
Abstract
The human cervical cancer oncogene 1 (HCCR-1), a novel human oncoprotein, has been shown to be upregulated in various human tumors and plays a critical role in tumorigenesis and tumor progression. Here, the authors investigated HCCR-1 level in esophageal squamous cell carcinoma (ESCC) tissues and assessed the correlation between HCCR-1 level and prognosis of the patients with ESCC. HCCR-1 levels were investigated by immunohistochemistry, in situ hybridization, real-time quantitative RT-PCR and Western blotting methods; Kaplan-Meier curve was used to evaluate the prognostic value of HCCR-1 level in patients with ESCC using log-rank test. HCCR-1 displayed high levels in ESCC tissues compared to squamous dysplasia tissues and normal esophageal epithelial tissues. No significant correlation was observed between the levels of HCCR-1 mRNA and protein and gender and age (all p>0.05) but obviously related to histological grade, clinical stage, and lymph node metastasis (all p<0.001). Moreover, the survival rate of the patients with low HCCR-1 levels was higher than that of the patients with high HCCR-1 levels (both p<0.05). These data demonstrate that HCCR-1 may be used as a novel predictor for the prognosis of the patients with ESCC.
Keywords
Esophageal cancer, a highly aggressive neoplasm, is the ninth-most-common malignancy and the sixth-most-common cause of cancer death in the world (Siersema 2008). Based on histological examination, esophageal cancer includes two histological types: adenocarcinoma and squamous cell carcinoma, both with an equally poor prognosis. Although the incidence of the former has increased in the United States and Europe over the past three decades, esophageal squamous cell carcinoma (ESCC) is still the dominant histological type worldwide (Ekman et al. 2008). Moreover, there is wide geographic variation in the incidence of esophageal cancer, with the highest rates occurring in China, South-Central Asia, and Eastern and Southern Africa (Parkin et al. 2005), especially in Linzhou and Anyang city of Henan province, China (Yang 1980). Currently, 5-year survival rates of ESCC are also dismal (5–10%), with over 50% of patients harboring distant metastases at the time of presentation (Enzinger et al. 1999; Edwards et al. 2005). Therefore, it is particularly important to seek new powerful molecular markers to diagnose ESCC and improve the prognosis of patients with ESCC.
Human cervical cancer oncogenes (HCCRs), which are overexpressed in primary cervical cancers and cervical cancer cell lines (Ko et al. 2003), were firstly identified in primary cervical cancers and cervical cancer cell lines by differential display RT-PCR approach (Ko et al. 2003; Ko et al. 2004; Chung and Kim 2005). HCCR oncogenes are mainly classified into two isoforms according to molecular features: HCCR-1 and HCCR-2 (Ko et al. 2003). However, currently, a large number of studies mainly focus on the relationship between HCCR-1 and tumors. It is well documented that HCCR-1 is upregulated in many different tumors and implicated in the progression of tumors including the carcinoma of hepatocellular (Jirun et al. 2011), pancreatic (Xu et al. 2010), colon (Shin et al. 2006), and breast (Jung et al. 2005; Ha, Lee, et al. 2009; Ha, Shin, et al. 2009). Additionally, HCCR-1 has been identified as a novel oncogene with strong tumorigenic features in nude mice, and its role in tumorigenesis may be in the negative regulation of the p53 tumor suppressor gene (Ko et al. 2003). All data suggest that HCCR-1 might provide the fundamental function essential for tumor growth and survival, and play a pivotal role in the development and progression of tumors.
To date, the potential role of HCCR-1 in the occurrence and development of ESCC remains elusive. In the present study, we investigated the expression levels of HCCR-1 mRNA and protein in ESCC tissues, elucidated the clinical significance of HCCR-1 in patients with ESCC, and evaluated the relationship between HCCR-1 expression and prognosis of the patients with ESCC.
Materials and Methods
Tissue Samples
One hundred and fifty-eight cases of formalin-fixed paraffin-embedded ESCC tissues, 105 cases of squamous dysplasia tissues, and 158 cases of normal esophageal epithelial tissues obtained from the First Affiliated Hospital of Zhengzhou University were enrolled in this study. These specimens included 97 males and 61 females. In addition, 113 cases were from patients who were more than or equal to 60 years old, and 45 cases were from patients who were less than 60 years old. The mean age of the patients was 59.2 years (SD = 13.3). Regarding the histological grade, there were 51 cases of well-differentiated ESCC samples, 39 cases of moderately differentiated ESCC samples, and 68 cases of poorly differentiated ESCC samples. In addition, 63 cases of ESCC samples were pathological grades I and II, and 95 cases of ESCC samples were grades III and IV. Moreover, there was lymph node metastasis in 80 cases of the patients with ESCC but no metastasis in 78 cases. None of the patients received any form of treatment prior to surgery.
In Situ Hybridization Analysis
Human HCCR-1 probe comprising a 69-bp region of HCCR-1 cDNA (GenBank accession number: NM_015416) was amplified with HCCR-1-specific primers (forward: 5′-GACCCCAAAACAACAAACTGAT T-3′; reverse: 5′-GGGATGAC CTTTTCTAAATAACTAATA-3′) and labeled with Digoxigenin (Promega Corporation, Madison, WI) according to the manufacturer’s instructions. In situ hybridization (ISH) analysis for HCCR-1 mRNA expression was carried out according to previous description (Liu et al. 2010). Briefly, paraffin-embedded ESCC sections were incubated at 55C overnight. The slides were deparaffinized in xylene and graded alcohol. Heat pretreatment was performed in the pretreatment buffer at 98C to 100C for 15 min. The tissues were digested with pepsin for 10 min at room temperature (RT). Digoxigenin-labeled HCCR-1 probe was applied to the slides, covered with a coverslip, and edges sealed with rubber cement. The slides were then denatured on a hot plate at 96C for 5 min; and the hybridization reaction performed overnight at 37C using a moisturized chamber. Nitro blue tetrazolium chloride and 5-bromo-4-chloro-3-indolyl-phosphate (NBT/BCIP) stock solution were used as a chromogen substrate for visualization of the signal. PBS instead of HCCR-1 probe was used as a negative control.
