
Abstract
A recently described metaphyseal irregularity of the radius and ulna was diagnosed radiographically in a significant proportion of Newfoundland dogs during the course of a large study. This case report describes the pathological picture of a Newfoundland dog with these radiographic changes. The lesions in the distal radius and ulna were characterized by focal, longitudinal striations of sclerosis of the bone marrow cavity, surrounding thin trabeculae of primary spongiosa of the distal metaphysis. It is suggested that these lesions represent a sclerosing dysplasia not previously described in dogs, but with some similarities to the human disorder, osteopathia striata.
Developmental orthopedic diseases like metaphyseal osteopathy, enostosis, osteochondrosis, hip and elbow dysplasia, and pes varus are conditions of young dogs that may cause considerable problems for both the dogs and their owners with respect to the clinical condition, animal welfare considerations, and financial outlay. In order to achieve a high level of diagnostic accuracy thorough scientific descriptions of the normal development of the affected tissues, the various manifestations of these diseases and their differential diagnoses are important.
A large-scale, longitudinal, observational study was conducted to study skeletal lesions in growing dogs with regard to nutrition, growth rate, and environmental factors. 7 The study included 4 large breeds of dog: Newfoundland, Labrador Retriever, Leonberger, and Irish Wolfhound. Seven hundred privately owned dogs, derived from 107 different litters, were initially enrolled in the study, with the housing and feeding regimen of each participating dog decided by its owner. During the study, previously undescribed radiographic irregularities in the distal radial and ulnar metaphysis were discovered and described in 54 of the 118 Newfoundlands (NFs) participating in the study. 8 The dogs with irregularities did not show any obvious clinical signs, and their development did not seem be impaired. However, the importance of these findings lies in their potential to be misinterpreted as metaphyseal osteopathy (hypertrophic osteodystrophy), osteodystrophy caused by malnutrition, enostosis (panosteitis), or other diseases affecting cancellous bone in growing animals, and thereby likely to cause unnecessary concern and costs for the owner, considerable diagnostic work for the veterinarian, and, in the worst case, erroneous euthanasia.
This report describes the clinical and pathologic findings from one of the NFs with the metaphyseal irregularities described. Based on these findings, it is proposed that the lesion represents a type of sclerosing bone dysplasia.
One of the dogs with metaphyseal irregularities, and which had participated in the study described, was euthanatized and submitted for necropsy. At 4 months of age, routine radiography had revealed irregular remodeling in the distal ulna. At 6 months of age, metaphyseal irregularities of grade II had been observed in both radius and ulna (Table 1). The irregularities were most pronounced in the ulna, where they reached from the distal metaphysis to the middle of the diaphysis, with distinct opaque islands of trabeculae. At 12 months of age, focal cortical irregularities with poorly defined margins were present. The cortical irregularities in the ulna were “cystlike” in appearance, with reduced radiographic opacity in the center of the “cyst.” The irregular changes seen in the metaphysis at 6 months were in regression in both radius and ulna at 12 months.
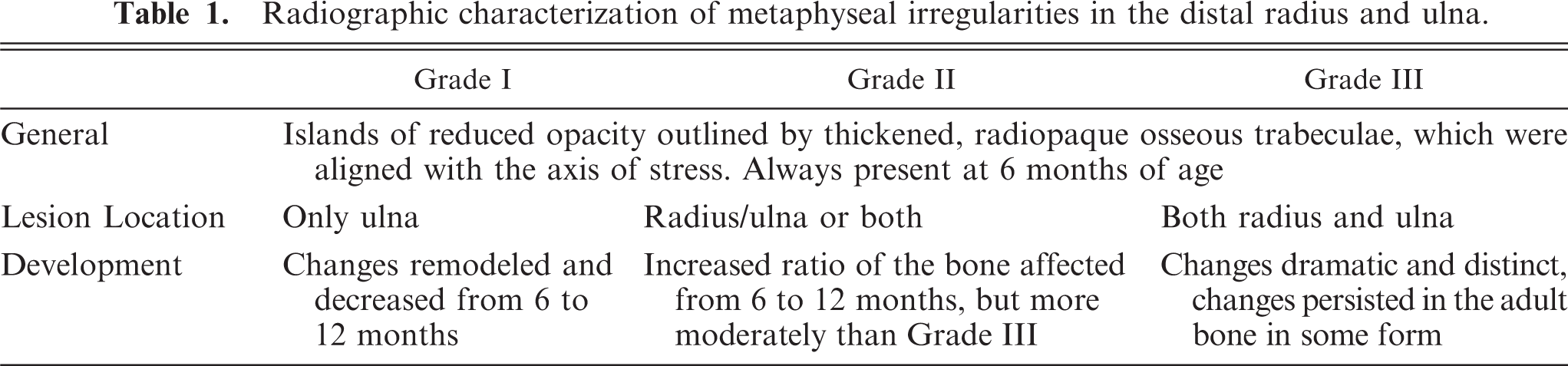
Radiographic characterization of metaphyseal irregularities in the distal radius and ulna.
