
Abstract
A 7-year-old, female European shorthair cat with a history of recurrent vomiting had a 2-cm cystic mass in the midjejunum. Cross-sectioning and histology revealed 3 separate cystic structures in the muscular layer, in addition to a regularly structured intestinal lumen. One cyst had a 3-layered wall consisting of a dysplastic mucosa, a regularly structured submucosa, and partly double-layered muscularis that sporadically contained neurons resembling a myenteric plexus. The remaining 2 cysts had similar structures except for granulation tissue lining the lumen. The lesion was diagnosed as multiple cystic duplications in the midjejunum, which is unknown to the veterinary literature to date.
Duplications of the gastrointestinal tract are uncommon congenital abnormalities. By definition, they are lined by intestinal mucosa, contain smooth muscles in their walls, and are located in or adjacent to the wall of a gastrointestinal tract section. 8 They are well-documented in humans, especially infants. 2, 5, 9 Documented cases in animals cover dogs, a cat, foals, and goats. 3, 4, 6– 8 Their localization in the alimentary tract and their inner lining may differ widely, and diverse theories in terms of their formation during embryogenesis have been discussed. 5 Here, we describe the first case of multiple intestinal duplications in the jejunum of a cat.
A 7-year-old, spayed female European shorthair cat was presented with recurrent vomiting for several years. Diagnostic laparatomy revealed a focal multicystic mass in the mid region of the jejunum with a longitudinal extension of 2 cm and 1 cm in diameter. The mass was surgically excised and fixed in 4% formalin. Serial cuts were examined macroscopically before the slices were routinely processed for histology.
Macroscopically, a regular jejunal lumen of up to 1 cm in diameter was centrally located in the mass. In addition, the muscular layer contained 3 additional cystic structures (Fig. 1). None of these cysts was connected to the regular jejunal lumen. The largest cyst was ovoid in shape, 1 cm in diameter, and located in the mesenteric segment. Transverse sectioning of the 2 remaining cysts revealed cystic spaces of up to 0.7 × 0.3 cm in diameter. Sections were embedded in paraffin and routinely processed for histology. In addition to hematoxylin and eosin (HE) staining, van Gieson, periodic acid–Schiff (PAS), and Weigert's elastica stains were performed for further structural characterization. Immunostaining with polyclonal antibodies for alpha–smooth muscle actin (SMA) was performed using the avidin–biotin–peroxidise complex (ABC; Vectastain Elite, Vector Laboratories, Inc., Burlingame, CA) method.
Histologically, the centrally located regular intestinal lumen had a typical intestinal 3-layered structure, consisting of normal mucosa, submucosa, and muscularis (Fig. 1). The lumen contained ingesta, and the mucosa was normal. The wall of the larger cyst located between the regular lumen and the mesentery had a similar composition, with an inner layer consisting of an intestinal mucous membrane with columnar epithelial cells, scattered cryptlike glands, and villous protrusions into the lumen (Fig. 2). Epithelial cells had basal nuclei and apical eosinophilic cytoplasm, sometimes containing PAS-positive vacuoles (Fig. 4). PAS-positive goblet cells with secreted mucins were rarely interspersed throughout the epithelium. Most epithelial cells were cuboidal, but some regions also had more flattened epithelial cells (Fig. 5). Villous epithelial protrusions contained smooth muscle cells, confirmed by immunohistochemical staining for SMA (Fig. 6). In the connective tissue underneath the mucosa, a thin layer of smooth muscle cells reminiscent of a lamina muscularis mucosae was present, under which a sparse fibrovascular connective tissue contained sporadic lymphocytes and plasma cells. The tunica muscularis was predominantly separated in a circumferential and longitudinal layer of smooth muscle cells, sporadically interspersed with neurons resembling a myenteric plexus (Fig. 7). Elastic fibers arranged in loose concentric bands around the cyst as seen in normal intestinal submucosa were identified by Weingart's elastica stain. The 2 remaining cysts had similar walls except for the absence of an inner epithelial lining. Instead, the cysts were lined by granulation tissue with multifocal mild hemorrhage and macrophages containing hemosiderin. Moderate fibrin exudates sporadically covered the luminal surfaces of the granulation tissue, partially associated with small numbers of neutrophils (Fig. 3, inset). Mucinous PAS-positive material but no ingesta was detected in the lumen of all 3 cysts. No communications were present between the cysts and the regular jejunal lumen. Some smooth muscle layers between the cysts and the intestinal lumen completely surrounded the cysts, while others fused and were discontinuously shared by more than 1 cyst or a cyst and the intestinal lumen, respectively. Complete surgical removal of the mass resulted in complete recovery of the cat. In conclusion, the multicystic structure was diagnosed as multiple cystic intestinal duplications, 2 of which with granulation tissue substituting for the epithelial lining.