Immunohistochemical Analysis
Immunohistochemical (IHC) analysis was performed as previously reported (Liu et al. 2010). In brief, 4-µm paraffin-embedded ESCC sections were placed in an oven overnight at 37C. The slides were dewaxed in xylene, rehydrated in graded alcohol, and incubated in 0.01 M citrate buffer at 95C for 20 min as antigen retrieval. After blocking for nonspecific antibody binding, the HCCR-1 monoclonal antibody (1:200) (Santa Cruz Biotechnology, Santa Cruz, CA) was applied. Signal visualization was developed by the avidin-biotin-peroxidase method using DAB. Following immunohistochemical staining assay, the slides were placed in hematoxylin for 1 min. As a negative control, we used tumor sections in which normal horse serum was used instead of the primary antibody.
Evaluation of Staining
Under a light microscope, all tissue sections were blindly investigated by two experienced pathologists. Evaluations of immunoreactivity of IHC and ISH were performed according to previous description (Liu et al. 2010). In brief, the scoring methods for HCCR-1 were as follows: the mean percentage of positive tumor cells was determined in at least five areas at 400-fold magnification and assigned one of the following five categories: 0, <5%; 1, 5–25%; 2, 25–50%; 3, 50–75%; and 4, >75%. The intensities of HCCR-1 cytoplasm staining were scored as follows: 1+, weak; 2+, moderate; and 3+, intense. The mean percentage of positive tumor cells and staining intensity were multiplied to produce a weighted score for each case. Cases with weighted scores <1 were defined as negative, and cases were otherwise defined as positive.
Real-Time Quantitative Reverse Transcription PCR
Real-time quantitative reverse transcription PCR (real-time qRT-PCR) was performed using standard SYBR Green real-time PCR method (Li et al. 2009; Wang et al. 2004). A total of six randomly chosen cases of ESCC tissues and paired normal esophageal epithelium tissues were used for real-time qRT-PCR. Briefly, total RNA was isolated from 50–100 mg of ESCC and normal esophageal epithelium tissues using TRIzol reagent (Promega Corporation, East Port, Prague, Czech Republic), and 1 µg of total RNA was subjected to reverse transcription using 300 U M-MLV Reverse Transcriptase (Life Technologies, Gaithersburg, MD). Real-time qPCR was performed on an ABI 7300 PCR instrument (Applied Biosystems, Foster City, CA) using three-stage program parameters provided by the manufacturer as follows: 2 min at 50C, 10 min at 95C, and then 40 cycles of 15 s at 95C and 1 min at 60C. Primers used for real-time qPCR analysis were designed using Primer Express software (Applied Biosystems) as follows: HCCR-1 (forward: 5′-CTACCTGGT CTTCTTGCTAATGT-3′; reverse: 5′-AGGGATGACCTTTT CTAAA TAACT-3′; product size: 157 bp) and β-actin (forward: 5′-GCGCGGCTA-CAGCTTCACCA-3′; reverse: 5′-GGGCAGCGGAACCG-CTCATT-3′; product size: 189 bp); β-actin was used for normalization. For each PCR, the reaction was carried out in a reaction mixture (25 µL) containing 1×reaction buffer (0.01 nmol of each primer, 0.25×SYBR green I, 200µmol/L deoxynucleotide triphosphate, 2 mmol/L MgCl2, and 1.5 units of TaqDNA polymerase). Specificity of the produced amplification product was confirmed by examination of dissociation reaction plots. A distinct single peak indicated that a single DNA fragment was amplified during PCR. Each sample was tested in triplicate using real-time qRT-PCR, and samples obtained from three independent experiments were used for analysis of relative gene expression data using the 2-ΔΔCt method (Livak and Schmittgen 2001).
Western Blotting Analysis
Western blotting protocol was performed according to standard methods as per a previous publication (Zeng et al. 2006; Li et al. 2010). In brief, six randomly chosen cases of ESCC tissues and paired normal esophageal epithelium tissues were lysed in a sample buffer (50 mM Tris-HCl, pH 8.0; 150 mM NaCl, 1% Triton X-100; 100 µg/ml PMSF) on ice for 30 min. Lysates were then centrifuged for 5 min (12,000×g, 4C). Protein concentrations were determined with standard Bradford method. An equal amount of tissue lysates (50 µg/lane) were electrophoresed through a 10% SDS-PAGE gel and then transferred to nitrocellulose membranes (Amersham, Uppsala, Sweden). The membranes were then blocked in 5% skimmed milk in PBS-T containing 0.05% Tween-20 at RT for 2 h and then incubated at RT for 2 h with corresponding primary antibodies including anti-HCCR-1 and anti-β-actin (all from Santa Cruz Biotechnology) diluted in 1% skimmed milk in PBS-T, respectively, followed by incubation with horseradish peroxidase–conjugated goat anti-mouse IgG. The bands of specific proteins on the membranes were developed with DAB. Quantification of band intensity was performed using Image-Pro Plus 5.0 software (Media Cybernetics, Silver Spring, MD).
Statistical Analysis
Statistical analyses were performed using the SPSS 13.0 statistical package (SPSS, Inc., Chicago, IL). The relationships between HCCR-1 at mRNA and protein levels and various clinicopathological parameters were evaluated with χ2 test. The relative levels of HCCR-1 mRNA and protein were analyzed using one-way ANOVA. Survival analyses were performed according to the Kaplan-Meier method using the log-rank test (Mantel-Cox). A value of p<0.05 was considered statistically significant.
