
Abstract
Hypoxic/ischemic encephalopathy in a cloned American Quarter horse foal was initially associated with placental insufficiency and exacerbated by protracted hypotension during anesthesia for a surgical procedure. The foal, born at the Texas A&M Veterinary Medical Center, was diagnosed at birth with neonatal maladjustment syndrome that was accompanied by dysmaturity, muscle contracture of the front limbs, and a blood clot within the lumen of the urinary bladder. Seizures that developed after anesthesia were attributed to hypoxia/ischemia during anesthesia and culminated in death. Macroscopically, the cerebrum had flattened cerebral gyri with shallow sulci, yellowish cortical discoloration, and apple-green autofluorescence (under 365-nm ultraviolet light) at the cortical/white matter junction. Microscopically, there was laminar cortical necrosis with prominent diffuse ischemic change of neuronal cell bodies. The white matter had prominent rarefaction with focal axonal and myelin degeneration and focal macrophage (gitter cell) accumulation. Additionally, there was astrocytic hypertrophy with gemistocyte formation. The chorioallantois was diffusely thickened in the area corresponding to the uterine horns. Histologically, microcotyledons were markedly attenuated with absence of chorionic villi.
Hypoxic/ischemic encephalopathy (HIE) developed in a cloned, newborn American Quarter horse foal and was exacerbated by anesthesia. The lesions that resulted exemplify the problems that can occur after attempted surgical intervention in foals with neonatal maladjustment syndrome (NMS).