At presentation, at 13 months of age, the dog was in normal body condition. The dog was standing in an underposition with its hind limbs, was lame in both hind limbs, and had bilateral thickening of the knees. The radiographic diagnosis was severe bilateral gonitis with subluxation of patellae. Due to the poor prognosis, the owner decided the dog should be euthanatized.
The previously diagnosed metaphyseal irregularities were described at the necropsy, and the diagnosis of bilateral subluxation of patellae and severe osteoarthritis was confirmed. In the bone marrow of the diaphysis of the distal radius and ulna, several linear, longitudinal striations between 1 to 4 cm long, of solid, relatively homogenous tissue, focally displaced the normal cancellous bone (Fig. 1). Histologic examination revealed that the tissue consisted of loosely packed, sparsely cellular fibrous tissue infiltrating between, and blending with, surrounding bone trabeculae (Figs. 2, 3). The bone trabeculae were relatively thin and delicate compared with the surrounding areas of cancellous bone. They consisted mainly of woven bone, sometimes with central areas of mineralized cartilage (Fig. 4), compared with the surrounding trabeculae and cortex made from lamellar bone. There were few to moderate numbers of osteoclasts on their surfaces. The cortex adjacent to the striations was unevenly thickened. On the outer surface, numerous active osteoclasts formed multiple depressions in the lamellar bone. In the overlying inner layer of the periost, mild edema and proliferation of osteoprogenitor cells were evident. In some areas, the loosely packed fibrous tissue of the striations blended with the inner layer of the periost through gaps in the cortex. The physeal growth plates were narrow and not continuous throughout the whole width of the bone, i.e., close to cessation of longitudinal growth but were otherwise apparently normal.
To the authors' knowledge this is the first report of clinical and pathologic findings in a dog with the described radiographic irregularities in the metaphysis. Such metaphyseal irregularities were discovered and described in NFs during a larger study. 8 Radiographically, the irregularities were characterized by distinct opaque islands of trabeculae in the metaphyses and distal diaphyses of the radius and ulna. Pathologically, they were characterized by focal, longitudinal striations of sclerosis of the bone marrow cavity, surrounding thin trabeculae of primary spongiosa. In comparison, metaphyseal osteopathy (hypertrophic osteodystrophy) is characterized radiographically by alternating radiodense and radiolucent zones parallel to the growth plate and characterized histologically by inflammatory changes, with hemorrhages and massive infiltrates of neutrophils and lymphocytes within the metaphyseal bone marrow and necrosis of trabecular bone. 4, 6 Enostosis (panosteitis), however, is characterized by focally increased radiodensity in the medulla around the nutrient foramen, while histologically, this disorder is characterized by increased osteoblastic and fibroblastic activity, medullary fibrosis, and formation of bone by fibrous metaplasia, creating islands of woven bone within the spongiosa. 1, 2, 6 Consequently, the lesions described in the present case resemble neither metaphyseal osteopathia nor enostosis, nor malnutritional skeletal changes, but represent a “new” entity in dogs.