Results
Overexpression of HCCR-1 mRNA in ESCC Tissues
In situ hybridization was utilized to detect HCCR-1 mRNA level in 158 cases of ESCC tissues, 105 cases of squamous dysplasia tissues, and 158 cases of normal esophageal epithelial tissues. The results demonstrated that HCCR-1 mRNA was mainly localized in the cytoplasm of esophageal cancer cells with purple-blue staining (Fig. 1). Of the 158 patients with ESCC, 122 (77.22%) were positive for HCCR-1 mRNA expression, whereas positive ratios of HCCR-1 mRNA expression in squamous dysplasia tissues and normal esophageal epithelial tissues were 36.19% (38 of 105) and 3.16% (5 of 158), respectively. Chi-square analysis revealed a significant increase in the expression of HCCR-1 mRNA in ESCC tissues as compared to squamous dysplasia tissues or normal esophageal epithelial tissues (p<0.001), suggesting that overexpression of HCCR-1 mRNA in ESCC tissues may be tightly associated with the emergence and progression of ESCC.
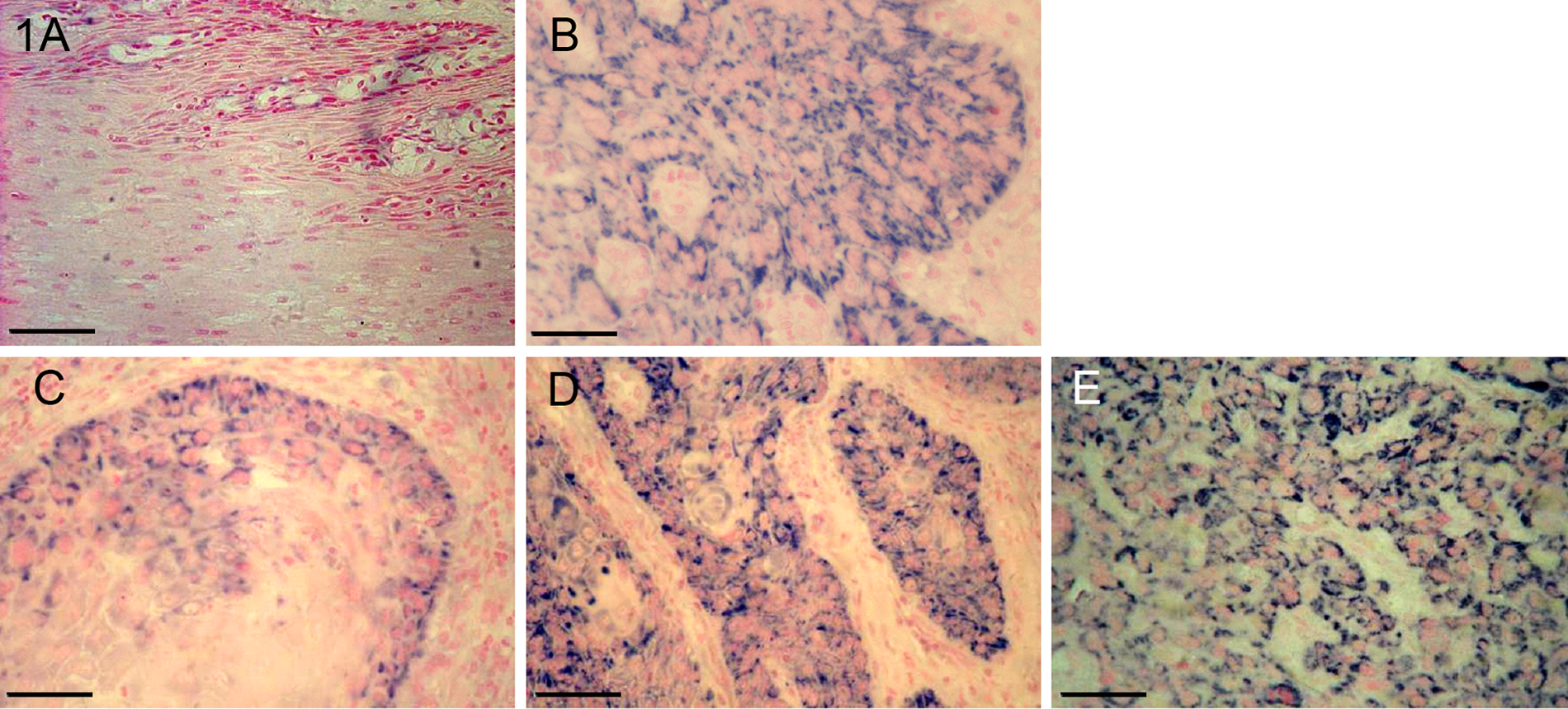
In situ hybridization detection for HCCR-1 mRNA expression in ESCC tissues, paracancerous tissues and its corresponding normal esophageal epithelial tissues. A: Negative expression of HCCR-1 mRNA in normal esophageal epithelial tissues; B: Weak positive expression of HCCR-1 mRNA in squamous dysplasia tissues; C: Moderate HCCR-1 mRNA staining in well-differentiated ESCC tissues; D: Strong HCCR-1 mRNA staining in moderately differentiated ESCC tissues; E: Stronger HCCR-1 mRNA staining in poorly differentiated ESCC tissues. Bar=100 µm.
Overexpression of HCCR-1 Protein in ESCC Tissues
Immunohistochemistry was employed to investigate the level of HCCR-1 protein in 158 cases of ESCC tissues, 105 cases of squamous dysplasia tissues, and 158 cases of normal esophageal epithelial tissues. The results revealed that HCCR-1 protein was mainly localized in the cytoplasm of esophageal cancer cells with brown staining (Fig. 2). Among all the 158 cases of ESCC and paired normal esophageal epithelial tissues, 126 (79.75%) and 6 (3.80%) displayed a positive expression of HCCR-1 protein, respectively, but there were 43 cases of positive expression of HCCR-1 protein in 105 cases of squamous dysplasia tissues. Compared to that of squamous dysplasia tissues and normal esophageal epithelial tissues, there was an obvious increase in the expression of HCCR-1 protein in ESCC tissues (p<0.001). These protein expression profiles in ESCC tissues indicate that HCCR-1 may function in the progression of ESCC. In addition, expressions of HCCR-1 mRNA and protein in ESCC tissues appeared to be positively correlated (p<0.001) (Table 1), suggesting that HCCR-1 mRNA or protein alone may be an ideal predictor for ESCC.
