
Abstract
A case of eosinophilic granulomatous gastroenterocolitis and hepatitis in a 1-year-old male Siberian Husky is described. The dog presented with a history of diarrhea, weakness, lethargy, and anorexia of several months' duration. Hematologic and biochemical examinations, abdominal ultrasonography, computer tomography, and exploratory laparotomy were performed. Histopathologic examination of full-thickness biopsies from the gastrointestinal tract and liver revealed the presence of eosinophilic granulomatous lesions in the submucosa and tunica muscularis of stomach, jejunum, ileum, colon, and liver. infectious agents were not detected by light microscopic and electron microscopic examination or by immunohistochemistry. On the basis of the findings, it is concluded that the disease in this dog represents an unusual manifestation of chronic idiopathic inflammatory bowel disease.
Keywords
Granulomatous inflammatory lesions of the gastrointestinal tract in dogs can have noninfectious causes (e.g., food starch, foreign bodies, nonsteroidal anti-inflammatory drugs, tissue trauma, immune-mediated diseases) or can result from chronic infections. 6 Possible infectious agents include bacteria or fungal organisms (e.g., Mycobacterium sp., Campylobacter sp., Pythium insidiosum, Lagenidium giganteum, Prototheca sp., and Histoplasma sp.). 5, 6, 8 Furthermore, parasites such as migrating larvae of Toxocara canis (visceral larva migrans) can be a cause of granulomatous lesions in the gastrointestinal tract and other organs of dogs. 7 Rarely, granulomatous inflammatory lesions, with or without eosinophils and of undetermined etiology, can occur in the small intestine, large bowel, or both of dogs, which are classified as belonging to the group of idiopathic inflammatory bowel diseases. 6 Only rare case reports are available about idiopathic granulomas, which are dominated by eosinophilic granulocytes and have been observed in the esophagus, stomach, and small and large intestine of dogs of various breeds. 4, 6, 9, 12
A 1-year-old male Siberian Husky presented with a history of diarrhea, lethargy, and anorexia of several months' duration. At clinical examination, the dog had a decreased cardiac rate. On abdominal radiographs, an enlarged liver was observed, and on computer tomography, the bile ducts appeared to be dilated and the liver had an inhomogeneous appearance. No enlarged mesenteric or hepatic lymph nodes were detected. The blood count revealed slight anemia (38% hematocrit, reference range 40–55%), marked leukocytosis (59 × 103 leukocytes/μl, reference range 6.0–12.0 × 103 leukocytes/μl), a decreased percentage of segmented neutrophilic granulocytes (26%, reference range 60–75%), 0% lymphocytes (reference range 15–30%), 74% eosinophils (reference range 0–6%), and moderate thrombocytopenia (111 × 103 platelets/μl, reference range 150–500 × 103 platelets/μl). Serum biochemistry showed abnormal values for liver enzymes (alanine aminotransferase 123 U/liter, reference range up to 50 U/liter; glutamate dehydrogenase 25.2 U/liter, reference rang: up to 6.0 U/liter), and total protein (9.29 g/dl, reference range for dogs over 1 year 6.0–7.0 g/dl). During the following 3 weeks after initial presentation of the patient, further blood counts revealed an increase of eosinophils up to a maximum of 87%, with a final decrease to 11%. Decrease of the percentages of eosinophils was accompanied by an increase of lymphocytes up to normal levels. Examination of feces for parasites was negative. On exploratory laparotomy, dilated bile ducts and coarse, yellow-white, granular hepatic foci were seen. The wall of the pylorus was thickened and had similar yellow-white foci like the liver. During laparotomy, full-thickness biopsies were obtained from the pyloric region of the stomach, duodenum, jejunum, ileum, and colon. Furthermore, a liver biopsy was taken. Formalin fixed samples were embedded in paraffin wax. Sections (5 μm) were stained with hematoxylin and eosin (HE), periodic acid–Schiff, Gram stain, cresyl echt violet, Ziehl–Neelsen, and Grocott's silver stain. Serial sections were subjected to immunohistochemistry with different primary antibodies against canine parvovirus, canine distemper virus, Neospora caninum, Toxoplasma gondii, Helicobacter pylori, and Mycoplasma pneumoniae (cross-reactions with different Mycoplasma spp.) and with the avidin–biotin complex–peroxidase method (ABC kit; Vector Laboratories, Burlingame, CA). For electron microscopic examination, HE-stained paraffin sections were deparaffinized and re-embedded into epoxy resin.