In human medicine, the term “sclerosing bone dysplasias” is used for a wide range of developmental anomalies discernible by distinct radiodense radiographic findings. Based on a target-site approach, originally proposed by Greenspan 3 and later modified in International Nomenclature and Classification of the Osteochondrodysplasias (2001) 5 by Vigorita 10 and by Vanhoenacker, 9 the conditions are classified into 3 groups: dysplasias of endochondral bone formation, dysplasias of intramembranous bone formation, and mixed sclerosing dysplasias. Within these groups, further differentiation can be made by clinical findings and by mode of inheritance. 9 Osteopathia striata, or Voorhoeve disease, is an asymptomatic autosomal–dominant or sporadic inherited disorder, characterized by radiodense striations in the meta- and diaphysis of predilection sites, typically locations where growth is rapid. 9 The striations are oriented parallel to the long axes of the bones and appear to be linked to the predominant pattern of the longitudinal columns of bone trabeculae of the developing secondary spongiosa. This suggests that they are the result of aberrant, or incomplete, conversion of primary spongiosa into mature secondary spongiosa. 10
In our opinion, our findings from the dog in this case bear many similarities to the descriptions of the isolated form of the human asymptomatic sclerosing bone dysplasia, designated osteopathia striata. As suggested for this disorder, 10 the radiographic and histopathologic findings in this canine case also suggest a pathogenesis involving focal failure in the conversion from primary to secondary spongiosa. The observed sclerosis of the bone marrow might be considered an attempt at mechanical stabilization of the fragile primary spongiosa, rather than being an integral part of the primary spongiosa. The etiology, however, remains obscure.
The metaphyseal irregularities described were evident in 54 of 118 dogs (45.8%). 8 The significance of these findings lies in their potential for misinterpretation, especially if they are discovered in the presence of clinical signs, such as lameness or growth arrest. The high incidence of this condition in this group of dogs emphasizes the importance of accruing knowledge on the associated radiographic and pathologic findings in order to be able to differentiate these findings from others, which are of pathologic significance.
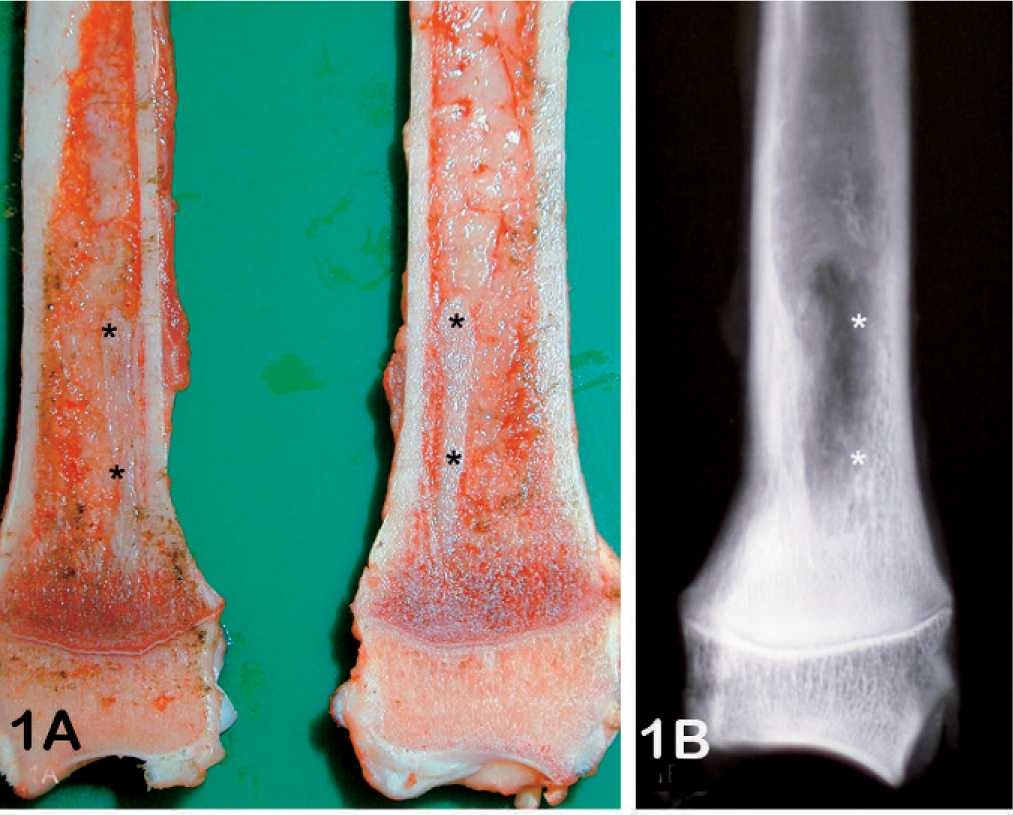
Radius; dog. Gross morphology of the sliced bone (A). The fibrous tissue (asterisks) visible on the cut surface of the bone marrow of the distal radius (A) appears as a radiolucent area (asterisks) on the radiographs (B) taken on the same specimen.