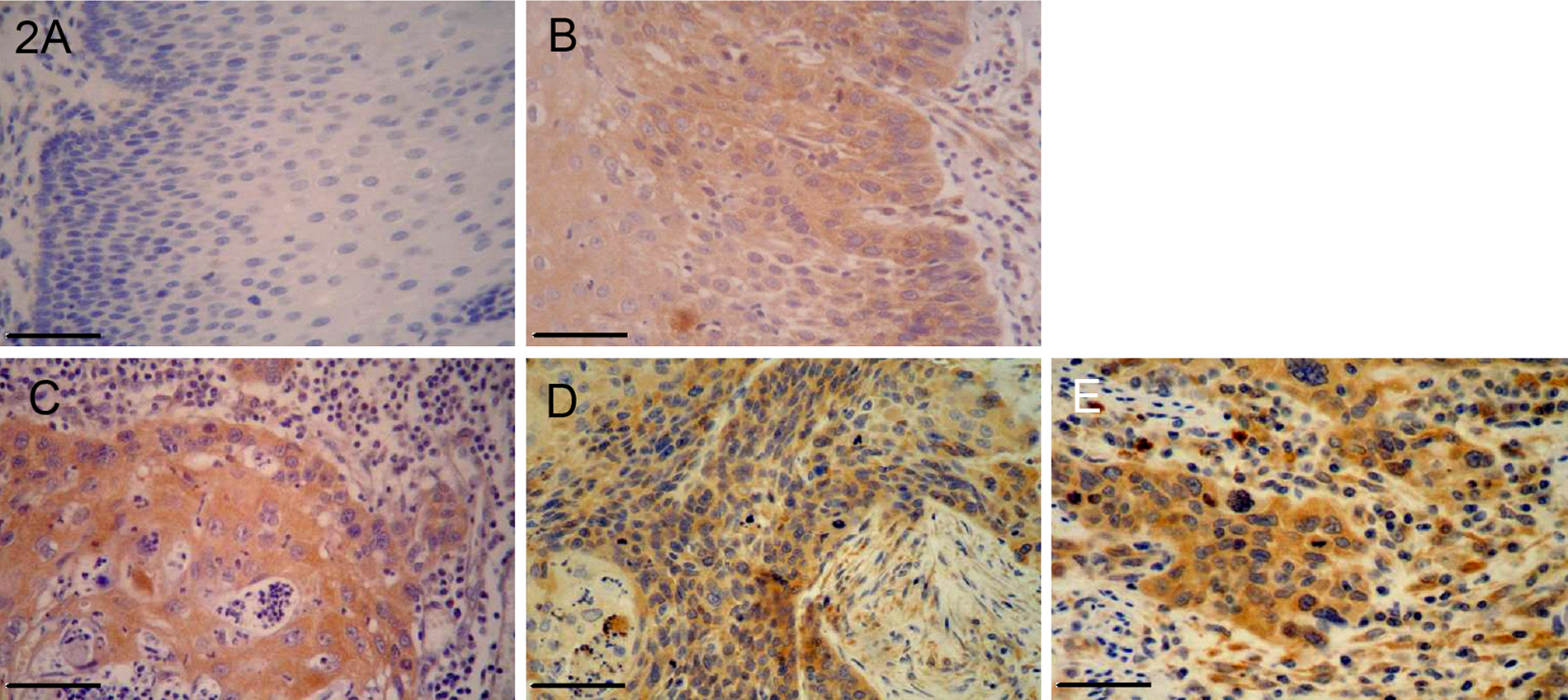
Immunohistochemistry analysis for HCCR-1 protein expression in ESCC tissues, paracancerous tissues and its corresponding normal esophageal epithelial tissues. A: Negative expression of HCCR-1 protein in normal esophageal epithelial tissues; B: Weak positive expression of HCCR-1 protein in squamous dysplasia tissues; C: Moderate HCCR-1 protein staining in well-differentiated ESCC tissues; D: Strong HCCR-1 protein staining in moderately differentiated ESCC tissues; E: Stronger HCCR-1 protein staining in poorly differentiated ESCC tissues. Bar=100 µm.
Correlation Analysis of HCCR-1 mRNA and Protein in ESCC Tissues

Relationship between Expressions of HCCR-1 mRNA and Protein and Clinicopathological Features in ESCC Tissues
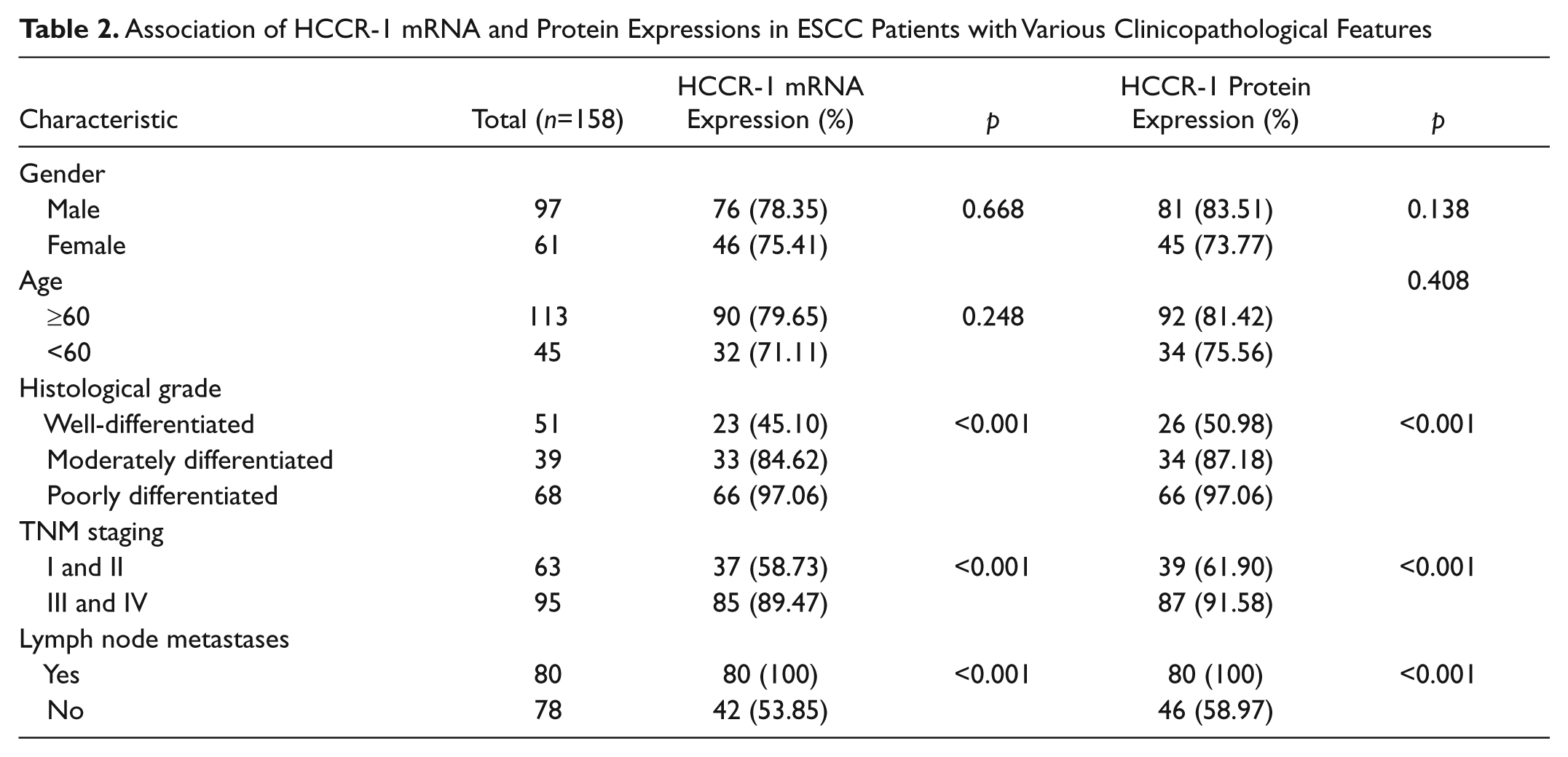
To clarify the role of HCCR-1 at mRNA and protein levels in the development and progression of ESCC, we analyzed the correlations between HCCR-1 at mRNA and protein levels and clinicopathological features, such as gender, age, histologic grade, clinical staging, and lymph node metastasis. As indicated in Table 2, we found a positive correlation between the expressions of HCCR-1 mRNA and protein and histologic grade, clinical staging, and lymph node metastasis (all p<0.001). Most striking, there was a higher incidence of lymph node metastasis with 100% positive expressions of HCCR-1 mRNA and protein compared to those without lymph node metastasis (100% vs 53.85%, 100% vs 58.97%, respectively), suggesting the expressions of HCCR-1 mRNA and protein play critical roles in malignant transformation of ESCC. Conversely, no significant correlation was found between the expressions of HCCR-1 mRNA and protein and gender (p=0.668 and 0.138, respectively) and age (p=0.248 and 0.408, respectively).