Histopathologic examination revealed the presence of palisading eosinophilic granulomas with flame figures, mostly located in the submucosa in sections from pylorus, jejunum, ileum, colon, and liver (Figs. 1–3). In sections from pylorus and jejunum, multiple granulomas were seen that were not only located in the submucosa but also extended into the tunica muscularis (Fig. 1), although in the section from the colon, only 1 large submucosal granuloma was found (Fig. 2). Granulomas consisted of variable-sized nodular areas with centrally located, densely eosinophilic material representing remnants of fragmented collagen bundles and degenerate eosinophils (flame figures; Fig. 2). Around necrotic centers of granulomas, numerous palisading macrophages and eosinophils were present (Fig. 3). Some macrophages resembled epithelioid cells, whereas others had a vacuolated or almost foamy cytoplasm. The surrounding submucosal tissue, especially in sections from the pylorus, showed marked fibrosis and many newly formed blood vessels and was markedly infiltrated with numerous diffusely distributed eosinophilic granulocytes intermingled with small numbers of lymphocytes, plasma cells, and neutrophils. Eosinophilic infiltrations were also seen in the muscular layers. Multinucleate giant cells were not found in any of the specimens examined. In the mucosa of sections with granulomatous lesions, a moderate to marked diffuse infiltration of the lamina propria of both the superficial and deeper mucosa with eosinophils was seen. In sections from the duodenum, granulomas were absent. There was, however, a mildly increased mucosal infiltration with eosinophilic granulocytes. In the liver parenchyma, multiple randomly distributed eosinophilic palisading granulomas resembling those seen in the tissue locations described above were found. In the surrounding hepatic parenchyma, numerous eosinophils were seen within sinusoids. Moderate periportal and mild interlobular fibrosis with moderate bile duct hyperplasia and infiltration of periportal areas with numerous eosinophils and few lymphocytes and neutrophils were found. Immunohistochemically, scattered immunopositive Helicobacter-like organisms were seen at the lumenal border of a few glands in the pyloric mucosa. Immunohistochemical staining of tissue sections for the above-named antigens was negative. No microorganisms were detected ultrastructurally in any of the different tissue samples.
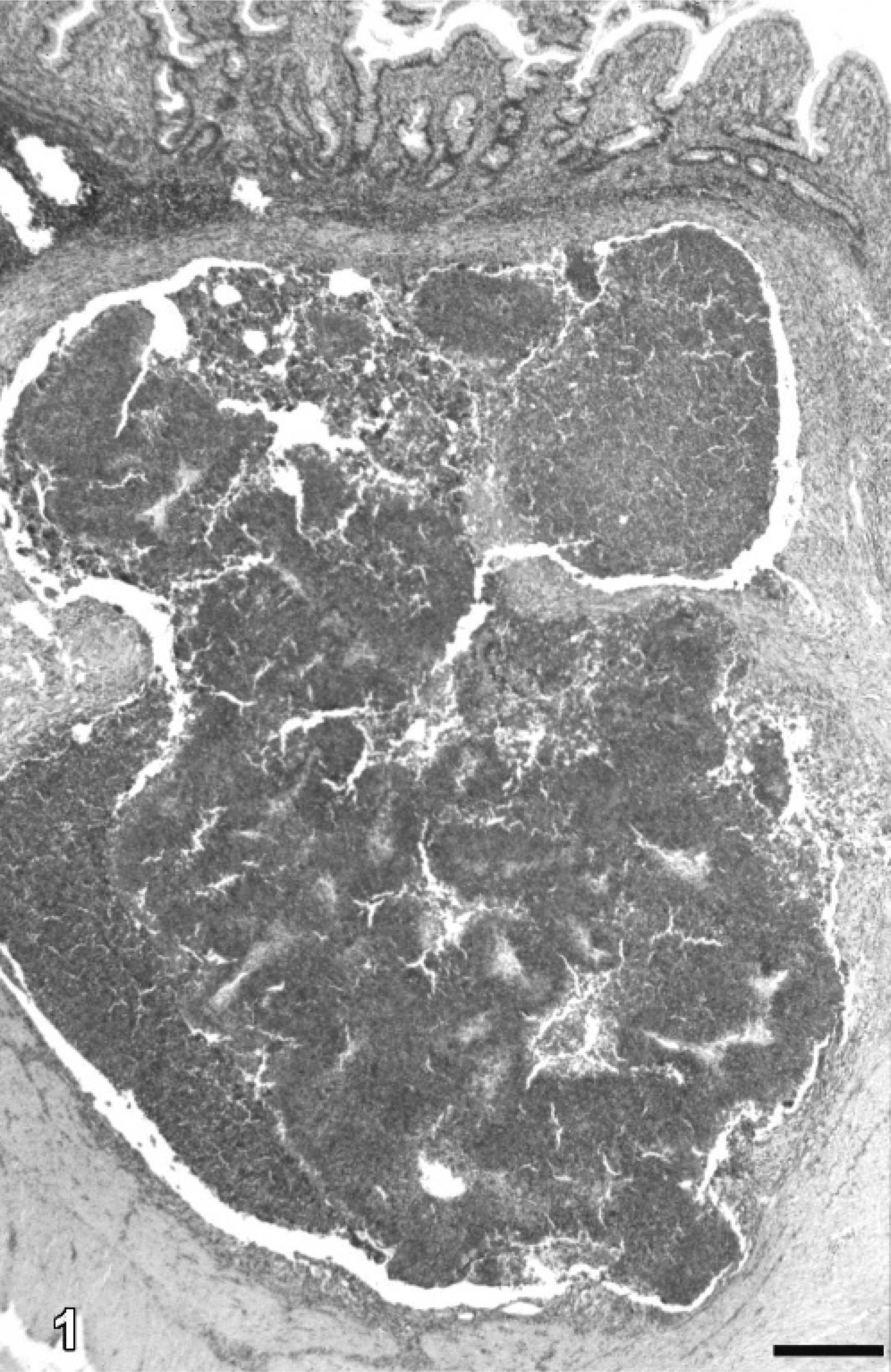
Small intestine; Siberian Husky. Full-thickness biopsy sample from the jejunum with multiple coalescing eosinophilic granulomas located in the submucosa and extending into the tunica muscularis. HE. Bar = 435 μm.
On request, the referring veterinary surgeon reported that the dog had been re-presented 6 times, beginning approximately 6 months after eosinophilic granulomatous organ lesions had been diagnosed. According to the referring surgeon's records, the dog had peripheral eosinophilia (22.4%), hematochezia, and diarrhea and was treated with antibiotics. Twenty-three months after histopathologic diagnosis of the disease, the dog was still alive. Further information about the outcome of the disease of this patient is not available.
