
Abstract
A 12-year-old pregnant female giraffe (Giraffa camelopardalis reticulata) died approximately 2 months prior to her anticipated parturition date. At necropsy, a mass measuring approximately 20 x 36 x 20 cm was observed, attached to the umbilical cord, the latter being otherwise normal in appearance. Histologically, the mass contained 3 germinal tissue components with areas of squamous epithelium, respiratory epithelium, primitive neural tissues, glial tissue, peripheral nerve, adipose tissue, cartilage, and smooth muscle. Based on these findings, the tumor was diagnosed as a teratoma originating from the umbilical cord. This is possibly the second reported case of umbilical cord teratoma in animals.
Keywords
Tumors of the umbilical cord have rarely been reported in humans, and the majority of those reported have been angiomyxomas.5,10 In humans, teratomas originating from the umbilical cord are exceedingly rare, and only 11 reports of such cases exist in the world literature.9 Teratomas arise from pluripotent germ cells that differentiate into tissues from at least 2, and usually 3, of the embryonic layers, that is, the endoderm, mesoderm, and ectoderm.7 Teratomas are infrequently observed in animals, the most common being those in the ovaries of bitches and the testes of stallions.7 To our knowledge, although such tumors have been described in humans, there have been no reports but one3 describing tumors of the umbilical cord, including umbilical teratomas, in animals.
A 12-year-old female pregnant giraffe (Giraffa camelopardalis reticulata), which had 5 previous normal parturitions, died about 2 months before parturition. No clinical disorders had been observed until 2 weeks before death, at which point the animal developed anorexia and exhibited abdominal turgescence.
At necropsy, a tumor mass measuring approximately 20 × 36 × 20 cm was attached to the umbilical cord about 8 cm from the abdominal wall; the cord was otherwise normal in appearance. The mass was mostly covered with a thin, glistening membrane (Fig. 1). The umbilical cord was closed from the abdominal wall to the mass. The umbilical artery was seen extending from the margin of the mass (Fig. 2). On the cut surface, no skeletal axis could be identified. The fetus appeared morphologically normal, with neither dysmorphism nor external malformation. The animal had a large amount of amniotic fluid in the amnion.
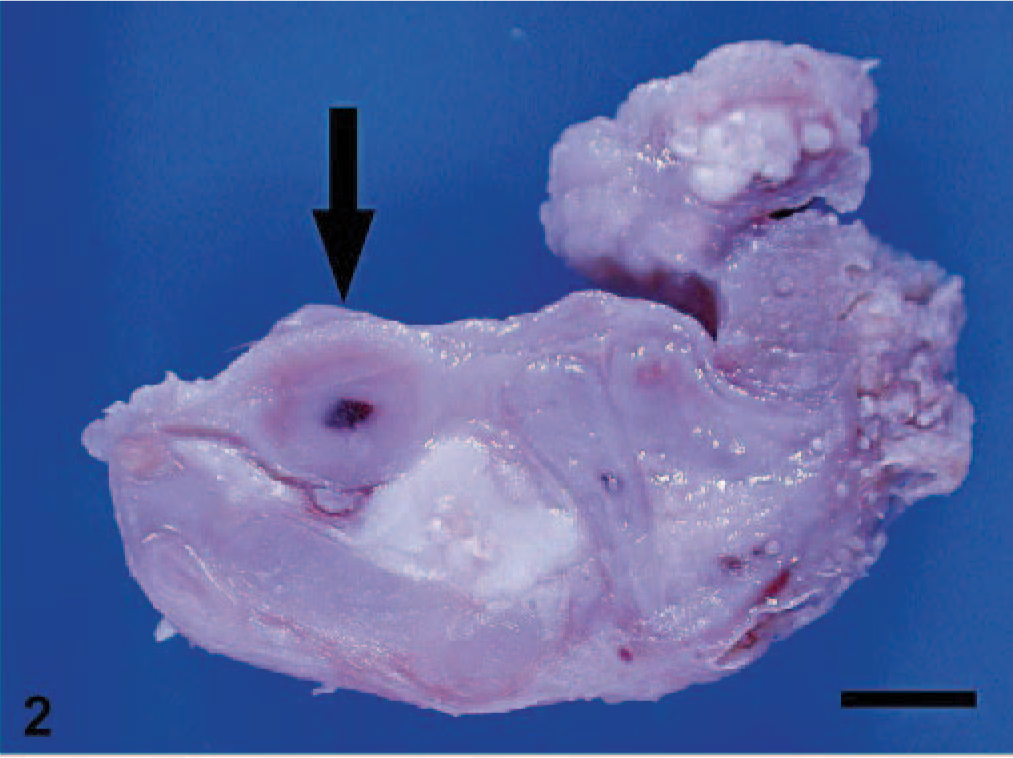
Teratoma; giraffe. Umbilical artery embedded in teratoma (arrow). Bar = 5 mm.

