
Abstract
A carcinoma ex pleomorphic adenoma was diagnosed in the left mandibular salivary gland of an 8-year-old female spayed dog. The animal presented with a large nonpainful swelling in the left submandibular region. A computed tomography scan detected an irregularly enhancing soft tissue mass that was closely associated with the left external ear canal and extended to the left wing of the atlas. On surgical exploration, the mass was intimately associated with the left mandibular salivary gland. Both the mass and the adjacent gland were removed, and the diagnosis was determined by histopathology. The tumor was comprised of basaloid and low columnar epithelial cells, many glandular units formed by well-differentiated sebocytes, and multifocal regions of necrosis, mineralization, and hemorrhage. Salivary gland tumors with sebaceous differentiation are very rare in animals, with one previously reported case in a cat.
An 8-year-old female spayed Basset Hound was presented to the University of Tennessee Veterinary Teaching Hospital because of a mass located in the left submandibular area. The mass was first noticed by the owners 2–3 months prior to presentation and was gradually increasing in size. The dog was otherwise healthy and exhibited no clinical signs associated with the mass. At presentation, the mass was subcutaneous, fixed, and firm on palpation. Fine needle aspirate of the mass revealed many streaming erythrocytes and nucleated cells, suggesting a mucinous background. The heterogeneous cell population consisted of a few large aggregates of well-differentiated salivary secretory epithelial cells and several large clusters of uniform, basophilic cells exhibiting a high nuclear-to-cytoplasmic ratio. The aspirate was considered to be of salivary gland origin; differentials for the mass included basal cell tumor or a well-differentiated ductular tumor.
A computed tomography (CT) scan showed a focal, well-circumscribed, heterogenous-density mass measuring approximately 44 (dorsoventral dimension) × 35 (mediolateral dimension) × 48 (rostrocaudal dimension) mm arising within the left mandibular salivary gland (Fig. 1). The mass was expansive within the gland, effacing the adjacent gland parenchyma. Postcontrast images revealed nonuniform enhancement of the mass with normal strong uniform enhancement of the adjacent compressed glandular tissue. There was mild enlargement of one of the adjacent submandibular lymph nodes. Imaging diagnosis was of a discrete mass arising within the left mandibular salivary gland with mild associated lymphadenomegaly. Primary consideration was given to a neoplastic process.

Postcontrast axial CT image at the level of the larynx. The dog is imaged in dorsal recumbency. A heterogeneously enhancing mass (spanned by vertical white line) is present within the left mandibular salivary gland (large arrowhead). The dorsal portion of the salivary gland (small arrowheads) is effaced by the expansion of the mass within the gland parenchyma. The right mandibular salivary gland (arrow) is normal. Bar = 1-cm increments.
Surgical excision of the mass and an enlarged left submandibular lymph node was performed. Grossly, the mass was intimately associated with the left mandibular salivary gland. The salivary gland itself, however, was compressed by the mass to the periphery and did not appear to be involved.
Four sections of the mass with adjacent salivary gland and two sections of the left submandibular lymph node were examined histologically (Figs. 2, 3, 4). Peripheral salivary gland tissue was compressed by an oval, well-demarcated, encapsulated, densely cellular multilobular mass, consisting of predominantly basaloid epithelial cells that occasionally invaded the capsule. They were arranged in narrow trabeculae, ducts, tubules, and solid sheets, supported by a moderate fibrous stroma. The basaloid cells had minimal eosinophilic cytoplasm and densely basophilic nuclei. Small areas were composed of cuboidal to low columnar cells occasionally forming acinar structures. These cells had small amounts of eosinophilic cytoplasm and basally located nuclei, with a stippled chromatin pattern and variably distinct nucleoli. There were infrequent clusters of spindle cells loosely spaced in a blue/gray, mucinous matrix, consistent with myoepithelial cells. Many glandular units formed by well-differentiated sebocytes were scattered throughout the mass, as is characteristic of sebaceous differentiation. These cells had abundant, clear, vacuolated cytoplasm and a small central hyperchromatic nucleolus. The overall mitotic index was 3–5 per 40× high-power field, with no mitotic activity or cellular atypia in the sebocytes. Occasional nests of squamous differentiation and keratinization were present but there was no cellular atypia within these areas. Small areas of the fibrous stroma had a glassy, hyalinized appearance.