Association of HCCR-1 mRNA and Protein Expressions in ESCC Patients with Various Clinicopathological Features
Real-Time Quantitative RT-PCR Analysis for HCCR-1 mRNA Expression in ESCC Tissues
The relative levels of HCCR-1 mRNA were investigated in six randomly selected cases of ESCC and paired normal esophageal epithelial tissues by real-time qRT-PCR method. The results demonstrated that the relative level of HCCR-1 mRNA was significantly elevated to varying degrees in a panel of ESCC tissues compared with paired normal esophageal epithelial tissues (all p<0.05) (Fig. 3). Upregulation was greatest in sample 6 (88.50-fold), intermediate in samples 4 and 5 (10.53- and 12.82-fold, respectively), and moderate in samples 1, 2, and 3 (2.50-, 6.06-, and 2.87-fold) compared with paired normal esophageal epithelial tissues. These data presented herein indicate that HCCR-1 at high levels in ESCC tissues may play a pivotal role in the development and progression of ESCC.
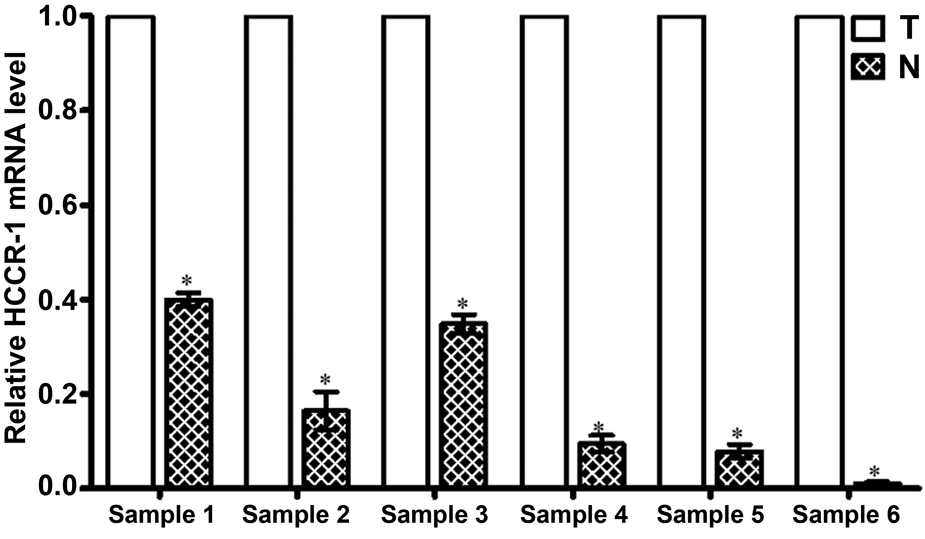
Relative levels of HCCR-1 mRNA in six representative cases of ESCC tissues (T) and paired normal esophageal tissues (N). The total RNA was isolated in different randomly selected samples, and then subjected to reverse transcription to obtain the first cDNA strand. Subsequently, real-time quantitative RT-PCR based on SYBR green dye was carried out to obtain the Ct value of various samples on an ABI 7300 PCR instrument. Relative levels of HCCR-1 mRNA in various samples were counted by the formula 2-DDCt, the results were analyzed by SPSS 13.0 software, are expressed as means ±SD. *P<0.05, compared to relative levels of HCCR-1 mRNA in ESCC tissues.