A pregnant mare from a research colony at Texas A&M University was transferred to the Texas Veterinary Medical Center to undergo supervised delivery of an American Quarter horse foal cloned from fibroblasts of a gelding. The mare foaled at a normal gestation of 352 days and the delivery was uneventful and minimally assisted. The placenta was collected immediately and submitted for gross and histologic evaluation. The 45-kg male foal was born weak with no suckle reflex, and was suspected to have NMS. An arterial blood gas and serum biochemistry panel performed shortly after birth revealed a moderately decreased P
At necropsy, the brain had congested meninges and flattened cerebral gyri and shallow sulci resulting from edema (Fig. 1). On cross section, the gyri were swollen with a poorly demarcated cerebral gray matter–white matter interface. A focally extensive yellowing of the cortex also involved the subcortical white matter, putamen, and globus pallidus. Discolored cerebral tissue autofluoresced apple-green under 365-nm ultraviolet light (Fig. 1 inset), as described in the cerebrum of cattle with polioencephalomalacia. 13
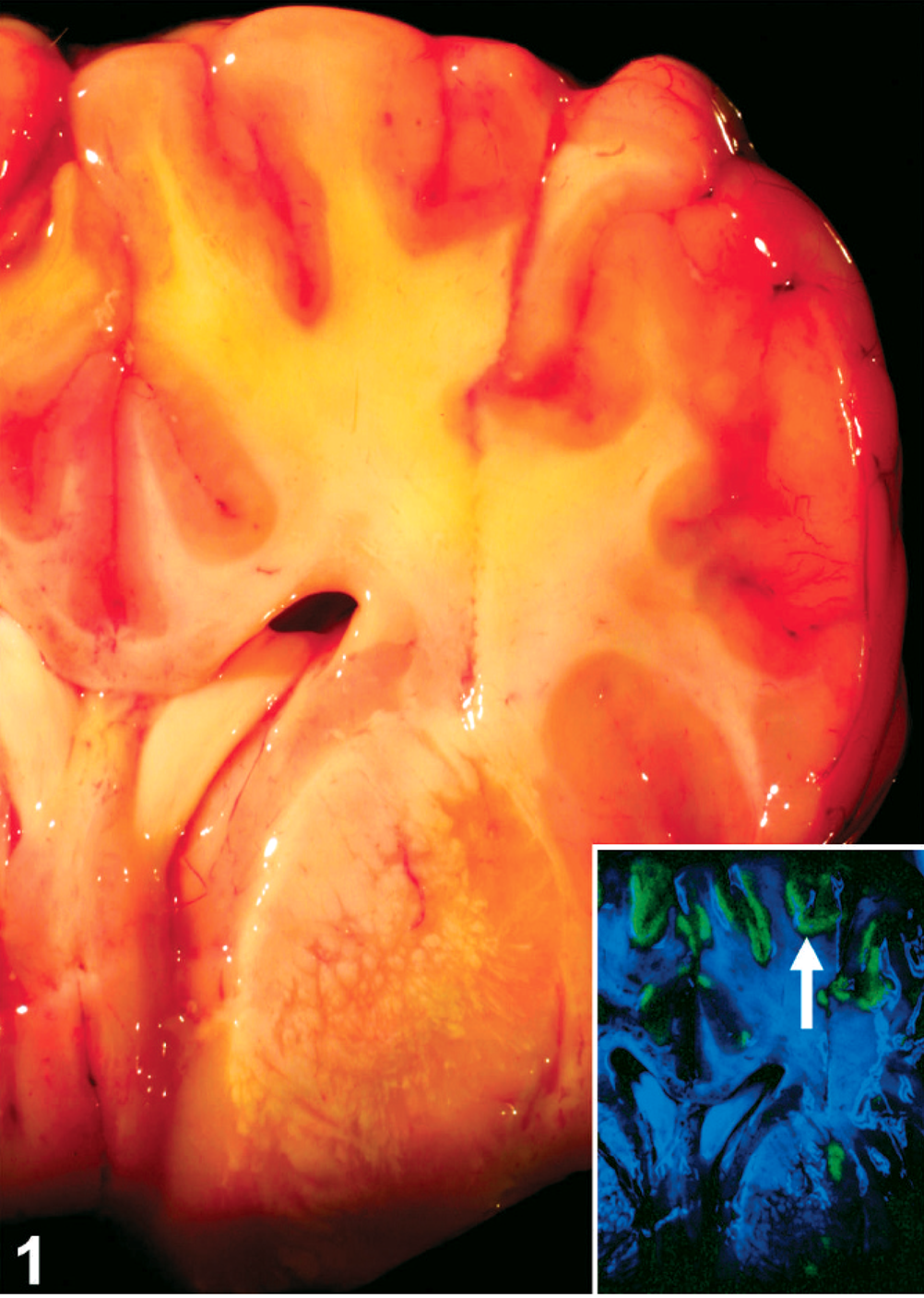
Brain, cross-section, level of basal nuclei; neonatal foal. Swelling of cerebral gyri, compression of sulci, and focal yellowing of the cortex that also involves the subcortical white matter and basal nuclei. Inset: Brain, cross-section, through basal nuclei. Linear strands of apple-green autofluorescence of the dorsal cortex (arrow). Ultraviolet illumination of fresh specimen, 365 nm.
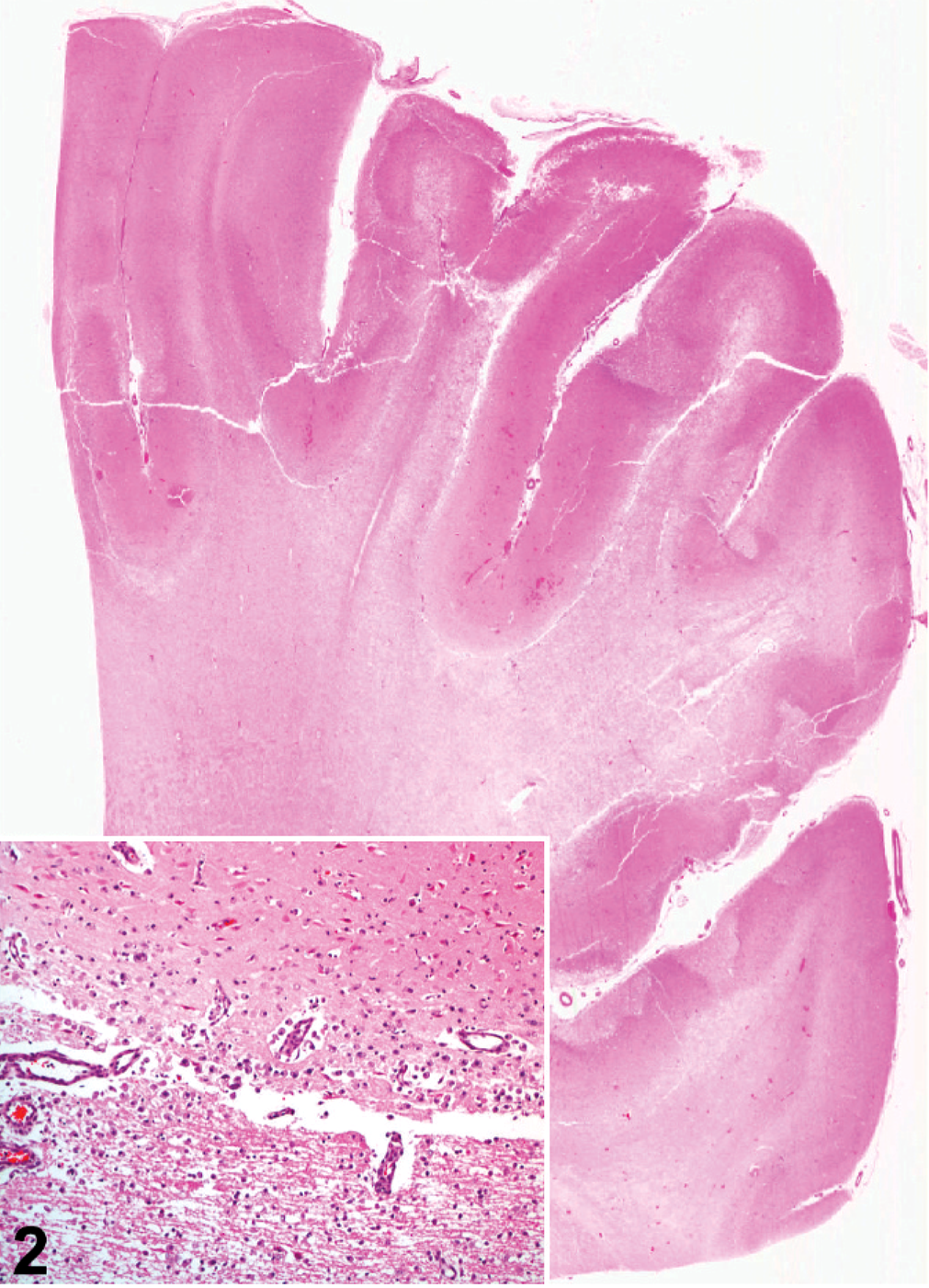
Cerebrum; neonatal foal. Prominent edematous rarefaction of white matter and cortical necrosis illustrated by the darker staining, especially of the dorsolateral cortex. HE. Inset: Higher magnification of laminar cortical necrosis also involving the gray matter (top)–white matter (bottom) interface with macrophage accumulation. HE.