Gastrointestinal duplications are rare congenital anomalies appearing most commonly in the ileum and the esophagus. Several features of the lesion described here make this case unique among intestinal duplications described earlier. All cases described in foals were located in the esophagus, whereas 1 case in a goat had a duplication of the lower urinary and genital tracts as well as a complete intestinal duplication starting in the midjejunum and resulting in 2 anal openings. The single duplication described in a cat was located in the midjejunum but lined with esophagus-type epithelium. 7 In general, the case presented here shares all characteristics of intestinal duplications: a location adjacent to the intestinal lumen, a wall composed of smooth muscles, and a lining by intestine-like mucosa. 2 All structures of a regular intestinal wall were present in 1 cyst, whereas the mucosal lining was absent in the remaining 2 and instead replaced by granulation tissue. There was no communication between the cysts and the unchanged intestinal lumen. The granulation tissue that lined 2 of the cysts was considered a secondary inflammatory change following epithelial atrophy and loss, possibly a result of pressure by mucosal secretions. Heterotopic gastric mucosa or pancreatic tissue as reported frequently in such lesions and causing loss of epithelial lining 5 was not seen in this case. Thus, both the multiplicity and the replacement of the mucosal lining by granulation tissue make the case described here unique among previously described cases. The most important differential diagnoses include intestinal diverticular malformations and diverticulitis. The former are also congenital and occur in the small intestine of dogs and cats as well as in other species like rat, sheep, and pigs. 1 In contrast to humans commonly showing asymptomatic clinical courses, documented cases in dogs and cats usually presented with clinical signs, mostly vomiting. 1 The differential diagnosis of multiple intestinal diverticular malformations can be ruled out here by the lack of any communication with the regular intestinal lumen.
In summary, the lesion presented here is consistent with multiple cystic intestinal duplications, most likely resulting from congenital malformation. Their multiplicity and inner linings are unlike any such lesions described earlier.
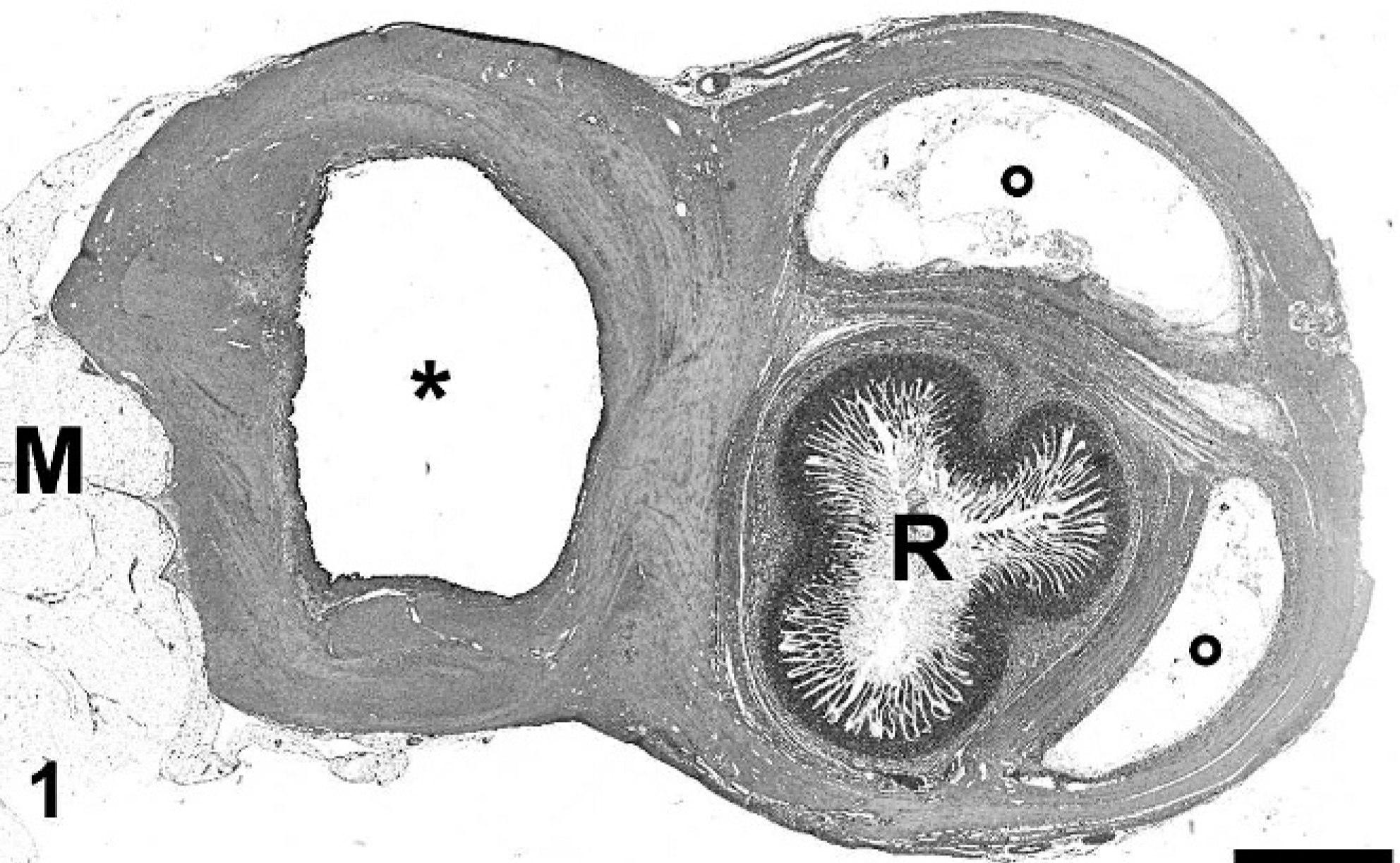
Cross-section of the jejunum and additional cystic structures. The largest cyst with mucosal lining (asterisk) is located in the mesenteric (M) segment. Additional cysts (circles) flanking the regular intestinal lumen (R) are lined by granulation tissue. HE. Bar = 2.7 mm.