Western Blotting Detection of HCCR-1 Protein Expression in ESCC Tissues
HCCR-1 protein levels were determined in six randomly selected cases of ESCC samples and paired normal esophageal epithelial tissues by Western blotting. The results revealed that the relative level of HCCR-1 protein in various ESCC samples was markedly higher than that in corresponding normal esophageal epithelial tissues (all p<0.05) (Fig. 4A, 4B). Of all six cases of samples selected, the relative expression of HCCR-1 protein in samples 6 and 1 reached the highest level and lowest level, as compared with the other different samples, respectively (Fig. 4A, 4B) and about 99.5- and 2.7-fold of normal esophageal epithelial samples, respectively. The data suggest that overexpression of HCCR-1 protein may be tightly associated with the development and progression of ESCC.
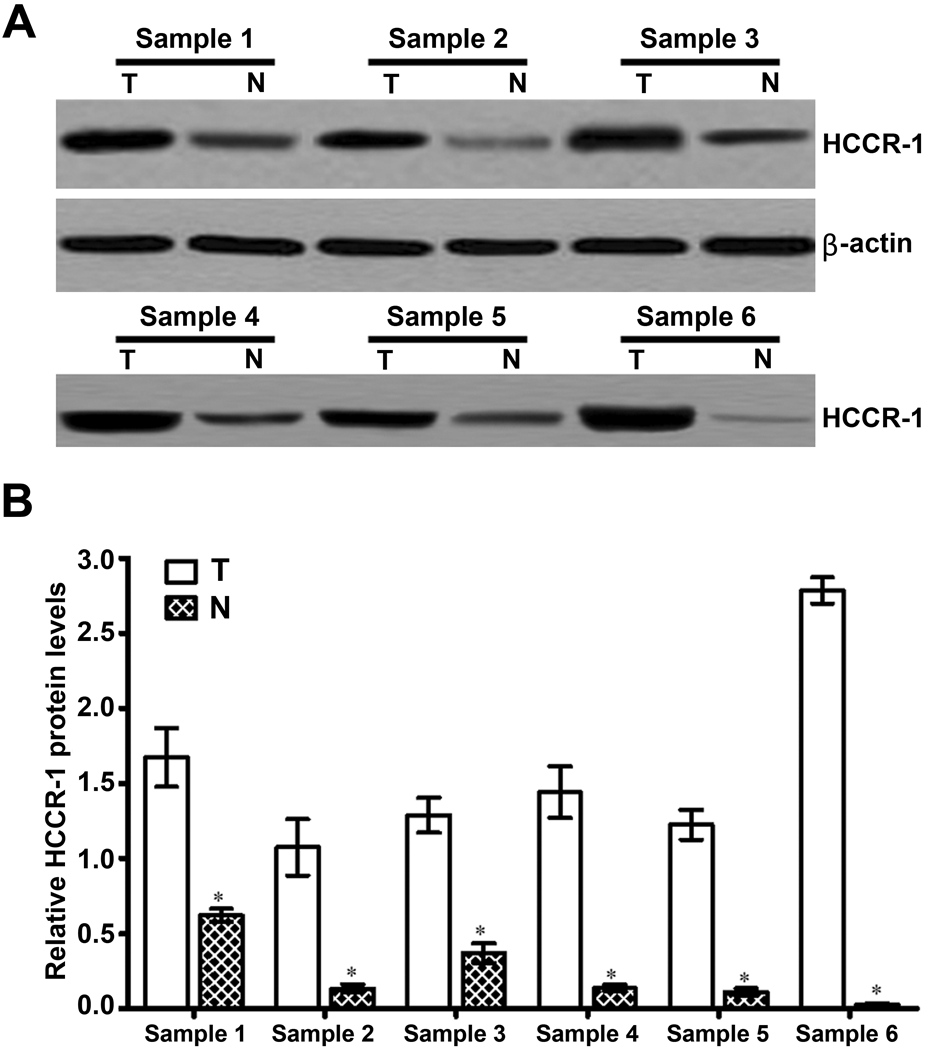
Relative levels of HCCR-1 protein in six representative cases of ESCC tissues (T) and paired normal esophageal tissues (N). The total proteins were extracted in randomly 6 cases of ESCC tissues and paired normal esophageal epithelium tissues. Potein concentrations were determined with standard Bradford method. An equal amount of tissues lysates were electrophoresed through a 10% SDS-PAGE gel, and then transferred to nitrocellulose membranes. Subsequently, HCCR-1 and β-actin antibodies were applied to membrane and DAB was used to develop the specific proteins on the membranes. A: The expression level of HCCR-1 protein was analyzed by Western blotting. Expression of β-actin was simultaneously used as an internal control. B: Semi-quantitative values of three independently repeated Western blotting were statistically analyzed by densitometry using Image-Pro Plus 5.0 software, are expressed as means ±SD. *P<0.05, compared to levels of HCCR-1 protein in ESCC tissues.
HCCR-1 at High Level Predicts Poor Prognosis for Patients with ESCC
The relationships between levels of HCCR-1 mRNA and protein and survival time of the patients with ESCC were evaluated by Kaplan-Meier survival curve. The mean follow-up period of all the patients with ESCC in this study was 43 months (range, 1 to 60 months). During the follow-up period, 77 of the 113 HCCR-1 protein–positive ESCC patients (68.14%) and 72 of the 104 HCCR-1 mRNA–positive ESCC patients (69.23%) had died, whereas 15 of the 45 HCCR-1 protein–negative or HCCR-1 protein–weak positive ESCC patients (33.33%) and 17 of the 54 HCCR-1 mRNA–negative or HCCR-1 mRNA–weak positive ESCC patients (31.48%) had died. As determined by the log-rank test (Mantel-Cox), the survival rate of patients with low-level HCCR-1 staining was higher than those patients with high-level HCCR-1 staining, whether it was mRNA or protein (both p<0.05) (Fig. 5A, 5B), suggesting that HCCR-1 may be used as a novel predictor for the prognosis of the patients with ESCC.
