
Abstract
An 8-month-old, female, mixed-breed dog presented to the Iowa State University Veterinary Teaching Hospital with a 1-month history of vomiting and diarrhea. An exploratory laparotomy was performed revealing markedly distended and fluid-filled small and large intestines that were not obstructed. The clinical condition of the dog did not improve subsequent to exploratory surgery, and it was euthanized. At necropsy, both the small and large intestines were distended (approximately 4 cm in diameter) and fluid-filled, and the wall was thin. The abdominal cavity contained approximately 500 ml of a brownish clear fluid. Microscopic lesions of the intestines were confined to the intestinal tunica muscularis and muscularis mucosae and consisted of locally extensive-to-diffuse replacement of the smooth muscle by fibrous tissue and multifocal infiltration by a moderately dense mononuclear inflammatory infiltrate. A unique finding was the presence of similar microscopic lesions in the tunica muscularis of the urinary bladder and stomach.
Chronic intestinal pseudo-obstruction (CIPO) is an uncommon clinical syndrome in veterinary medicine, characterized by impaired intestinal motility that results in clinical signs of obstruction without evidence of mechanical occlusion of the intestinal lumen. The syndrome has been described in multiple dogs, a horse, and a cat. 1, 2, 5, 6, 10, 11, 16, 17 In human medicine, the underlying abnormality of CIPO can often be broadly classified as a neuropathy, myopathy, or mesenchymopathy (injury to the interstitial cells of the Cajal network). 4, 14 Fibrosis and infiltration of the smooth-muscle fibers of the tunica muscularis by mononuclear cells are the most frequently reported microscopic lesions of CIPO in the dog. 5, 6, 10, 11 This report describes the gross and microscopic lesions of a case of CIPO in a young dog.
An 8-month-old, mixed-breed, female dog presented to the Iowa State University Veterinary Teaching Hospital with a 1-month history of vomiting and diarrhea. The dog was negative for parvovirus antigen (SNAP® Parvo antigen test) and had impaired intestinal transport as indicated by a barium study performed by the referring veterinarian; barium was still present within the intestines 10 days following its administration (small intestinal transit time for barium is approximately 3-5 hours). On physical examination, the dog was mildly dehydrated and had enophthalmos, a distended abdomen, and elevation of the nictitating membrane. Abdominocentesis was performed, and on cytologic examination, a small amount of a serosanguineous fluid containing a small number of neutrophils was observed. The following day an exploratory laparotomy was performed. The intestines were markedly distended with fluid and gas and were thin-walled. In addition, approximately 500 ml of a serosanguineous fluid was present in the abdominal cavity. Full-thickness biopsies of the jejunum and duodenum were taken. The biopsy results indicated that there was marked atrophy of the tunica muscularis and a lymphocytic ganglioneuritis within the small intestine. Subsequent to surgery, an ophthalmology consultation was requested. The Schirmer tear test results were within normal limits, and the pupillary light responses were present. On the basis of the dog's deteriorating clinical condition and biopsy results, the dog was euthanized and submitted for necropsy.
At necropsy, the anus was covered by watery, light-green feces. The degree of autolysis was minimal, and the body condition of the dog was adequate. The abdominal cavity contained approximately 500 ml of a brownish clear fluid, and both the small and large intestines were distended (approximately 4 cm in diameter). The intestinal wall was thin, but not rigid. The intestinal contents were bright green, fluidlike, and covered with mucus but became darker green and more dry aboral. In the lungs, pulmonary artery thrombi associated with small areas of edema were present. A complete set of tissues was obtained for histopathology. With respect to the intestinal tract, samples of stomach, duodenum, jejunum, ileum, and large intestine were collected.
Tissue samples were fixed overnight in 10% neutral buffered formalin, embedded in paraffin, and stained with HE. Selected sections of tissue were stained with Masson trichrome or periodic acid-Schiff (PAS) stains or stained by a standard streptavidin-biotin-immunoperoxidase method for smooth-muscle actin, neuron specific enolase (NSE), CD3 (T-cell marker), or CD79 (B-cell marker).