Teratoma; giraffe. A 20 × 36 × 20-cm tumor mass of the umbilical cord.
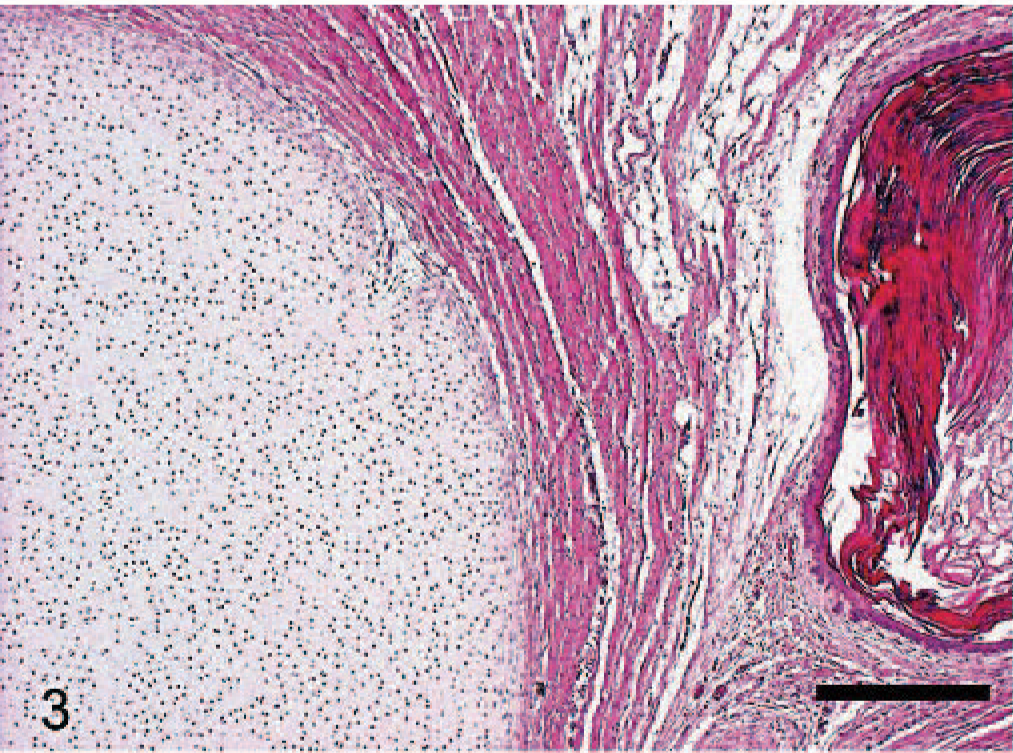
Histologically, the umbilical tumor mass consisted of various tissue components derived from the 3 germinal layers, characterized by various amounts of mesenchymal tissue, adipose tissue, cartilage, and smooth muscle (Fig. 3). A cystic integumentary component characterized by stratified squamous epithelium with ballooning degeneration and keratinization (Fig. 4), adnexal components, and sweat glands was also seen. An esophageal-like component with nonkeratinized squamous epithelium was present. It was continuous with an area of ciliated columnar epithelium with prominent mucus production that resembled respiratory epithelium (Fig. 5). There were also primitive neural tissue components (Fig. 6), which exhibited a positive reaction to S-100 immunohistochemically, as well as more differentiated glial tissues and peripheral nerve tissues. No organic structures, such as the liver, kidneys, lungs, or heart, were seen. Teratomas of the umbilical cord that have previously been reported contained various tissues, as in this case. These tissues were squamous epithelium,3 adipose tissue, cartilage,5 and organs such as hepatic cells, pancreatic glands,9 and colonic epithelium.10 Areas of nonsquamous epithelium that change into respiratory epithelium5 and immature nervous tissue9 have been reported, as in this case. The tumor components of this case showed no cellular atypia or other evidence of malignancy.