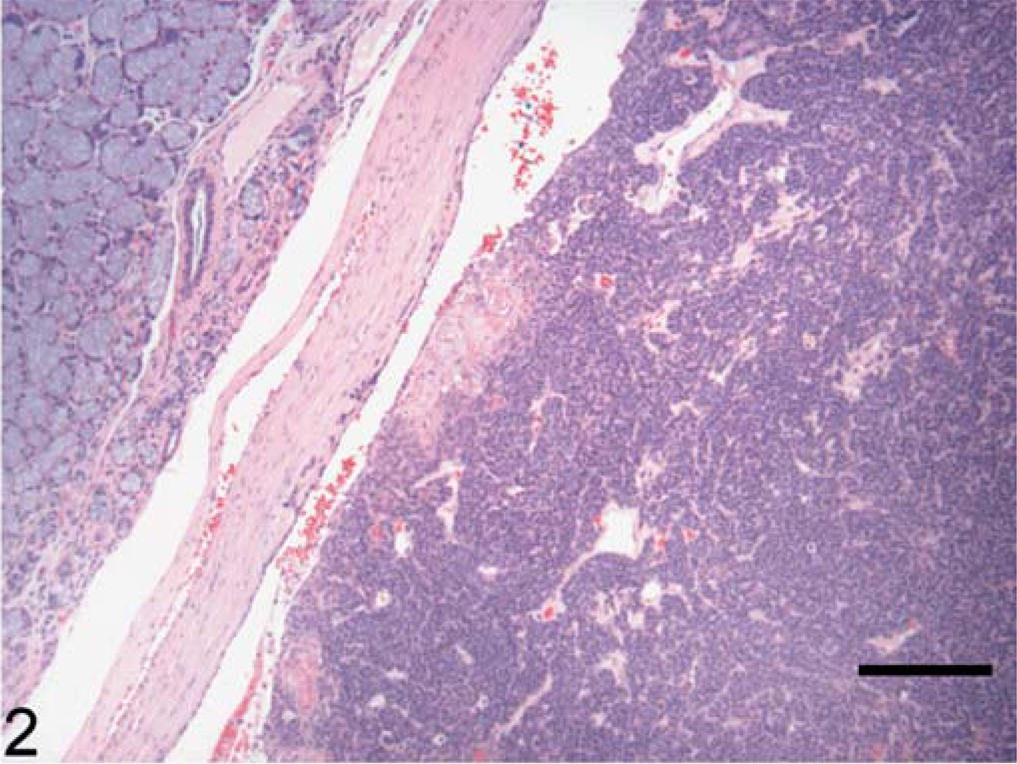
Carcinoma ex pleomorphic adenoma; dog. Border between the neoplasm and preexisting salivary tissue with intervening fibrous capsule. Within the neoplasm (right) there are foci of ductal and squamous differentiation. Hematoxylin and eosin. Bar = 200 µm.
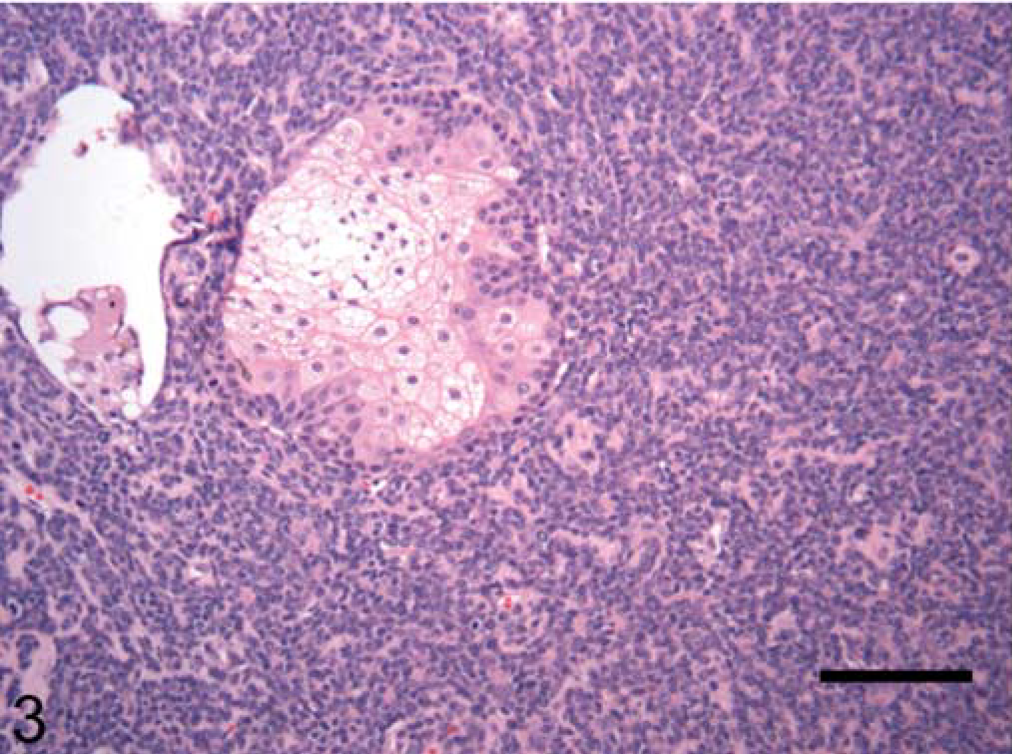
Carcinoma ex pleomorphic adenoma; dog. Within the neoplasm there is a cluster of well-differentiated sebocytes, consistent with sebaceous differentiation. Elsewhere, the pattern is more ductular. Hematoxylin and eosin. Bar = 100 µm.