The microscopic lesions of the small and large intestines consisted of locally extensive-to-diffuse infiltration of the tunica muscularis and muscularis mucosae by a moderately dense inflammatory infiltrate composed of lymphocytes, plasma cells, and a smaller number of macrophages and neutrophils, which sometimes surrounded blood vessels (Fig. 1). As demonstrated by immunohistochemistry, both T- and B-lymphocytes were present, but there appeared to be a greater number of T-lymphocytes. Additionally, there was locally extensive-to-diffuse replacement of the smooth muscle of the longitudinal and circular layers of the tunica muscularis and muscularis mucosae by an abundant amount of fibrous tissue. These observations were confirmed by Masson trichrome stain and immunohistochemistry for smooth-muscle actin. On the trichrome stain, individual smooth-muscle fibers were separated or replaced by stout bands of collagen, and scattered cells within the tunica muscularis were immunoreactive for smooth-muscle actin (Fig. 2). The lesions in the duodenum were relatively mild compared with the other segments of the intestinal tract, and significant microscopic lesions were not present within the mucosa of the small and large intestines. The PAS stain did not demonstrate fungal hyphae in the intestinal tunica muscularis. The myenteric and submucosal nerve plexuses were visualized. A small number of neurons had chromatolysis and a few were shrunken. Lymphocytes were occasionally associated with these ganglia. Immunohistochemistry was performed on selected sections for NSE to highlight the location of the myenteric and submucosal plexuses and to further confirm that the inflammatory infiltrate was not focused on the myenteric and submucosal plexuses (Fig. 3).
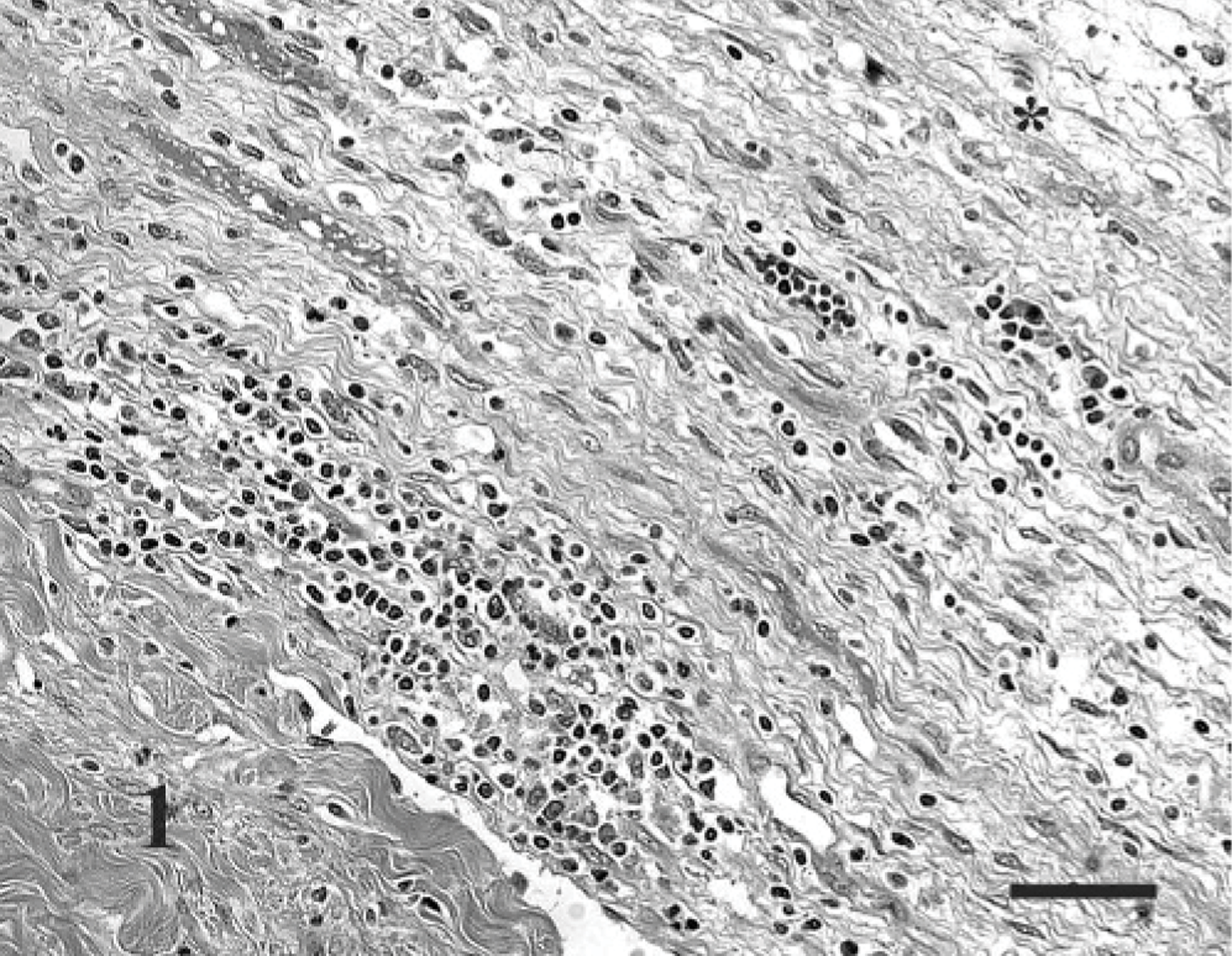
Small intestine; dog. The tunica muscularis is infiltrated by a moderately dense mononuclear cell inflammatory infiltrate. The asterisk (∗) indicates the serosal surface of the small intestine. HE; Bar = 40 μm.
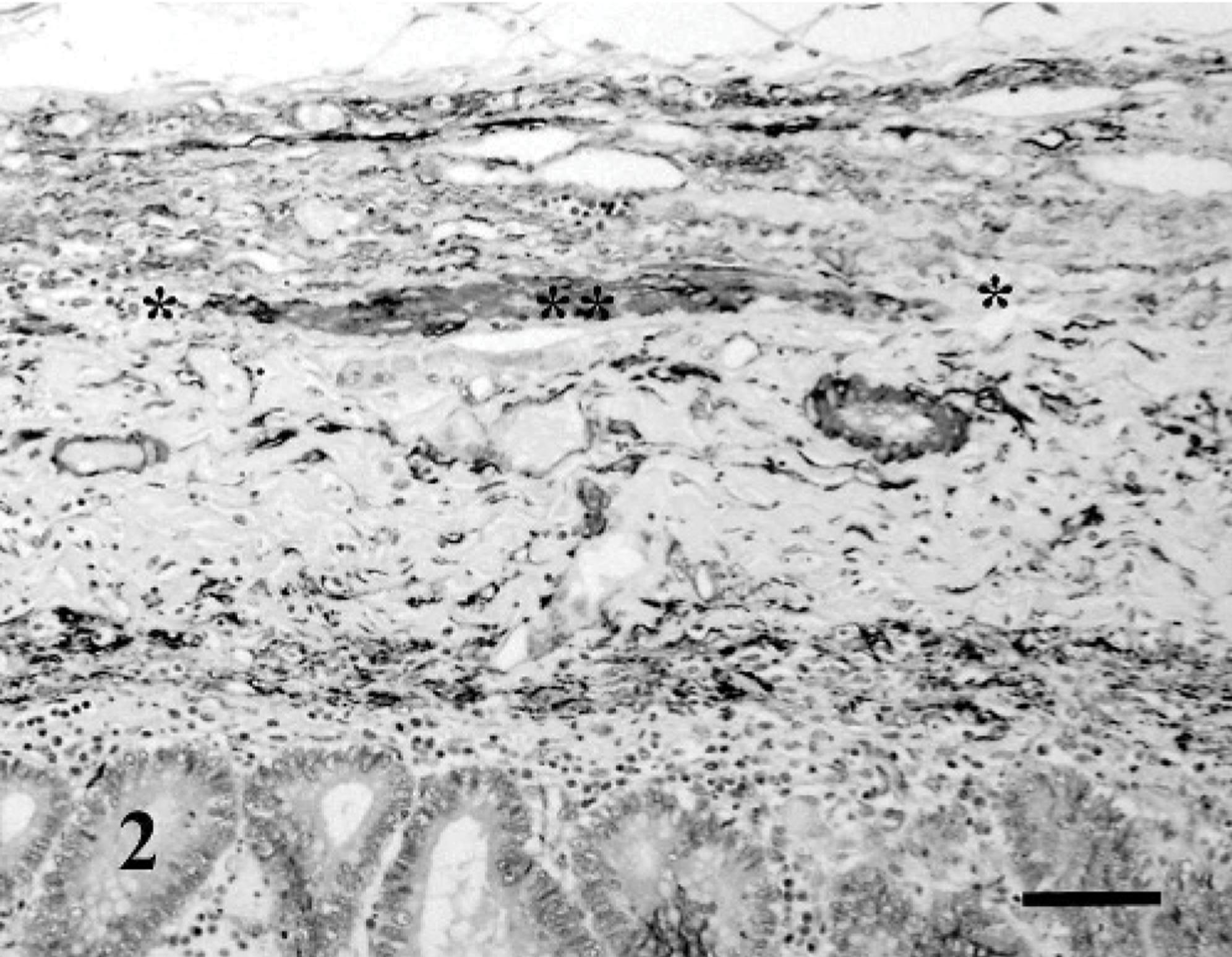