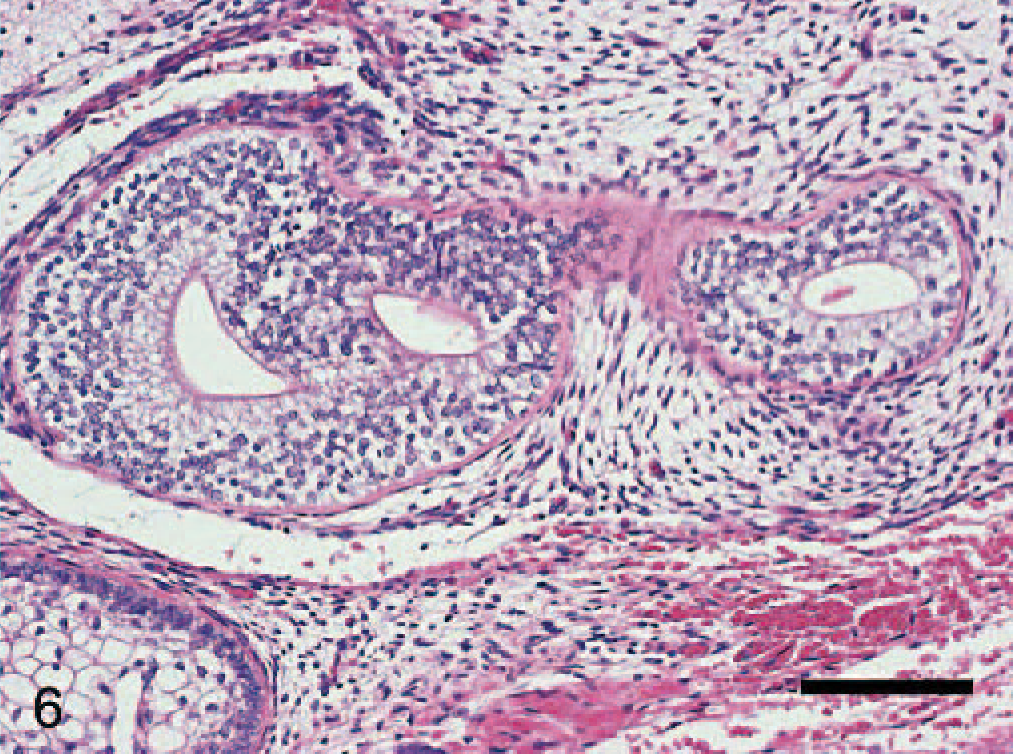
Teratoma; giraffe. Immature neural tissue. HE. Bar = 100 μm.