Radius; dog. Histologic examination revealed that the tissue consisted of a loosely packed, fibrous tissue infiltrating between, and blending with, bone trabeculae, thereby creating the striated pattern. HE.
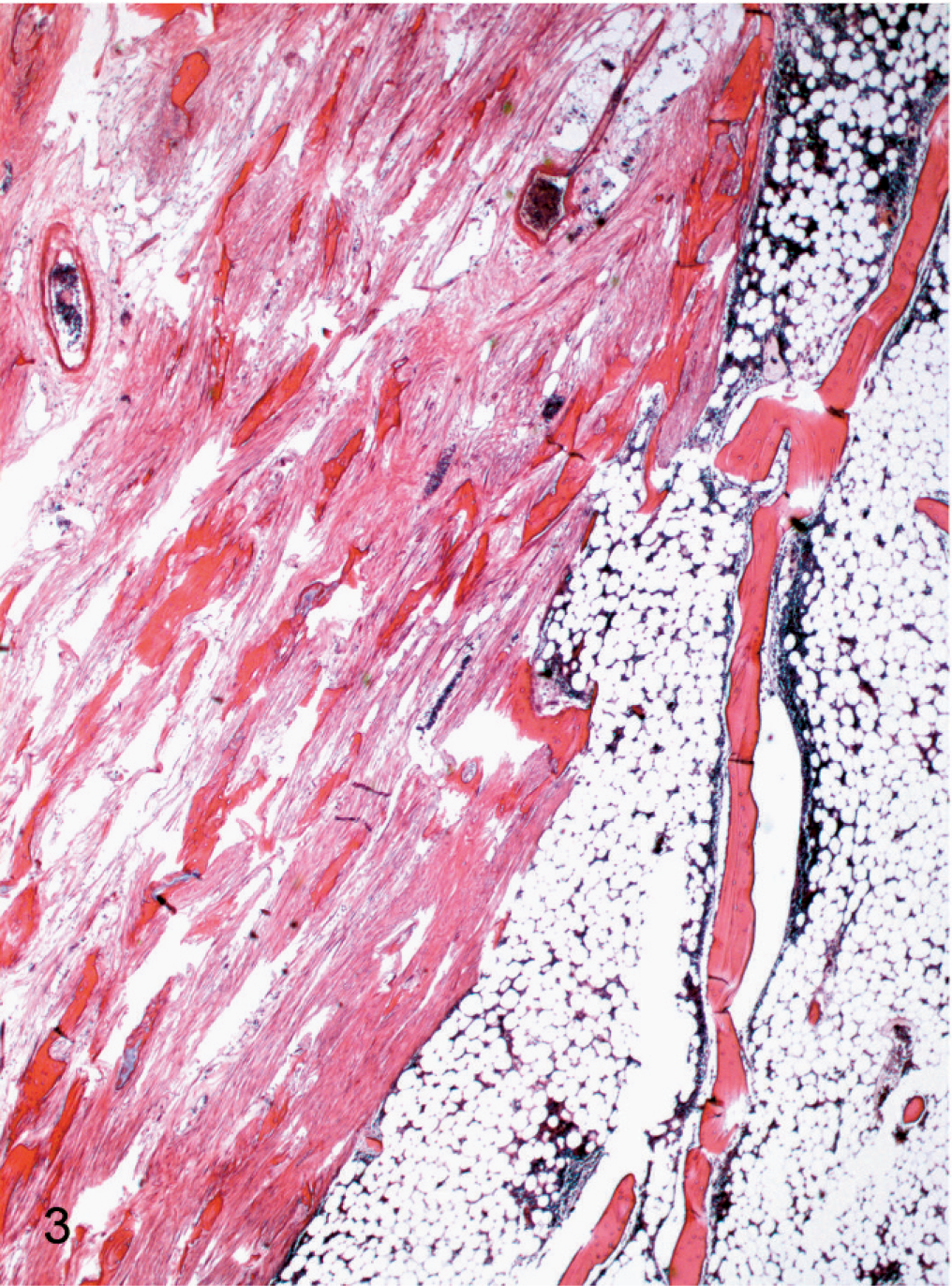
Radius; dog. The fibrous tissue was sparsely cellular. The bone trabeculae were relatively thin and delicate compared with the surrounding areas of cancellous bone. HE.