Small intestine; dog. Note the absence of smooth-muscle actin immunoreactivity (∗) immediately adjacent to a band of immunoreactive remnant smooth-muscle fibers (∗∗) within the tunica muscularis of the small intestine. Streptavidin-biotin-peroxidase method; Harris' hematoxylin counterstain; Bar = 60 μm.
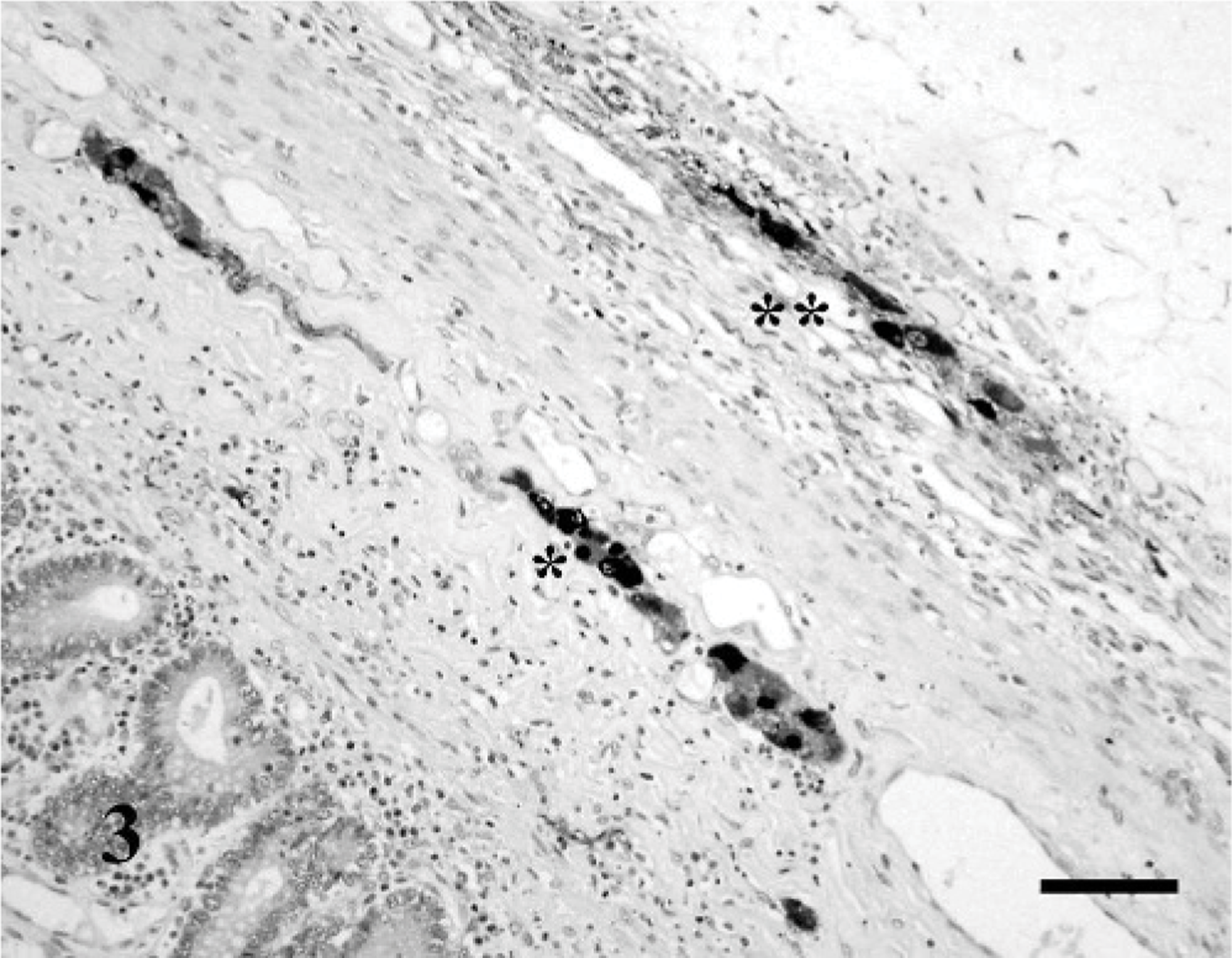
Small intestine; dog. Intense neuron-specific enolase immunoreactivity within the submucosal (∗) and myenteric (∗∗) plexuses. Inflammatory cells are not centered on the plexuses. Streptavidin-biotin-peroxidase method; Harris' hematoxylin counterstain; Bar = 80 μm.
Similar but less severe microscopic lesions were present within the tunica muscularis of the stomach and urinary bladder. Additionally, the lesions in these organs appeared to be more acute relative to the small and large intestine as suggested by multiple well-demarcated foci of smooth-muscle degeneration, manifested as multiple variably sized, round, clear cytoplasmic vacuoles within individual smooth-muscle fibers (Figs. 4, 5). Immunohistochemistry for smooth-muscle