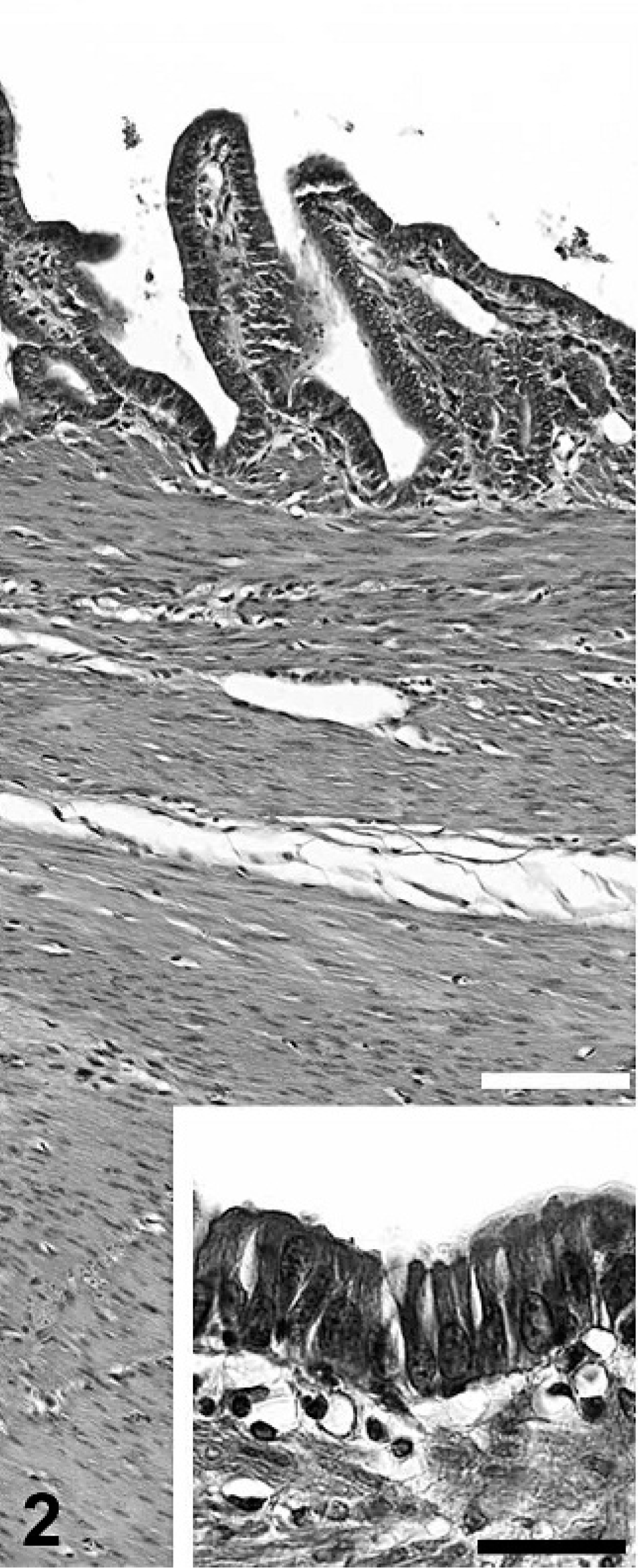
The wall of the largest cyst is lined by a regular mucosal membrane. HE. Bar = 100 μm. Inset: Higher magnification of the epithelial cells lining the cyst. HE. Bar = 30 μm.
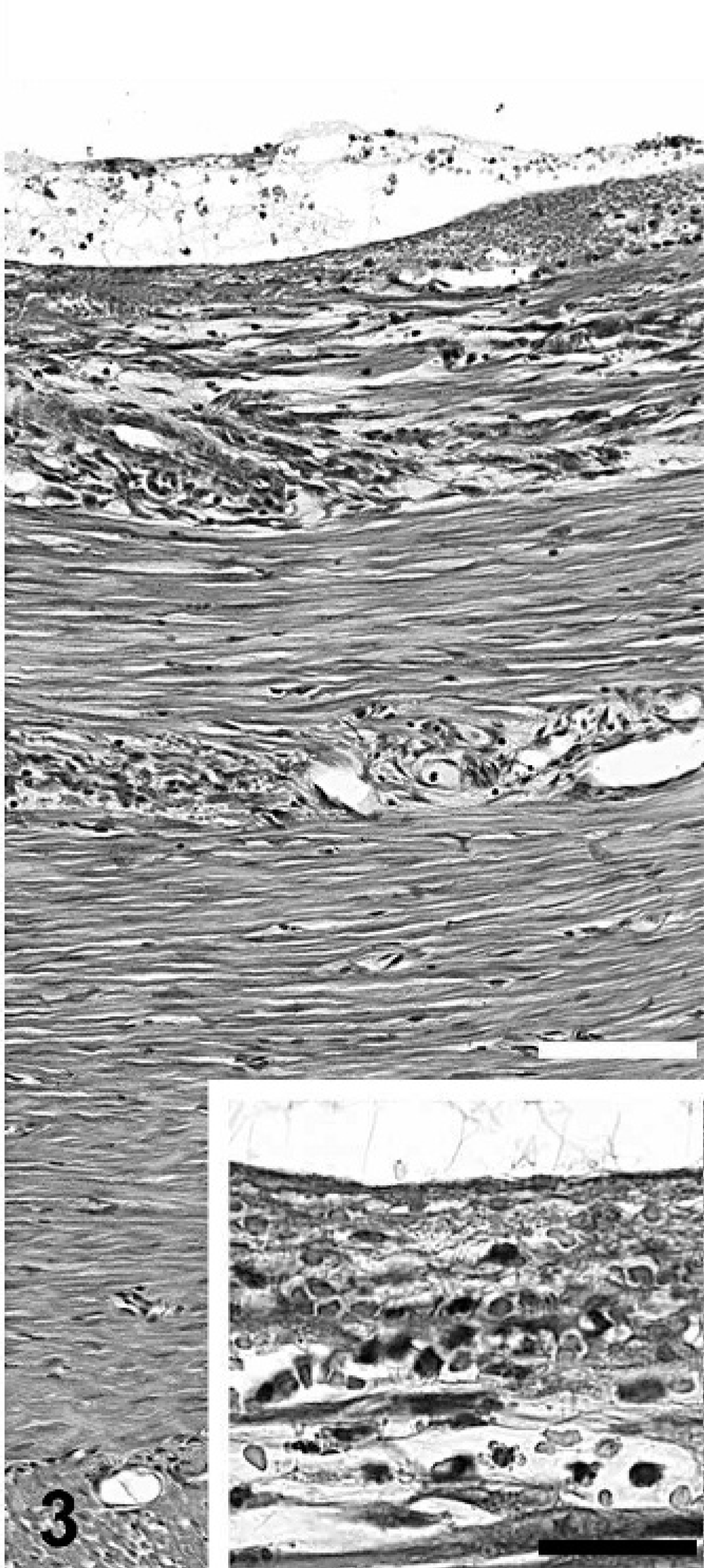
The wall of the 2 smaller cysts are lined by granulation tissue, cellular debris, and fibrin. HE. Bar = 100 μm. Inset: Higher magnification of the granulation tissue, debris, and fibrin lining the cysts. HE. Bar = 30 μm.
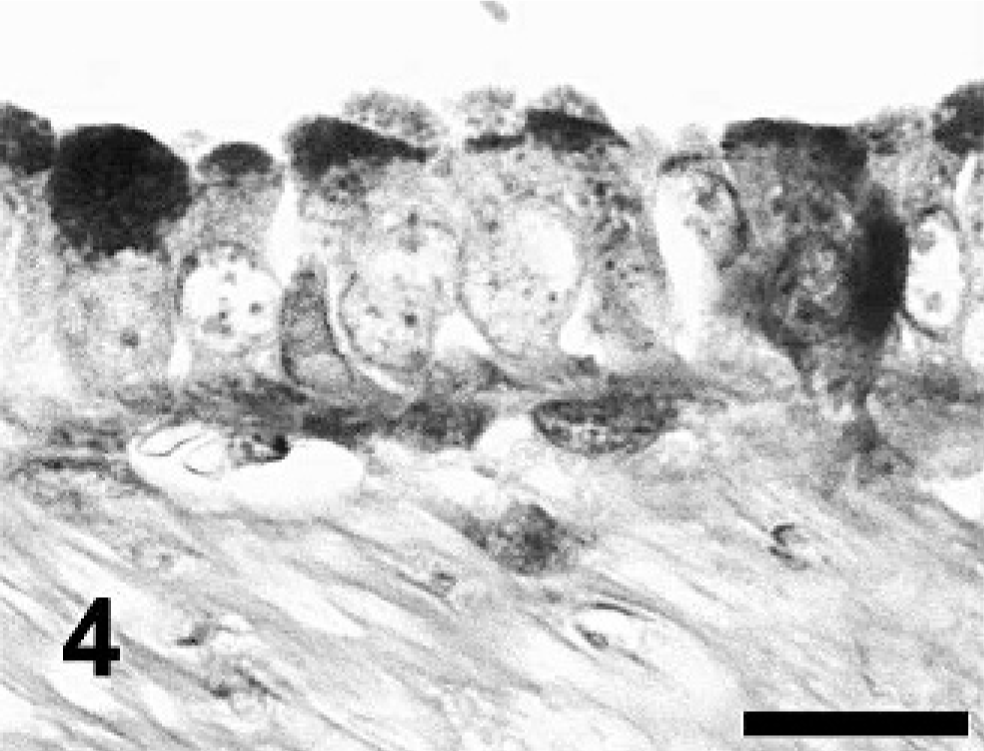
Mucosal lining of the largest cyst, located close to the mesentery, is consisting of cuboidal (Fig. 4) or flattened (Fig. 5) epithelial cells, respectively. PAS. Bar (for both) = 15 μm.
