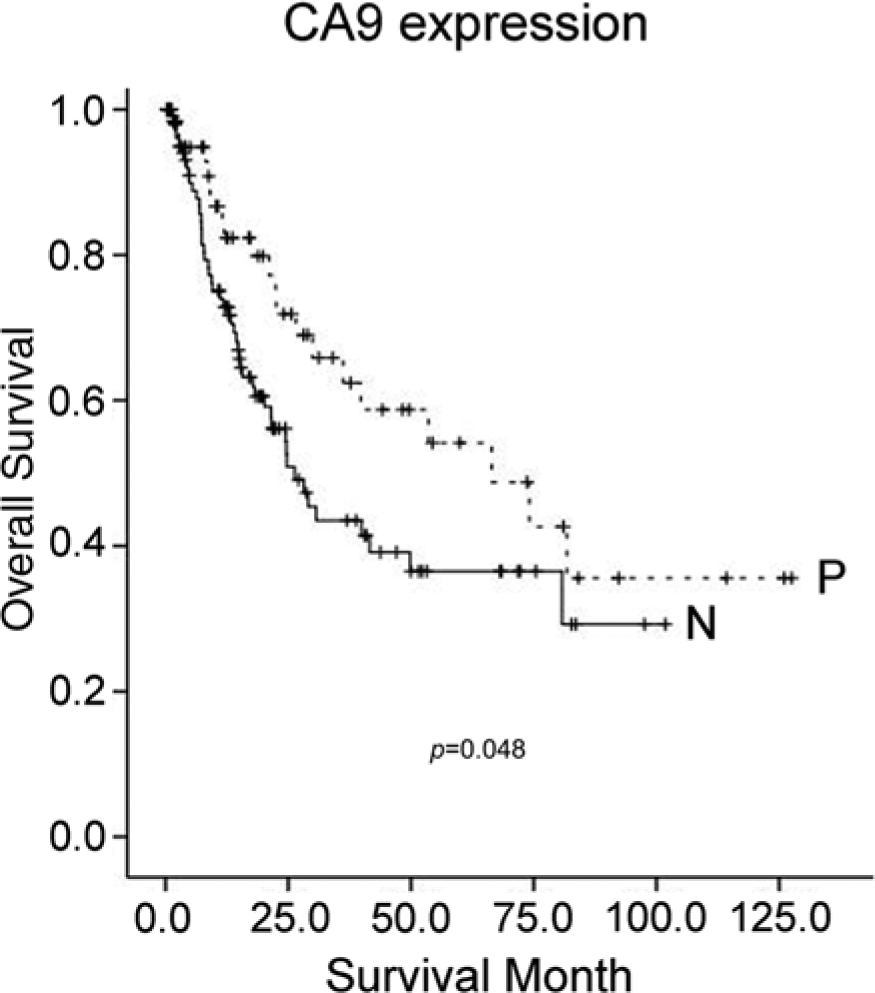
Overall survival analysis. Small intestinal carcinoma with CA9 expression (P) shows better overall survival than that with no or weak expression (N) (p=0.048, 66.5 months vs 26.3 months).
In the multivariate analysis, patients with poorly differentiated SICs showed a 51-fold higher risk of death compared with those with well-differentiated SICs (95%CI 9.060-290.693, p<0.001) and SIC patients with lymph node metastasis showed a 48-fold higher risk of death than those without metastasis (95%CI 4.015-582.184, p=0.002) (Table 2). CA9 expression was not an independent prognostic factor.
Variables Associated with Risk of Death.
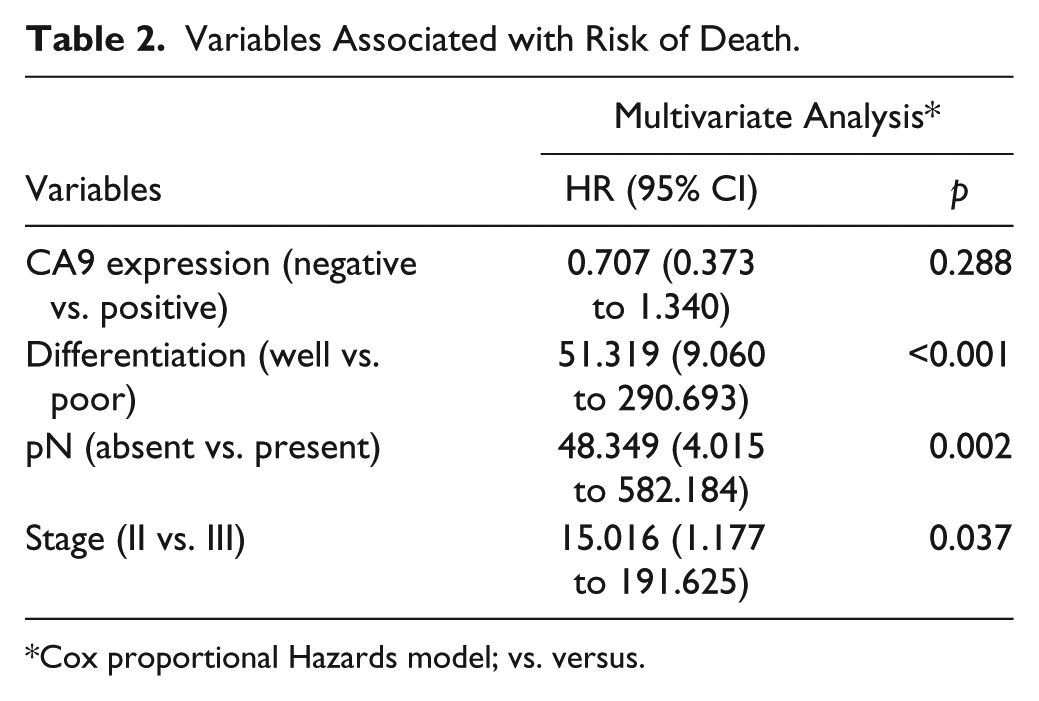
Cox proportional Hazards model; vs. versus.