actin demonstrated weak-to-absent staining within the areas of smooth-muscle vacuolar change in the stomach and urinary bladder, and Masson trichrome stain demonstrated mild fibrosis within these areas, as well. However, the areas interpreted as mild fibrosis may, instead, represent the underlying stroma and not new collagen production. Smooth-muscle fibers in both organs were separated by a mild lymphoplasmacytic inflammatory infiltrate.
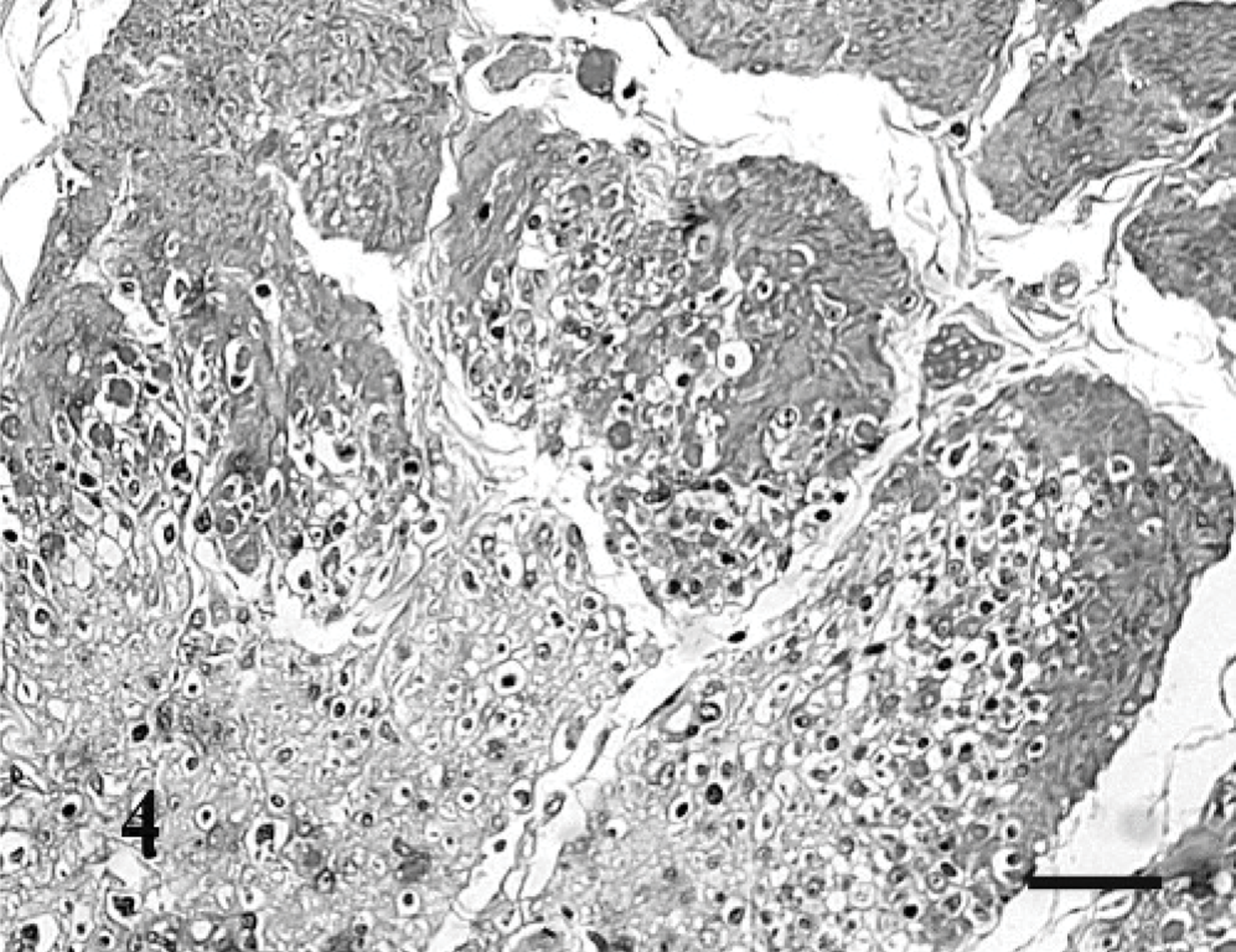
Stomach; dog. Smooth-muscle fibers of the tunica muscularis are expanded by multiple, variably sized, round, clear cytoplasmic vacuoles and are separated by a small number of mononuclear cells. HE; Bar = 60 μm.
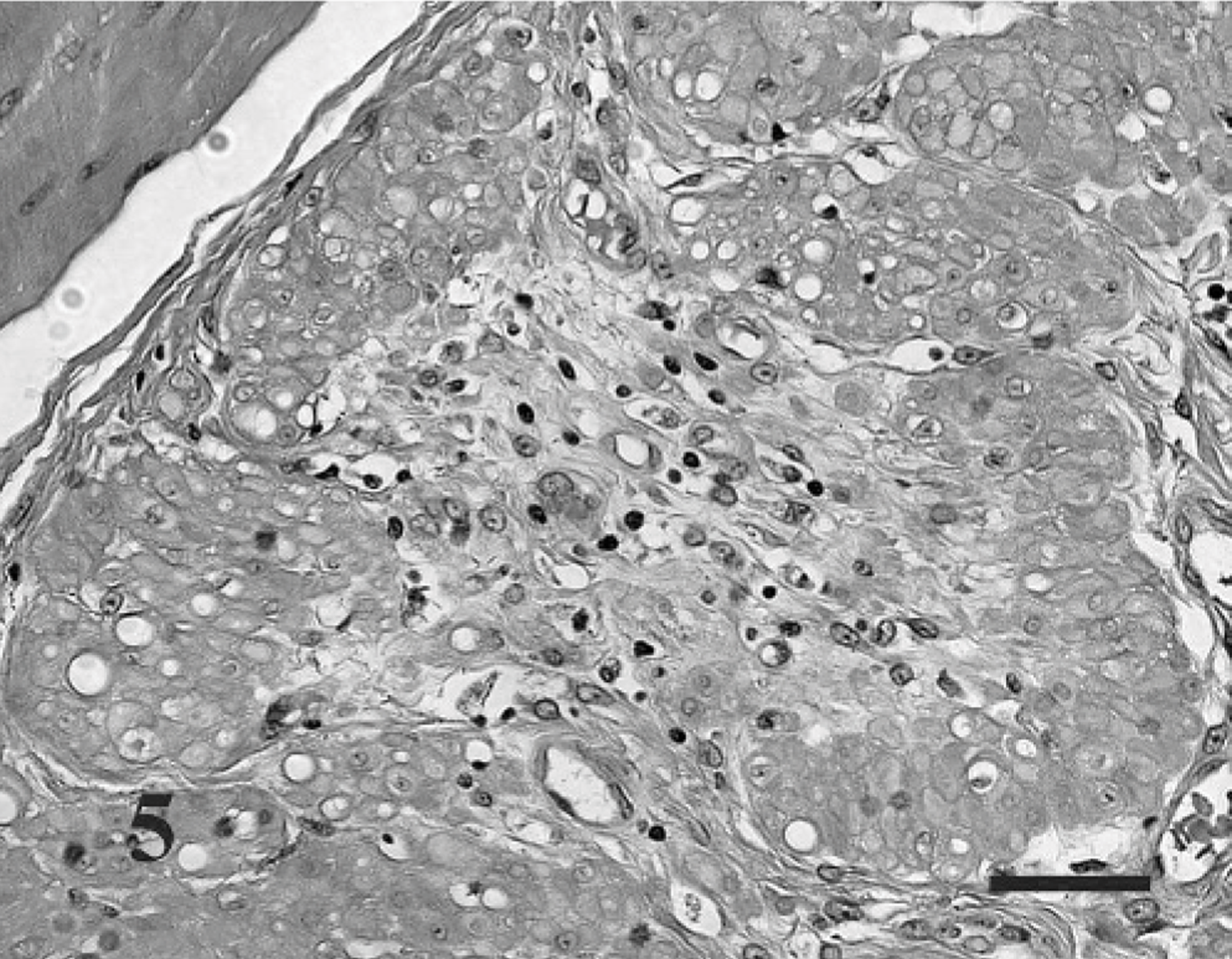
Urinary bladder; dog. Smooth-muscle fibers of the tunica muscularis are expanded by multiple, variably sized, round, clear cytoplasmic vacuoles and are separated by a small number of mononuclear cells. HE; Bar = 40 μm.