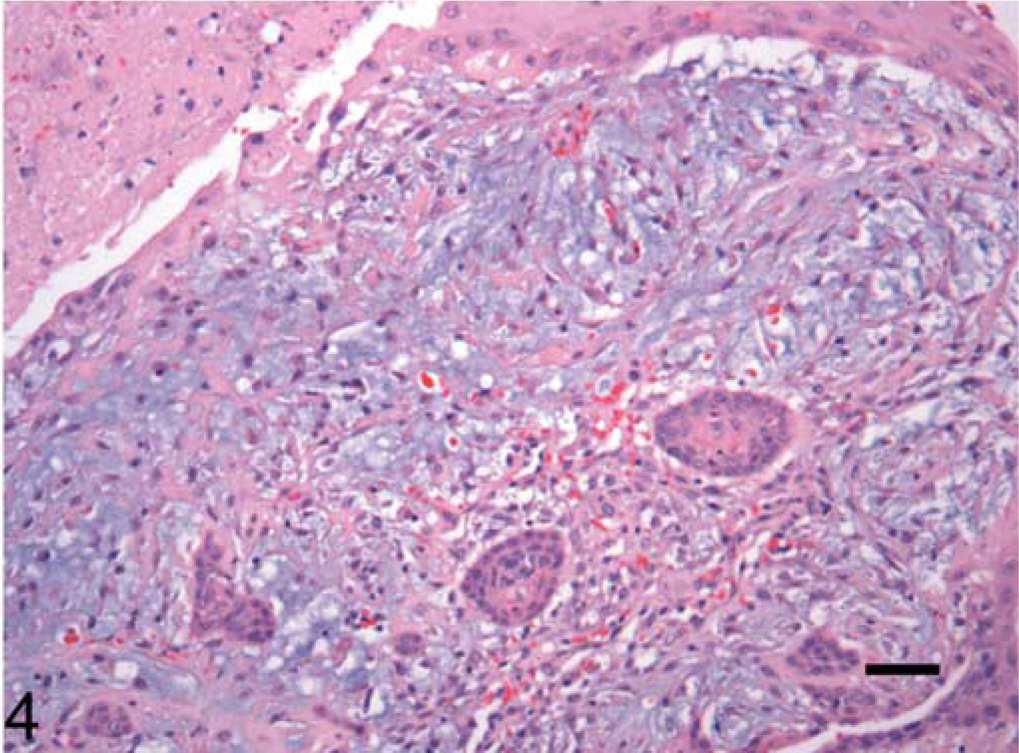
Carcinoma ex pleomorphic adenoma; dog. Cluster of myoepithelial cells within a mucinous stroma. These areas were infrequent, but this one is accompanied by islands of squamous cells. Necrosis is evident in the top left corner. Hematoxylin and eosin. Bar = 100 µm.
Neoplastic cells did not extend to the surgical margins. There were multifocal regions of necrosis, with mineralization, hemorrhage, and cholesterol clefts within the mass. In the interstitium of the preexisting salivary gland, there was a mild to moderate lymphoplasmacytic and neutrophilic infiltrate, and acini adjacent to the mass were atrophied. Final diagnosis was a carcinoma ex pleomorphic adenoma (carcinoma arising in a mixed tumor) with sebaceous differentiation.