In Siberian Huskies, eosinophilic granulomatous lesions have previously been described to occur in the skin, the oral cavity, and the eyelid but not in the gastrointestinal tract or the liver. 1, 2, 10, 11, 13, 14 Histomorphologically, the lesions seen in this dog closely resemble those described in the skin and in the oral mucosa of Siberian Huskies, supporting the opinion that Siberian Huskies are predisposed to develop eosinophilic granulomas. 2, 6, 10, 11, 13 Idiopathic granulomatous lesions are an uncommon finding in the gastrointestinal tract of dogs and can occur with or without an eosinophilic inflammatory component. 3, 4, 6, 9, 12 Differential diagnosis for granulomatous gastrointestinal lesions includes diseases from a variety of infectious agents. 6 Usually, the causative agents can be found in HE-stained sections or can be demonstrated by special stains or other methods, such as immunohistochemistry or electron microscopy. In our case, however, by applying such methods, no infectious agents were detected. In a short report, the occurrence of granulomatous colitis in a young Siberian Husky is described, which, in contrast to our case, did not have an eosinophilic inflammatory component and, because of radiographic findings and the presence of multinucleate giant cells, most likely represented a reaction to a foreign body. 3 Therefore, to the best of our knowledge, this is the first report of widespread noninfectious eosinophilic granulomatous lesions in the gastrointestinal tract, including the liver of a Siberian Husky. A parasitic cause seems to be unlikely in this Siberian Husky because no evidence of parasitic organisms was found histopathologically or by fecal examination. In this dog, a marked peripheral eosinophilia was present. In general, eosinophilia can be due to parasitic infestations, allergy, or eosinophilic granulomatous lesions, as in this dog. 6, 7, 9, 12 An initial 0 count of lymphocytes was due to the high percentages of eosinophils, later increasing to normal levels as the percentage of eosinophils decreased during following examinations. The possible pathogenesis of the lesions seen in our dog remains obscure. For canine eosinophilic granuloma, several pathogenetic mechanisms are under discussion, including vasculitis, microangiopathy, disorders of fibrinolysis or phagocytic function, and allergic reactions. In a case of canine eosinophilic granulomatous colitis in a 3-year-old female Bouvier des Flandres, fibrinous necrosis of the wall of submucosal blood vessels was described. 4 In our dog, no signs of vasculitic lesions were found. One could speculate that eosinophilic granulomatous lesions in Siberian Huskies might be an immune-mediated disease. So far, reports about immunologic investigations on possible allergic reactions in such dogs are not available. Therefore, it cannot be excluded that hypersensitivity reactions to yet unknown allergens could have been involved in the development of the disorder seen in this dog.