Intestinal motility is a complex process that involves contraction of smooth muscle, which is regulated by the pacemaker activity of the interstitial cells of Cajal, which, in turn, are fine-tuned by the intrinsic (enteric nervous system) and extrinsic nervous system (parasympathetic and sympathetic nervous system). Disturbances in any of these anatomic units may result in dysmotility that may subsequently lead to the development of CIPO. In veterinary medicine, CIPO is an infrequent cause of chronic vomiting, abnormal feces, and weight loss in both young and adult dogs. 1, 5, 6, 10, 11, 17 Fibrosis and infiltration of the tunica muscularis by mononuclear cells are commonly reported microscopic lesions in dogs diagnosed with CIPO. Of the reported cases, 6 of 8 have been described as having fibrosis and a mononuclear infiltrate within the tunica muscularis of only the small intestines or both the large and small intestines. 5, 6, 10, 11 This same lesion was also present in the small and large intestines of the dog in the present case report. In one previous case report, immunohistochemistry demonstrated moderate numbers of T- and B-lymphocytes within the intestinal lesions. 6 In the current case, both T- and B-lymphocytes were present; however, there appeared to be a greater number of T-lymphocytes within the intestinal lesions. In humans with intestinal leiomyositis, CD8+ T-lymphocytes are the predominant population of lymphocytes. 8, 13
Inflammation in previous reports has been restricted to the circular and longitudinal smooth muscle of the tunica muscularis, sparing the smooth muscle of the vascular walls, lamina propria, and the muscularis mucosae. In the present case, there was moderate segmental fibrosis and inflammation of the muscularis mucosae. Lesions of the muscularis mucosae have been reported in 2 canine cases of CIPO. One case was characterized by hypertrophy of the muscularis mucosae and hypoplasia of the tunica muscularis. 1 The other case had fibrosis of the interglandular and subglandular lamina propria and smooth-muscle hypertrophy of the muscularis mucosae. 17 A mononuclear inflammatory infiltrate was not present in either case.