The area of the chorioallantois corresponding to the uterine horns was diffusely thickened and gray-brown, with cobblestone texture. The urinary bladder mucosa was multifocally dark red with irregular borders and contained a 6-cm × 7-cm blood clot; however, the bladder wall was intact. The urachus and junction of the umbilical remnant were expanded to twice normal size and hemorrhagic. Muscle contracture was confirmed by an inability to fully extend the front limbs.
Sections of the brain, placenta, and umbilicus were immersed in 10% formalin and processed for microscopic and immunohistochemical examination. In addition to hematoxylin and eosin staining, serial sections (5–20 μm) of the cerebrum were stained with Luxol fast blue for myelin and impregnated with Holmes' silver nitrate for axons. Sections (5 μm) of the cerebrum were also processed with the streptavidin-biotin-immunoperoxidase method using a 1:1,000 dilution of the primary antibody glial fibrillary acidic protein (GFAP) (Dako; rabbit polyclonal). Normal equine brain tissue was used as the positive control and the primary antibodies were excluded for the negative control.
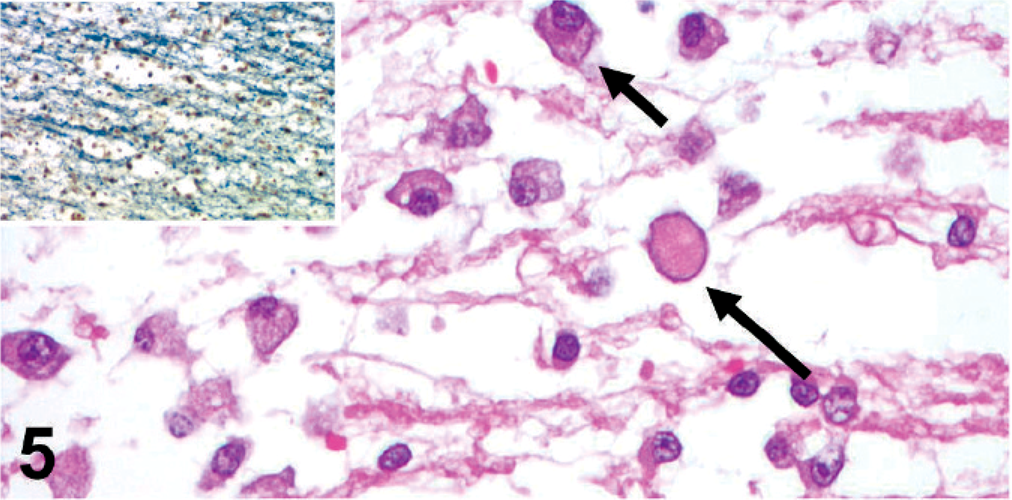
Microscopically, the cerebral cortex had prominent ischemic neuronal change, with shrunken, hypereosinophilic, angulated perikaryon and pyknosis of neuronal cell bodies (Fig. 3). The cerebral gray matter–white matter interface was disrupted by nonproteinaceous edematous rarefaction that extended into the adjacent white matter where myelinated axons (confirmed by Luxol fast blue staining and silver impregnation) were prominently separated. Within the affected white matter were focal axonal and myelin degeneration, modest clusters of macrophages (gitter cells), prominent endothelial reactive hypertrophy and hyperplasia, congestion, and prominent gemistocytic astrocytes that were often paired, indicating postmitotic division (astrocytosis). Additionally, there were frequent mitotic figures, some of which were considered to represent astrocytes (Fig. 4 and inset).