Discussion
The clinical significance of tumor hypoxia is its association with a more aggressive malignant behavior, and resistance to chemotherapy and radiotherapy (Brizel et al. 1996; Hussain et al. 2007). CA9, a transmembrane zinc metalloenzyme, is induced by hypoxia and plays an important role in tumor growth and survival under normoxia and hypoxia (Ilie et al. 2010). Its expression is restricted primarily to premalignant and malignant cells and is rarely found in normal tissue or benign lesions (Driessen et al. 2006). In carcinoma of the gastrointestinal tract, except for the small intestine, CA9 expression has been reported in 34% to 80% of cases (Driessen et al. 2006). To the best of our knowledge, no previous studies have reported associations between CA9 expression and clinicopathological parameters or prognosis in patients with SICs.
Overexpression of CA9 has been reported in a wide variety of human carcinomas, including upper gastrointestinal cancer, breast cancer, ovarian cancer, nasopharyngeal cancer, and rectal cancer, and its prognostic value has been associated with tumor aggressiveness and poor outcome (Hui et al. 2002; Driessen et al. 2006; Hynninen et al. 2006; Hussain et al. 2007; Korkeila et al. 2009; Choschzick et al. 2011). However, the opposite results have been demonstrated in renal cell carcinoma, gallbladder adenocarcinoma, rectal cancer, gastric cancer, and cervical cancer. Increased expression of CA9 in renal cell carcinoma, gallbladder carcinoma, and rectal cancer showed correlation with favorable survival (Atkins et al. 2005; Rasheed et al. 2008; Sergeant et al. 2011; Takacova et al. 2013). Low CA9 expression and the absence of von Hippel–Lindau (VHL) disease mutation showed an association with a poor clinicopathological phenotype and shorter survival in renal cell carcinomas (Patard et al. 2008). CA9 expression showed an inverse correlation with histological differentiation and showed an association with favorable prognosis in patients with gallbladder carcinoma (Sergeant et al. 2011). Rectal cancer patients with CA9 expression showed long-term survival compared with those patients with rectal cancer with no or weak CA9 expression (Rasheed et al. 2008). These results have been explained by the fact that cumulative genetic mechanisms involved in cancer progression alter the hypoxic pathway, leading to consistently low CA9 expression (Rak et al. 2002). In this study, CA9 overexpression showed significant correlation with well/moderate differentiation rather than a lack of differentiation, no lymph node metastasis, and lower stage, and patients showed better overall survival as compared with patients with tumors that showed no or weak expression. Higher CA9 expression was observed in lower pT than in higher pT (pTis, pT1, pT2 vs pT3, pT4: 57.9% vs 33.3%) without statistical significance. CA9 expression was more frequently observed in lower stage (stage 0 and I) than in stage II and stage III tumors. The abovementioned findings might imply that CA9 is a simple hypoxic marker or that the CA9-related hypoxic pathway participates in the early stage of SIC carcinogenesis. Therefore, other mechanisms may be necessary for tumor progression, invasion, and metastasis of SIC.
The importance of CA9 expression as a predictive marker to guide in the selection of the most appropriate adjuvant therapy has been demonstrated, because tumor hypoxia has been associated with tumor resistance to chemotherapy and radiotherapy as well as a more aggressive phenotype and poor survival (Hussain et al. 2007). A clinical trial for the evaluation of a CA9-targeting agent in renal cell carcinoma was recently conducted. However, the results of the current study suggest that a CA9-targeting therapy in SIC may not be useful in the improvement of patient outcomes.
In conclusion, CA9 expression in SICs was more frequently associated with good prognostic factors, such as well and moderate differentiation, no lymph node metastasis, and lower stage. SIC patients with CA9 expression showed better overall survival than those with no or weak expression. Thus, CA9 expression in SICs was not an independent prognostic factor.
Footnotes
Acknowledgements
We would like to thank the members of the Korean Small Intestinal Cancer Study Group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.