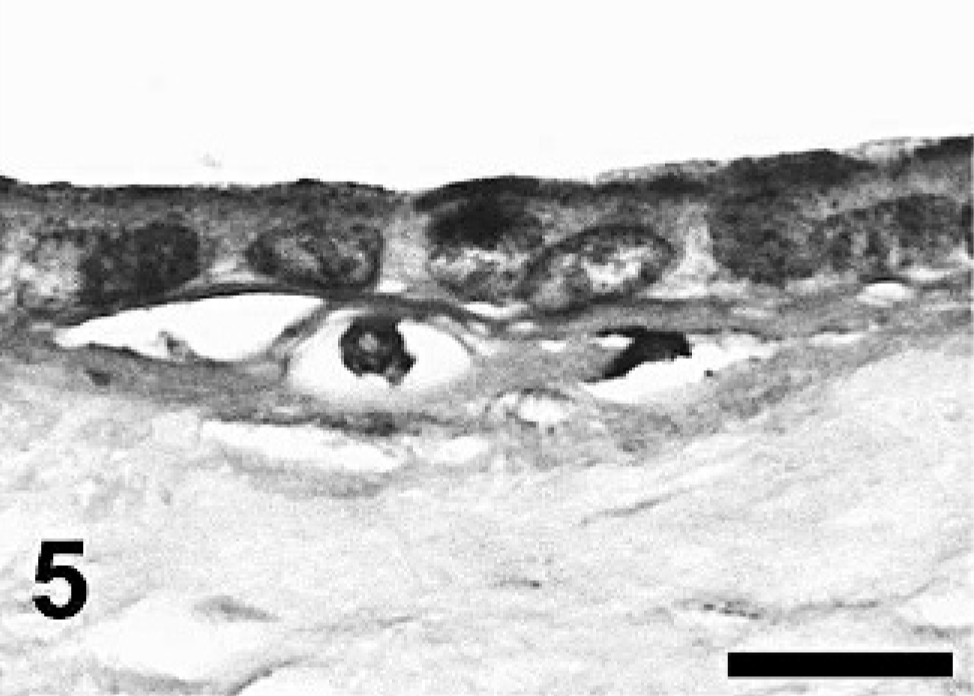
Mucosal lining of the largest cyst, located close to the mesentery, is consisting of cuboidal (Fig. 4) or flattened (Fig. 5) epithelial cells, respectively. PAS. Bar (for both) = 15 μm.