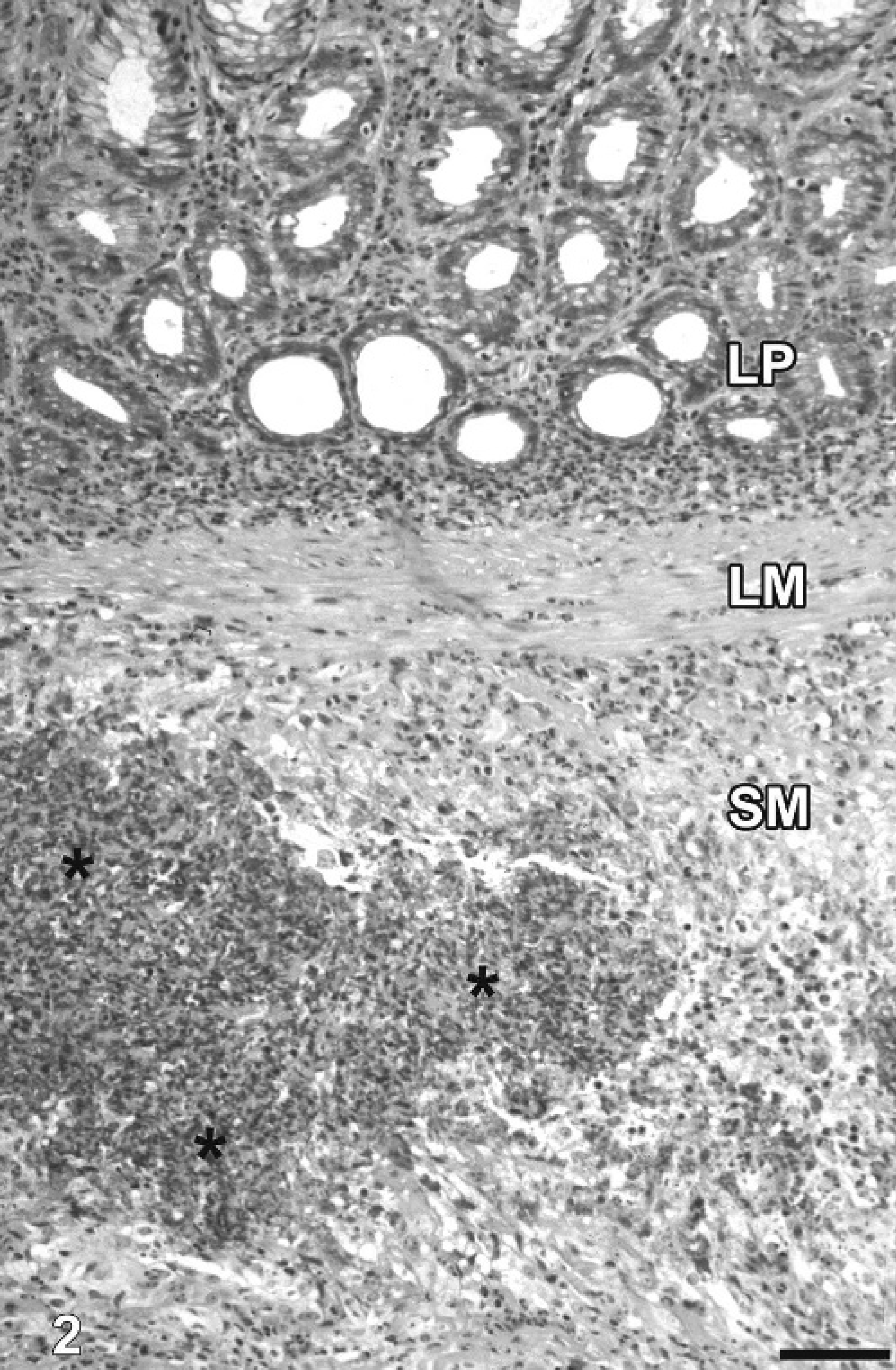
Large intestine; Siberian Husky. Section of full-thickness biopsy from the colon with submucosal eosinophilic granulomas (asterisks) consisting of centrally located, densely eosinophilic material representing remnants of fragmented collagen bundles and degenerate eosinophils (flame figures). LP = lamina propria; LM = lamina muscularis mucosae; SM = submucosa. HE. Bar = 55 μm.