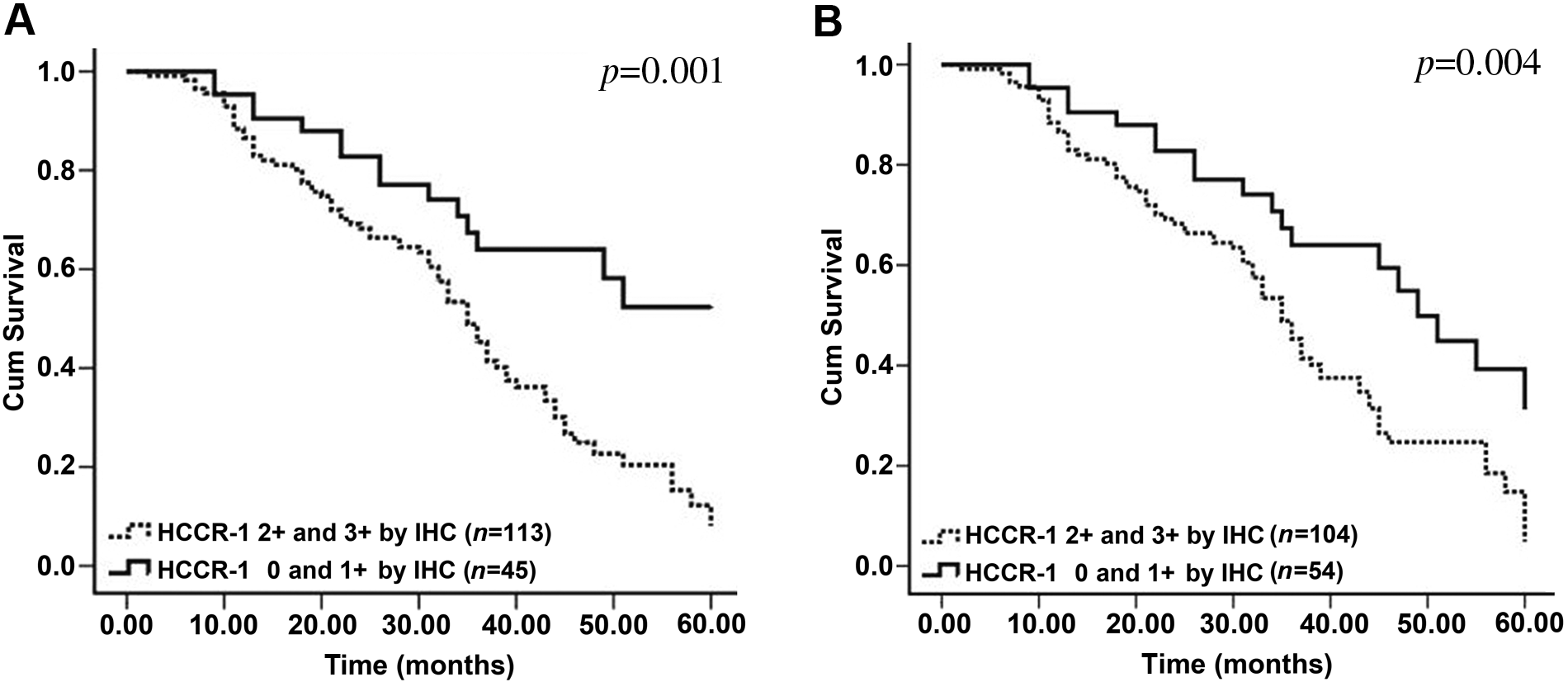
The relationship between the relative level of HCCR mRNA and protein and the prognosis of the patients with ESCC. A: IHC analysis for the association between HCCR-1 protein level and survival time of the patients with ESCC. B: ISH analysis for the relationship between HCCR-1 protein level and survival time of the patients with ESCC. There was a significant difference between the two curves by log-rank test (Mantel-Cox) (P<0.01).
Multivariate Analysis
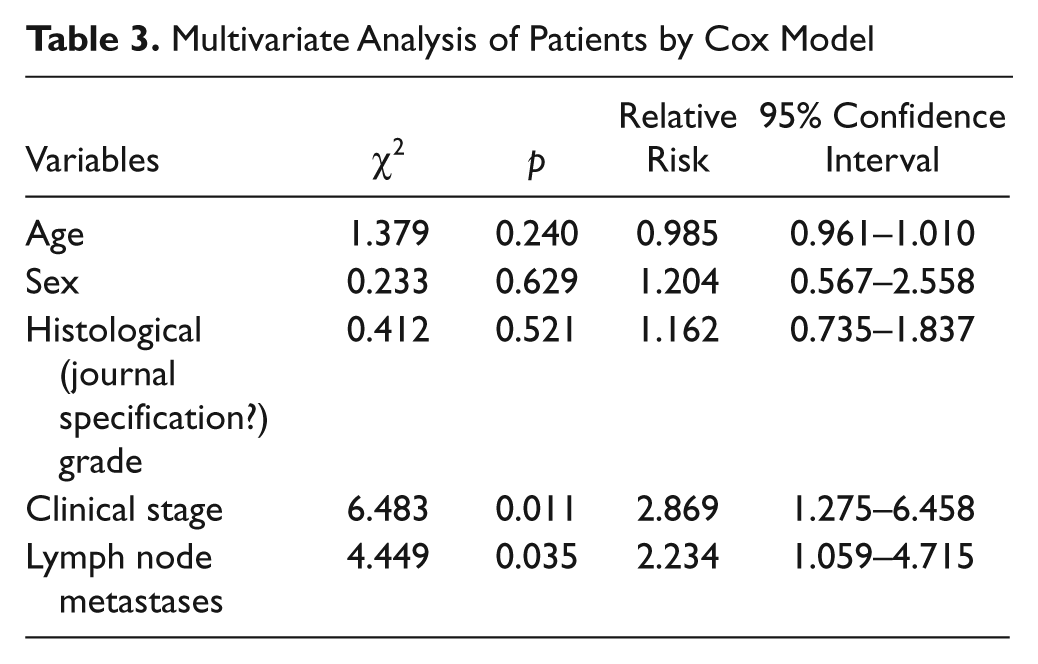
Multivariate survival analysis, including all significant prognostic factors mentioned in univariate analysis, was performed to determine the independent prognostic factors for ESCC. Multivariate analysis using Cox proportional hazards model showed that clinical stage and lymph node metastases were independent prognostic factors of ESCC (Table 3).