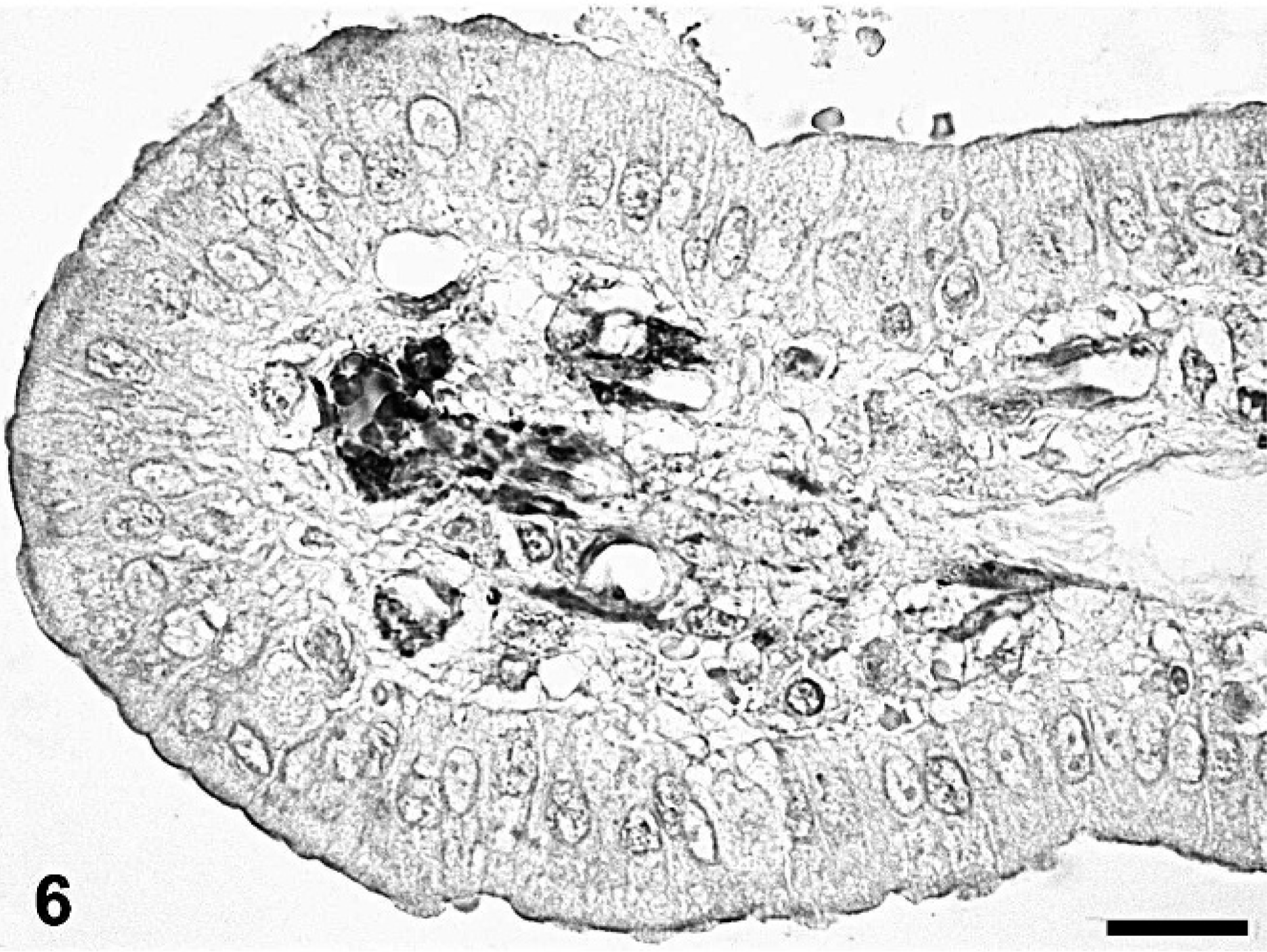
Villous tip of the mucosa lining the largest cyst. Smooth muscle cells stain positive for SMA in the lamina propria. Immunostaining for SMA with diaminobenzidine–tetrahydrochloride as substrate and hematoxylin counterstain. Bar = 20 μm.