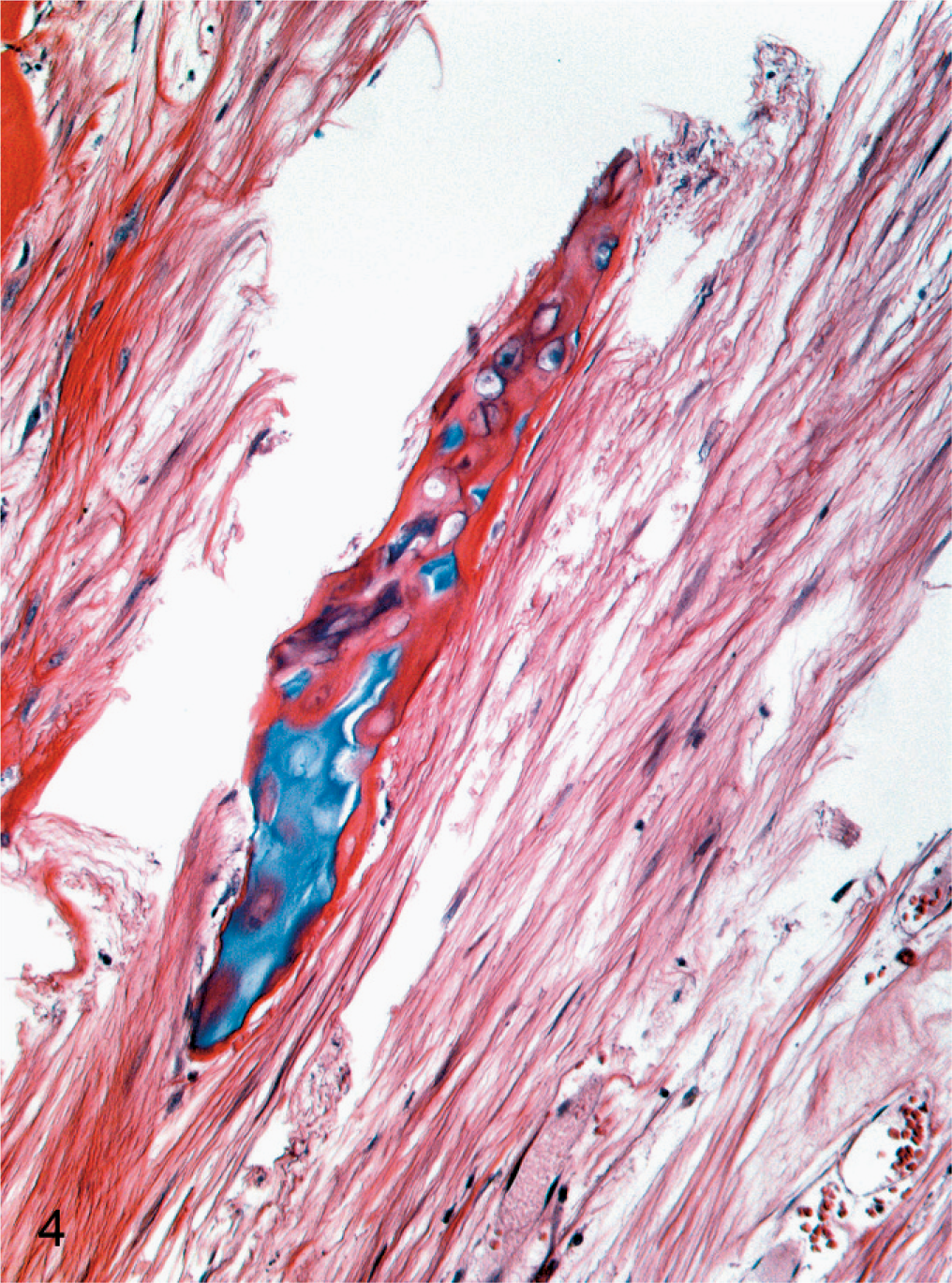
Radius; dog. The bone trabeculae within the fibrous tissue sometimes had central areas of mineralized cartilage. HE.
Footnotes
Acknowledgements
We thank Prof. Dr. Jon Teige and Dr. Arild Espenes, Department of Basic Sciences and Aquatic Medicine, Norwegian School of Veterinary Science, for helpful discussions and for performing the necropsy, respectively.