Multivariate Analysis of Patients by Cox Model
Discussion
The accumulated knowledge has demonstrated that elevation of HCCR-1 expression is involved in tumor development and progression in a variety of malignant tumors (Ko et al. 2003; Ko et al. 2004; Shin et al. 2006; Jung et al. 2005; Yoon et al. 2004). Recent investigations have revealed that HCCR-1 is expressed at a high level in a large proportion of hepatocellular carcinoma (HCC) but is undetectable in normal hepatocytes and nonmalignant liver disease (Yoon et al. 2004; Xia et al. 2006; Zhou et al. 2006; Yang et al. 2007). Additionally, Yoon et al. (2004) found that HCCR-1 mRNA and protein were overexpressed in tumor tissues compared with nontumorous cirrhotic tissue of HCC, and an elevated level of HCCR-1 has been verified to be closely associated with an increase in the risk of developing HCC. Stepwise investigations revealed that HCCR-1 also exerted an oncogenic activity in the breast and colon cancers (Ko et al. 2004; Shin et al. 2006). Interestingly, the upregulation of HCCR-1 found in most of pancreatic cancers was triggered by EGF signaling, which has been already known to regulate the development of pancreatic cancer (Xu et al. 2010). Given these findings, we put forward the question as to whether HCCR-1 is expressed at high levels in ESCC tissues. Therefore, in the current study, we evaluated the expression levels of HCCR-1 mRNA and protein in ESCC tissues by ISH and IHC methods. We found that the expression of HCCR-1 mRNA in ESCC tissues was significantly higher than that in squamous dysplasia tissues and normal esophageal epithelial tissues (p<0.001). Further investigation showed that the positive rates of HCCR-1 protein in ESCC, squamous dysplasia tissues, and normal esophageal epithelial tissue were 79.75%, 40.95%, and 3.80%, respectively. Compared with that of squamous dysplasia tissues and normal esophageal epithelial tissues, there was obvious increase in HCCR-1 protein level in ESCC tissues (p<0.001). Additionally, we randomly selected six cases of ESCC tissues and paired normal esophageal epithelial tissues to detect the expressions of HCCR-1 mRNA and protein by real-time qRT-PCR and Western blotting methods, and the results showed that overexpression of HCCR-1 appeared in ESCC tissues compared with normal esophageal epithelial tissues. The present data herein suggest that overexpression of HCCR-1 plays a critical role in the progression of ESCC.
It is well-documented that clinicopathological parameters, including histological grade, clinical staging, and the status of lymph node metastasis, are the most critical prognostic factors for determining clinical outcomes in esophageal cancer (Roder et al. 1995). To date, few studies have been available that examine the relationship between HCCR-1 expression and clinicopathological features of ESCC. Here, to elucidate the potential role of the HCCR-1 expression in the development and progression of ESCC, we investigated the relationship of expressions of HCCR-1 mRNA and protein and clinicopathological features of ESCC. We found a positive correlation between the expressions of HCCR-1 mRNA and protein and histological grade, clinical staging, and lymph node metastasis (all p<0.001). The patients with ESCC in poorly differentiated status appeared with higher levels of HCCR-1 mRNA and protein. Most important, there were 100% positive expressions for both HCCR-1 mRNA and protein in ESCC tissues in lymph node metastasis groups, suggesting that HCCR-1 might serve as molecular predictor for tumor metastasis and play an essential role in malignant transformation of ESCC; however, further analysis for this event remains under investigation.
The prognosis for patients with ESCC is dismal in recent years, despite attempts at aggressive multimodality treatments (Hofstetter et al. 2002; Urschel et al. 2002). Ha, Lee, et al. (2009) found that overexpression of HCCR-1 was well correlated with known breast cancer prognostic markers, including the presence of steroid receptors (ER and PR), p53 mutation, and high HER2 overexpression, thereby indicating that HCCR-1 may serve as a novel predictor for different malignant tumors. Currently, there are few ideal prognostic markers to investigate the prognosis of the patients with ESCC, to further explore whether there is a relationship between the expressions of HCCR-1 mRNA and protein and prognosis of the patients with ESCC. Kaplan-Meier curve was utilized to analyze the expressions of HCCR-1 mRNA and protein and prognosis of the patients with ESCC using the log-rank test (Mantel-Cox); as such, we found that the patients of ESCC with high levels of HCCR-1 mRNA and protein had a poorer prognosis than those with low levels of HCCR-1 mRNA and proteins, and there was a significant difference between HCCR-1 expression and survival time for patients with ESCC (both p<0.05), suggesting that HCCR-1 may be used as a novel predictor for the prognosis of patients with ESCC. Most important, multivariate analysis using Cox proportional hazards model showed that clinical stage and lymph node metastases were independent prognostic factors of ESCC.
In conclusion, HCCR-1 displays a substantial function in promoting ESCC carcinogenesis and tumor progression. It is concluded that the detection of HCCR-1 expression might serve as a clinical marker in the diagnosis or prediction of clinical outcomes for patients with ESCC. Meanwhile, these data also provide for future prospects for a therapy for ESCC based on the inhibition of HCCR-1 expression, although many details remain to be elucidated.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.