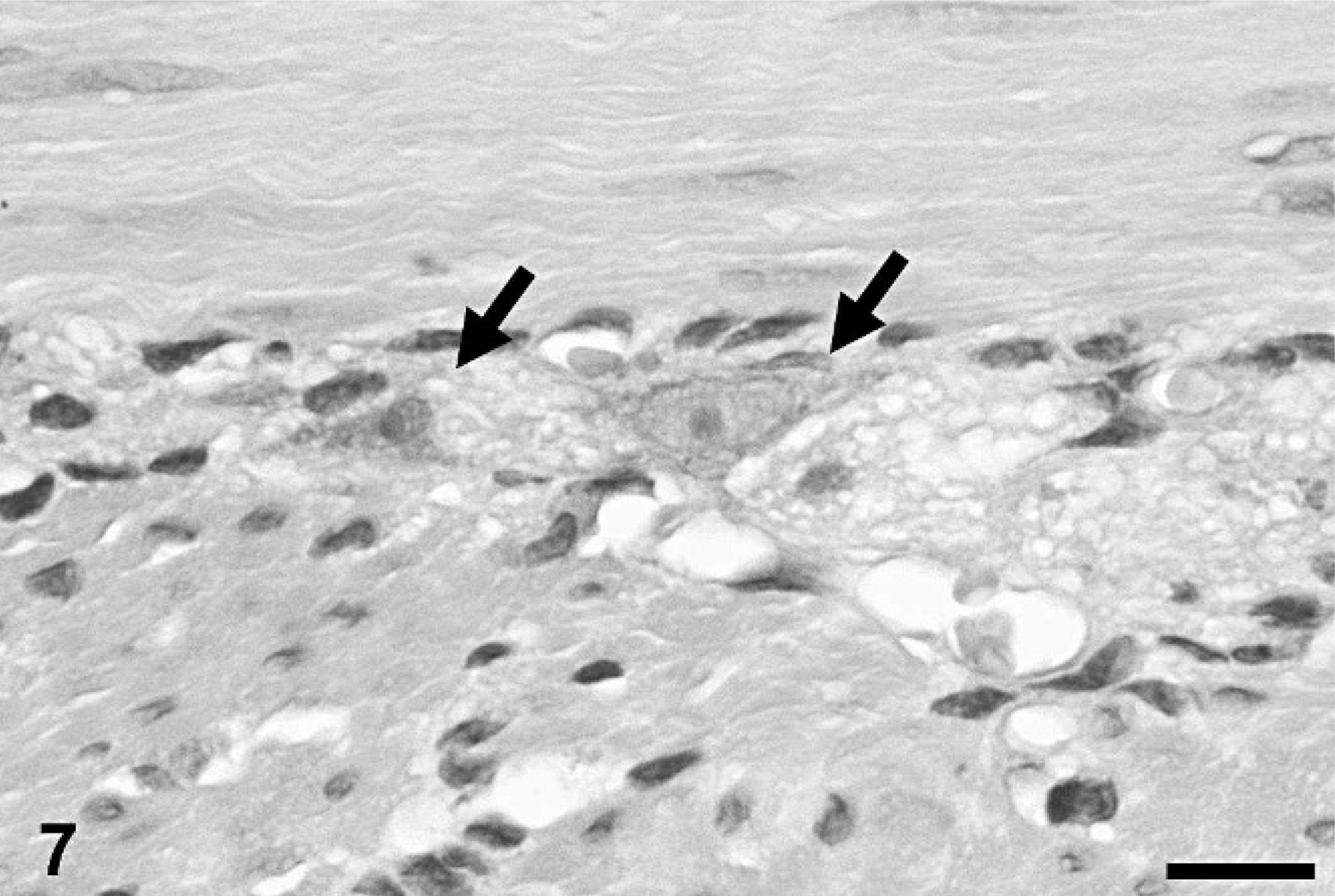
Tunica muscularis of one of the cysts lined by granulation tissue. The muscle layers were predominantly separated in a circumferential (top) and longitudinal (bottom) layer of smooth muscle cells, sporadically interspersed with neurons (arrows) resembling a myenteric plexus. HE. Bar = 15 μm.