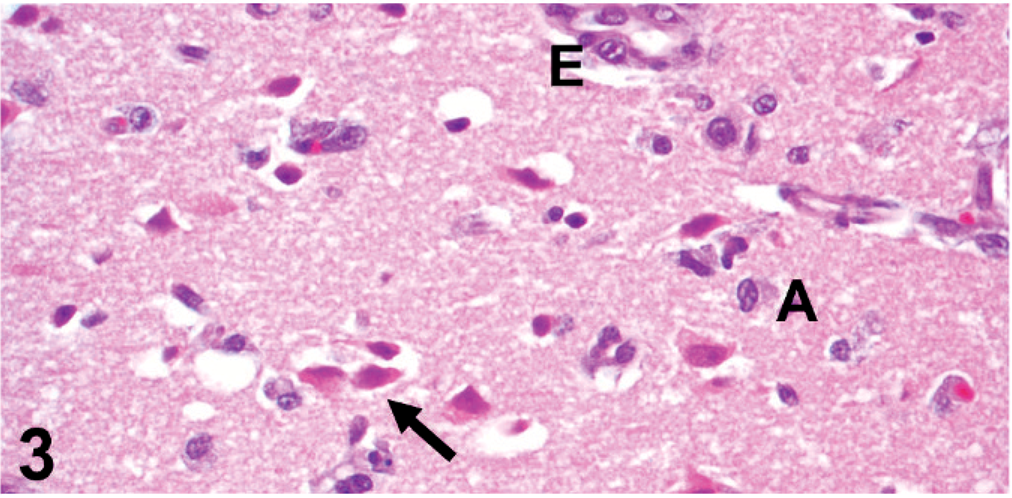
Cerebrum; neonatal foal. Ischemic neuronal change. Hypereosinophilic neuronal cell bodies with shrunken, angulated perikaryon (arrow). Note also prominent endothelial hypertrophy (E) and few gemistocytic astrocytes (A). HE.
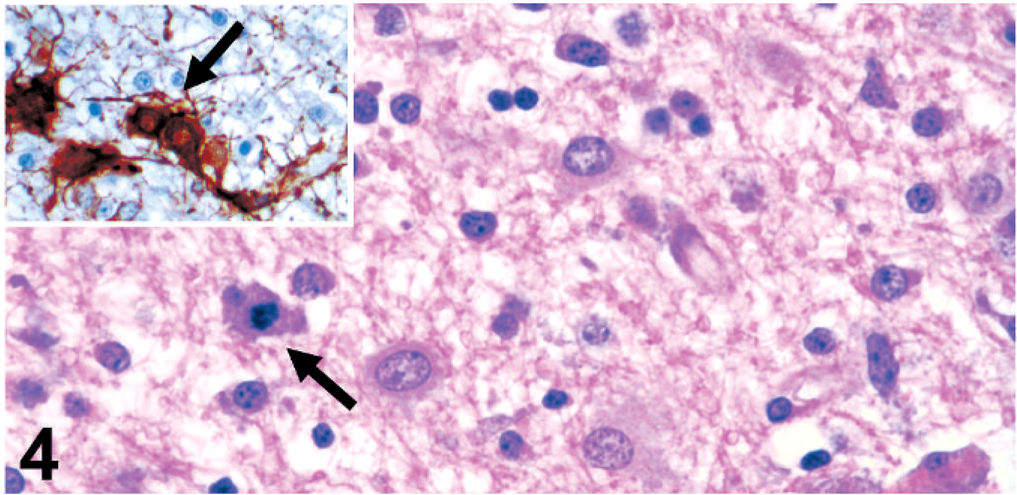
Cerebrum; neonatal foal. Gemistocytic astrocytes and mitotic figure in a presumed astrocyte (arrow). HE. Inset: Hypertrophied astrocytes with strong immunohistochemical reactivity for glial fibrillary acidic protein (GFAP). Note paired reactive astrocytes indicating recent cell division (arrow). GFAP immunohistochemistry.