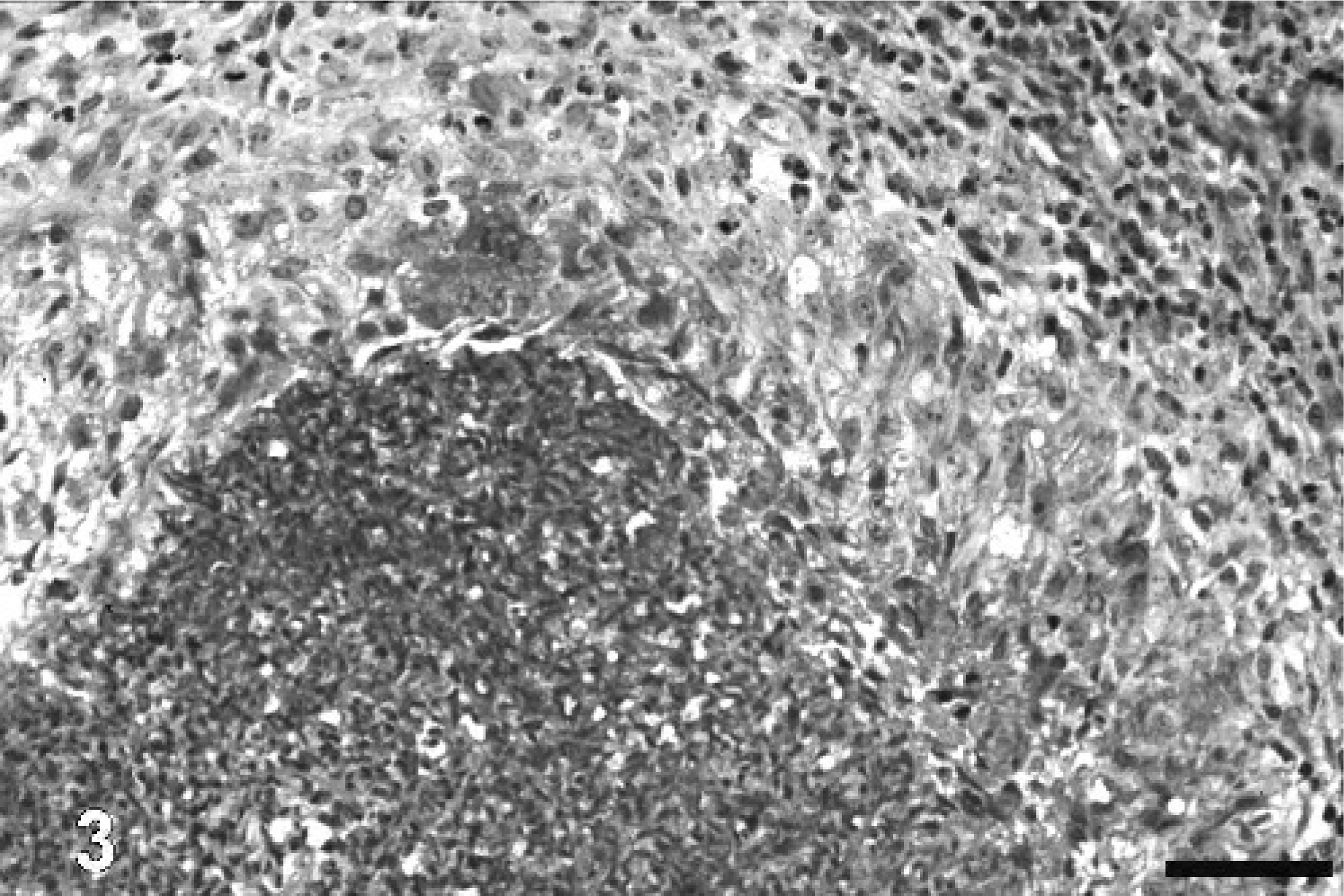
Large intestine; Siberian Husky. Eosinophilic granuloma with numerous palisading macrophages and eosinophils surrounding the necrotic center. HE. Bar = 28 μm.
Footnotes
Acknowledgements
We thank Mrs. P. Grünig, Mr. K.-P. Kuhlmann, and Mrs. K. Rohn for their excellent technical assistance.