The left submandibular lymph node contained numerous hemosiderin-laden macrophages, histiocytes, red blood cells and prominent lymphoid follicles with large germinal centers. The changes in the lymph node were consistent with reactive lymphoid hyperplasia.
Discussion
Canine salivary gland tumors are broadly classified into benign and malignant subtypes, with the vast majority of epithelial origin and malignant in appearance. 6 The mandibular gland is most commonly involved, with the parotid gland second in frequency. 4, 11 Salivary gland neoplasms are rare in dogs, with overall incidence of 1.6 benign tumors per 100,000 dogs at risk. For adenocarcinoma, the most common malignant salivary gland tumor, this figure was 3.1 per 100,000. 5, 6 Adenocarcinomas predominantly affect dogs between 10 and 12 years of age; there is no known breed or sex predilection for these tumors. 11 Treatment for canine salivary gland neoplasia centers mainly on surgical removal of the affected gland. Special attention is given to regional lymph nodes and lung as possible sites of metastasis, because 17% and 8% of dogs in one study had lymph node and distant metastasis, respectively. 4
The tumor described herein was most consistent with a carcinoma ex pleomorphic adenoma. The pleomorphic adenoma is the most common human salivary gland tumor, but it is rarely reported in dogs and cats. 5, 6, 12 Although uncommon, pleomorphic adenomas account for most reports of primary benign epithelial tumors arising from canine salivary glands. Most examples in the dog have been identified in the parotid gland. 5 The pleomorphic adenoma is described as containing a mixed population of epithelium, myoepithelium, and stroma, with no clear distinction between cell types. 6 Features that led to this diagnosis were the fairly uniform population of ductal epithelial cells, clusters of myoepithelial cells, and areas of squamous differentiation. The diagnosis of carcinoma was based on large areas of necrosis, local capsular invasion, and high mitotic index.
One of the most unusual aspects of this neoplasm was the fairly frequent sebaceous differentiation. In humans, sebaceous differentiation of parotid and mandibular glands is a normal finding, because sebaceous glands are present in the epithelium of the mouth and lining of the major ducts of salivary glands. 1 According to one study, approximately 10.5–42% of normal parotid and 6% of normal mandibular glands had such differentiation. 8 Degree of differentiation ranges from a single sebaceous cell to a completely developed sebaceous gland, and differentiation is most commonly found in periductal areas of interlobular ducts. The reason for such aberrant location of sebaceous glands is still under investigation. The two hypotheses, neither of which has been sufficiently proved, are developmental derivation from dermis and sebaceous metaplasia. It is not known whether the aberrant sebaceous glands give rise to sebaceous tumors. 8 However, sebaceous differentiation within salivary neoplasms seems to be considered less unusual in the human, where it is considered possible in any salivary neoplasm of ductal origin. 1 No comparative studies of normal canine salivary glands are available to provide analogous data for sebaceous differentiation in this species.
Primary sebaceous tumors of salivary gland origin are also rare. 7 In humans, these tumors are broadly classified into 4 groups: sebaceous adenoma, sebaceous lymphadenoma, sebaceous lymphadenocarcinoma, and sebaceous carcinoma/adenocarcinoma. 9 To date, the reports of salivary gland sebaceous adenoma come from the human literature, wherein sebaceous adenomas account for 0.1% of all salivary tumors. Sebaceous carcinomas are described as extremely rare. 2 The mean age of human patients with these tumors is 61.4 years. The tumor is usually described as a slowly growing, firm, nonpainful swelling. Most patients do not exhibit any symptoms at the time of presentation. Treatment of choice is a complete surgical excision. 3
The current case report describes a carcinoma ex pleomorphic adenoma in the salivary gland of a dog, a rare form of salivary neoplasia in this species. It also describes sebaceous differentiation within this tumor. This is a phenomenon that has not been previously reported in any canine salivary neoplasm, although a recent report describes a sebaceous carcinoma within the submandibular salivary gland of a cat. 10 We believe this tumor most likely originated within the left mandibular salivary gland, for two reasons. First, there was no apparent involvement of the skin on histopathology, and second, the tumor was almost circumferentially surrounded by salivary tissue. This patient also had no prior history of cutaneous sebaceous neoplasia as a potential source of a metastatic lesion.
The prognosis for carcinoma ex pleomorphic adenoma in humans is guarded; the prognosis is more difficult to predict in animals, given its rarity. However, clinical follow-up found this patient to be alive and free of disease 12 months after surgery.