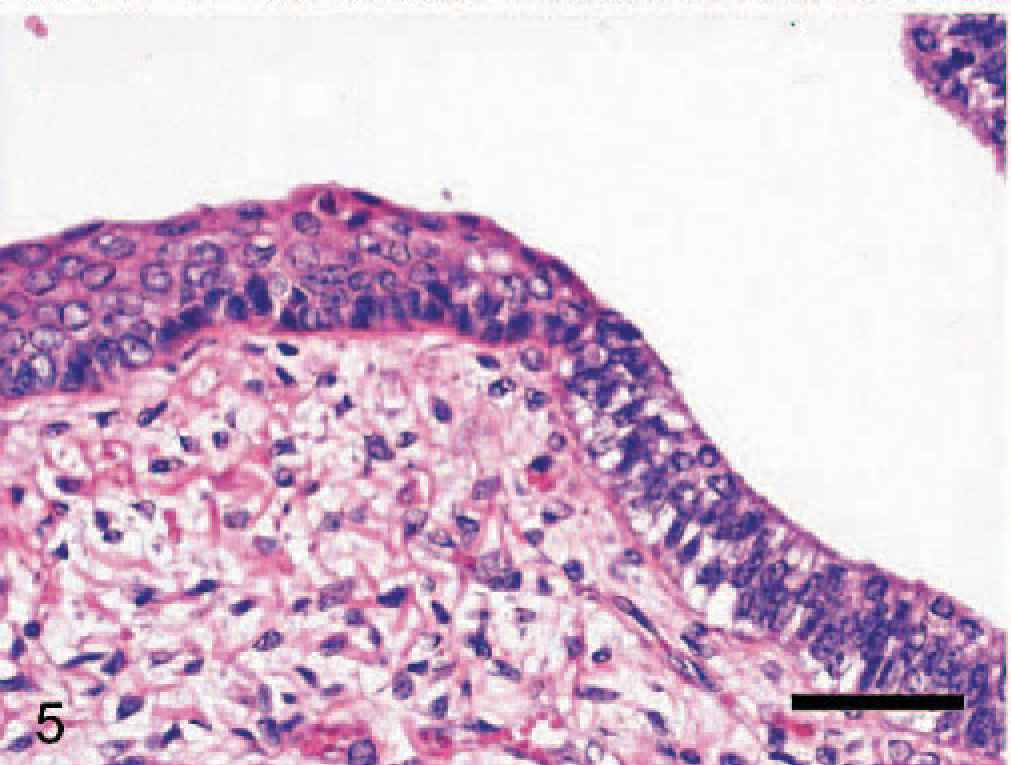
Teratoma; giraffe. Nonkeratinized squamous epithelium and ciliated columnar epithelium with prominent mucus production. HE. Bar = 50 μm.
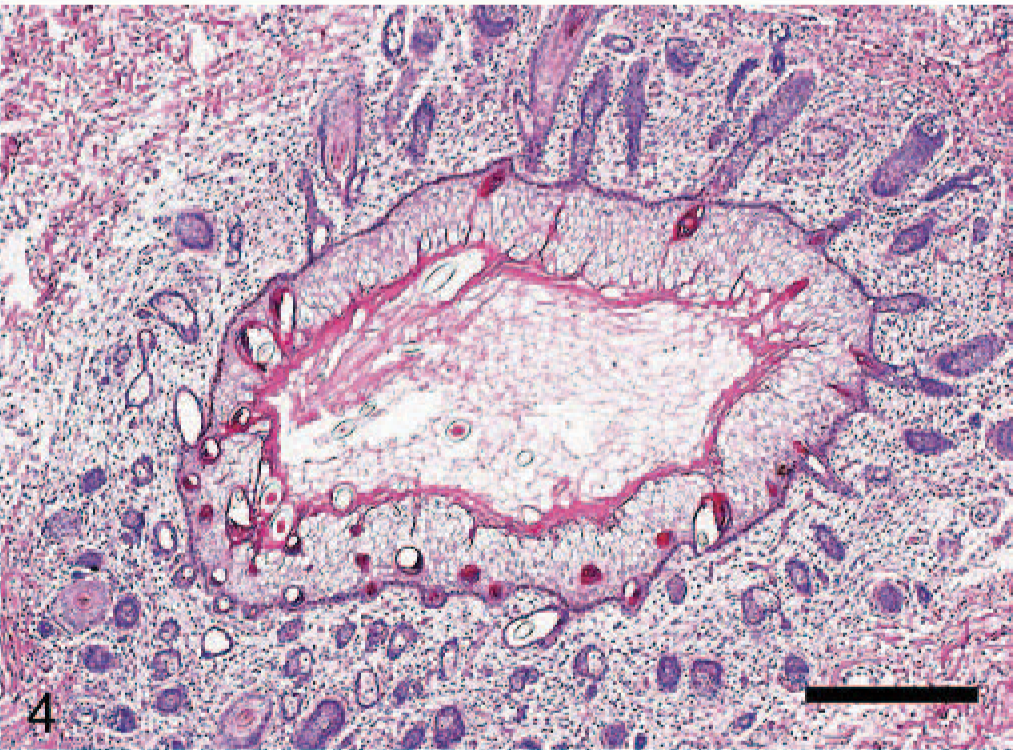
Teratoma; giraffe. Cyst with squamous epithelium with ballooning degeneration and keratinization. HE. Bar = 250 μm.