The pathogenesis of the intestinal leiomyositis and fibrosis in dogs is not known. There appears to be no age, sex, or breed predilection. 1, 5, 6, 10, 11, 17 Leiomyositis as a cause of CIPO in humans has been described in adults and children. 8, 9 In some cases, the lesion is thought to develop secondary to a primary autoimmune disorder. For example, intestinal leiomyositis has been reported in an adult with systemic lupus erythematosus 9 and in a child with autoimmune hepatitis. 8 Leiomyositis as a cause of CIPO in children may also occur secondary to a primary gastrointestinal disorder, such as gastroenteritis. 8, 13
Neuropathy has not been a feature of the reported cases of CIPO in the dog. A small number of mononuclear cells may be associated with the myenteric and submucosal plexuses, but there are not an abundant number of inflammatory cells centered on them. Furthermore, there typically are not significant degenerative changes within the neurons of the myenteric and submucosal nerve plexuses. In the present case report, ganglia within the biopsy specimen were surrounded and infiltrated by a small-to-moderate number of lymphocytes; however, this change was not prominent within the samples of the stomach, duodenum, jejunum, ileum, or large intestine obtained at necropsy. The neurons that were shrunken and exhibited chromatolysis may represent injury secondary to the primary disease process, which was focused on the smooth-muscle fibers of the tunica muscularis.
Although a primary neuropathy was not considered to be the cause of the intestinal pseudo-obstruction in this dog, dysautonomia, which is a disorder of the autonomic nervous system, can result in intestinal dysmotility. In equine dysautonomia, or grass sickness, distention of the stomach and small intestine can occur, with neuronal degeneration in the peripheral autonomic ganglia being the primary histologic lesion. 3 Neuronal degeneration is also a feature of canine dysautonomia 12 but was not a significant feature in the myenteric and submucosal plexuses in the current case report. Additionally, it has been demonstrated that there is a reduction in NSE immunoreactivity in affected neurons in equine grass sickness, 7 which was not apparent in the sections of small intestine stained for NSE in the present case report. Last, the dog in the current case report did not exhibit clinical signs that are often present in dogs with dysautonomia, such as dysuria, a distended urinary bladder, mydriasis, dry mucous membranes, and a decreased Schirmer tear test. Another differential to consider, which was not ruled out, is a toxin such as Clostridium botulinum toxin type C, which is thought to be involved in the pathogenesis of equine grass sickness. 3
A unique feature of the present case report was the fibrosis and mononuclear inflammation within the tunica muscularis of the stomach and urinary bladder, which, to our knowledge, has not been reported in association with CIPO in veterinary medicine. The smooth-muscle changes within both organs appeared to be relatively acute on the basis of the vacuolar change within the myofibers, with a minimal amount of fibrosis and inflammation. A previous report of CIPO in a dog documented interstitial fibrosis within the stomach mucosa; 11 however, smooth-muscle changes were not noted within the tunica muscularis. Furthermore, vacuolar change within smooth-muscle fibers is not a lesion that has been reported consistently in canine cases of CIPO in veterinary medicine. One other report has documented vacuolar change within the enteric smooth-muscle fibers. 10 In human medicine, vacuolar change within enteric and urinary smooth-muscle fibers of the tunica muscularis is a unique feature of hollow visceral myopathy, 15 a cause of CIPO; however, unlike the present case, a mononuclear inflammatory infiltrate is not present within the lesions of patients who have hollow visceral myopathy.
In conclusion, fibrosis and infiltration of the tunica muscularis by mononuclear cells are common microscopic lesions in the small and large intestines of dogs diagnosed with CIPO. Since the lesion is frequently restricted to the tunica muscularis, it is essential to obtain full-thickness biopsies to obtain a definitive diagnosis. Furthermore, this is the first report describing leiomyositis in the stomach and urinary bladder of a dog with CIPO.
Footnotes
Acknowledgements
We would like to thank Drs. David K. Meyerholz and Kristi K. Mason for assistance with image analysis and thoughtful review of the manuscript.