The microcotyledons of the uterine horn chorioallantois were devoid of long villi and instead, composed of moderately rugose, thickened chorion. This was lined by columnar to cuboidal, simple to pseudostratified, microvesiculated trophoblastic epithelium supported by mildly hyalinized collagen containing keratin fragments and mineral deposits (Fig. 6). The subchorionic epithelial stroma was prominent with abundant neovascularization contributing to its thickness, and minimal perivascular to diffuse neutrophilic inflammation.
Cerebrum; neonatal foal. Edematous rarefaction of white matter, with scattered gitter cells presumably containing myelin debris (short arrow) and axonal spheroids (long arrow). HE. Inset: Cerebrum, edematous separation of myelinated axons in the white matter. Luxol fast blue.
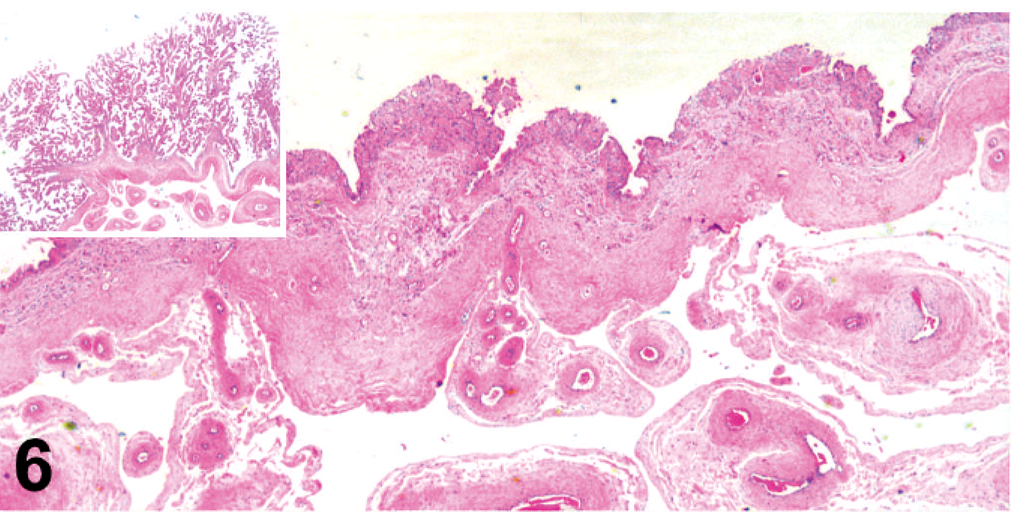
Placenta; uterine horn chorioallantois of neonatal foal. Note the marked attenuation of microcotyledonary chorionic villi and thickening of the placental membrane with prominent subchorionic stroma and neovascularization. HE. Inset: Normal placenta, uterine body chorioallantois. Normal diffuse placentation with prominent, long microcotyledonary chorionic villi. HE.
The urinary bladder was unremarkable with the exception of multifocally extensive areas of mucosal congestion and hemorrhage. The umbilical venous endothelium was ulcerated and replaced by a coagulum of erythrocytes, fibrin, and degenerate neutrophilic debris. The umbilical wall was thickened and disrupted by severe transmural fibrinosuppurative inflammation, granulation tissue, hemorrhage, edema, and fibrin thrombi. There was lymphoid depletion with hyalinosis in splenic corpuscles, suggestive of endogenous corticosteroid release or sepsis. Septicemia could not be determined with bacteriologic examination of the spleen due to concurrent antibiotic administration. No significant lesions were identified in other tissues examined.
Neonatal maladjustment syndrome is a disorder in which affected newborn foals display behavioral or neurologic abnormalities unrelated to the presence of infectious agents, toxicities, or metabolic disorders. 6 Also known as barkers, wanderers, and dummies, these foals exhibit central nervous system signs within the first few days of life and appear to suffer from cerebral hypoxia.
This syndrome has been proposed to result from deficient blood flow (ischemia) or decreased arterial oxygen tension (hypoxemia) leading to HIE. Proposed causes include fetal malformation, meconium aspiration, placental abnormalities (e.g., placental insufficiency, premature placental separation), dystocia, and maternal complications (e.g., illness, malnutrition). 5 In foals suffering from NMS and HIE, neurologic signs, such as stupor, seizures, motor dysfunction, and oculomotor disturbances, as well as abnormal or absent sucking and swallowing, have been reported. 4
Lesions of NMS have been described to involve the nervous, urinary, respiratory, endocrine, and gastrointestinal systems. 5, 12 The most severe lesions involve the central nervous system due to adverse effects on energy metabolism in the brain. The concentration of lactate rapidly increases as glucose is metabolized via anaerobic respiration due to limited oxygen availability. Free radicals are produced during hypoxic/ischemic episodes leading to peroxidation of membrane phospholipids and disruption of cellular integrity. 5, 6 Excitotoxicity may have contributed to neuronal cell death mediated by the excitatory neurotransmitter glutamate, which is produced during hypoxic/ischemic episodes. 12
A previous study found that up to 40% of foals suffering from NMS had septicemia.
3
Severe omphalophlebitis was confirmed in this case; however, septicemia could not be verified, presumably due to concurrent antibiotic administration. Although this foal was born at full-term, it had evidence of dysmaturity (incomplete ossification of the cuboidal bones, muscle contractures, weakness, and reduced suckle reflex). Dysmaturity is used to describe foals born at full-term with changes typical of prematurity, and is often associated with placental abnormalities.
10
In this case, placental insufficiency resulted from markedly attenuated microcotyledons with absence of chorionic villi and presumably contributed to the systemic hypoxia with decreased P
This case is noteworthy for the deterioration that occurred after anesthesia of the foal. During the first 3 days after birth, the foal could stand unassisted and was bright and alert. Serum biochemistry results improved, except for developing hematuria and azotemia. After anesthesia for bladder exploration, seizures and abnormal vocalization occurred, and the foal remained recumbent and unresponsive until death. Despite the development of azotemia, the foal might have survived the initial HIE if surgical exploration had not been necessary. In a study of 78 foals with NMS, 78% recovered after hospitalization and supportive care. 2 In another study, foals that developed sepsis, failed to improve neurologically within the first 5 days after birth and remained comatose, had the poorest prognosis. 3
Dysmature and premature foals that experience prolonged hypoxia in utero, which probably occurred in this case, are more prone to develop intractable hypotension and persistent seizure activity. 2 The severity of edema within deep cerebral white matter in this foal is unusual for uncomplicated cases of NMS. 11 However, its presence may have been due to the additive hypoxia that developed during anesthesia, which possibly exacerbated ischemic cytotoxic and vasogenic edema. Fluid therapy was considered an unlikely contributor to cerebral edema in this foal because hypertonic saline was used. Anesthesia-related cerebrocortical necrosis with subcortical edema and marked astrocytic response has been attributed to hypoxia/ischemia in animals. 11 The proposed causes include an anesthetic accident or cardiac arrest. In the present foal there was no evidence of cardiac arrest or other cardiac problems during the period of anesthesia.
The cloning of horses, using nuclear transfer embryos from adult or fetal donor cells, is a recent event with the first successful cloned foals reported in 2003. Pregnancy rates after transfer of equine-cloned embryos vary from 9% to more than 60%, with approximately 50% or greater of established pregnancies reaching full term. 7 Similar pregnancy rates of 73% and 62–69% have been reported for artificial insemination and natural matings, respectively. 1, 8, 9 By 2006, 16 viable cloned foals had been reported, 13 of which developed normally. 7 Three of these foals died, one each from septicemia, pneumonia, and anesthetic complications (the present case). Eleven of these 16 cloned foals were produced at the Texas A&M Veterinary Medical Center, 9 of which survived. With a survival rate of 13 of 16, it is unknown what influences cloning may have had on the developing fetus in this case. A much larger population of cloned foals is needed to elucidate the potential health effects that may be related to the cloning process.
Footnotes
Acknowledgements
We thank John Roths for his invaluable assistance with photographic images and Rosemary Vollmar, Sarah Jones, and Dr. Andy Ambrus for preparation of sections for microscopic and immunohistochemical examination.