Teratoma; giraffe. Cartilage and squamous cell cyst. HE. Bar = 250 μm.
Based on gross and histologic findings, a diagnosis of teratoma originating from the umbilical cord was made. There were no abnormalities on any organs in either the animal or the fetus.
Although 11 cases of umbilical teratomas in humans had been reported as of 2001, there have been no reported cases of umbilical teratomas but one3 in animals. In humans, umbilical teratomas have been thought to be biologically benign and primitive,9 and this is consistent with what we observed in the present case.
Teratomas arise from germ cells, either in the gonads or occasionally from germ cells that mistakenly stray to ectopic sites during migration from the yolk sac to the genital ridges during embryonic development.4,11 Umbilical teratomas are believed to arise from germ cells that migrate out of the wall of the invaginated gut into the loose connective tissue of the umbilical cord. If these germ cells continue their migration, they may arrive at the placenta between the amnion and chorion, and can give rise to a teratoma at this site.2
Smith and Majmudar10 stressed the importance of distinguishing between holoacardius amorphus and teratoma. The holoacardius amorphus is one form of asymmetric duplication or a monozygous twinning. Because of the different geneses of the 2 lesions, it is important to differentiate between them.5 Fox and Elston distinguished between these 2 entities by defining fetal acardius amorphus as follows:
Teratomas usually have some bone tissue component, which generally exhibits complete disorganization and never have their own umbilical cord.
Teratomas of the umbilical cord generally are considered to have no major influence on the life expectancy of the fetus in humans,5 but cases of premature birth in humans and abortion in equines have been reported. The features of umbilical teratomas described in these reports were supportive of the diagnosis of teratoma originating from the umbilical cord in the present study.
The 11 umbilical cord teratomas in humans that have been reported were considered to be benign, except in 1 case.9 Furthermore, despite the large volume in some of the tumors, few obstetric combinations have been reported. One fetus was reported to have died during pregnancy, a month before birth, because of a small vascular rupture near the placenta.6 In the present case both the animal and the fetus died, with their deaths possibly having been influenced by an abnormal increase in amniotic fluid. Because the fetus showed no gross or macroscopic abnormalities, polyhydramnios might not have been associated with fetal heart failure as previously reported.8 It is suggested that the fetus may have been compressed by the tumor, causing polyhydramnios in the umbilical cord hemangioma,1 and similar circumstances may have occurred in the present case. Gurfield and Benirschke cited that topologic differences in the type of placentation between equines and humans might relate to the likelihood of abortion.3 Giraffes also have a different topology and type of placentation than humans, which may have contributed to their deaths in this case.
The present case is an extremely rare case of umbilical cord tumor. In animals other than humans, no umbilical cord tumors have been reported except for 1 case;3 thus, the present case may be the second reported case of an umbilical cord teratoma.
Footnotes
Acknowledgements
We thank Ms. Cate Swift for grammatical proofreading of the manuscript. This study was partially supported by a Grant-in-Aid for Scientific Research (The 21st Century Center-of-Excellence Program) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan.