
Abstract
A 2-year-old, spayed female, Labrador Retriever-cross presented with a subcutaneous mass of several weeks' duration in the right flank region. Surgical excision and histologic examination were performed. The 1.0-cm-diameter mass was circumscribed, unencapsulated, and cystic with a bilayer wall. The inner layer resembled intestinal mucosa, including a tall columnar lining epithelium, crypt-like glands containing scattered neuroendocrine cells that were strongly immunopositive for synaptophysin, and a supporting lamina propria-like fibrovascular tissue that contained lymphocytes and plasma cells. The outer layer was 1- to 2-mm thick and was composed of intersecting and blending bundles of smooth muscle and collagen. Given the presence of organized intestinal tissues in the subcutis, the lesion was consistent with intestinal choristoma.
Reports of heterotopic gastrointestinal tract tissue in animals are rare, and most commonly involve ectopic gastric or pancreatic tissue in the intestines (dog), esophagus (cat), and Meckel's diverticulum (pigs, horses). 2 In humans, congenital gastrointestinal tract mucosal heterotopias (choristomas) in the tongue, oral cavity, esophagus, small intestine, gallbladder, and most frequently, in Meckel's diverticulum have been reported. 1, 3 However, reports of subcutaneous gastrointestinal tract tissue are extremely rare and have all been associated with implantation after enterostomy or colostomy. 1 We describe a case of subcutaneous intestinal choristoma in a dog.
A 2-year-old, spayed female, Labrador Retriever-cross presented to the submitting veterinarian with a 1.0-cm-diameter, dark subcutaneous mass in the right flank region several weeks after initial observation. The mass was surgically excised and submitted for histologic examination. The submitted tissue was fixed in neutral-buffered 10% formalin and embedded in paraffin, then 5-µm-thick sections were cut and stained with hematoxylin and eosin (HE) for microscopic evaluation. To further characterize the mass, staining was performed with Mayer's mucicarmine, Masson's trichrome, and Verhoeff's elastin using standard methods, and immunostaining for reactivity with polyclonal antibodies against synaptophysin and α-smooth muscle actin (SMA) was done by use of the linked streptavidin-biotin (LSAB) complex method with commercial kits (Dako, Carpinteria, CA).
Histologically, the subcutaneous mass was circumscribed, unencapsulated, and cystic with a bilayer wall (Fig. 1). The inner layer resembled intestinal mucosa, with luminal tall columnar epithelium and scattered, crypt-like glands (Fig. 2) that were formed by cuboidal epithelial cells and fewer neuroendocrine-like polygonal cells that had moderate amounts of eosinophilic granular cytoplasm and large oval peripheralized nuclei (Fig. 3). The lining epithelium and glands were supported by small-to-moderate amounts of a lamina propria-like fibrovascular tissue that contained aggregates of lymphocytes and plasma cells. The outer layer was 1- to 2-mm thick and was composed of intersecting and blending bundles of smooth muscle and collagen.
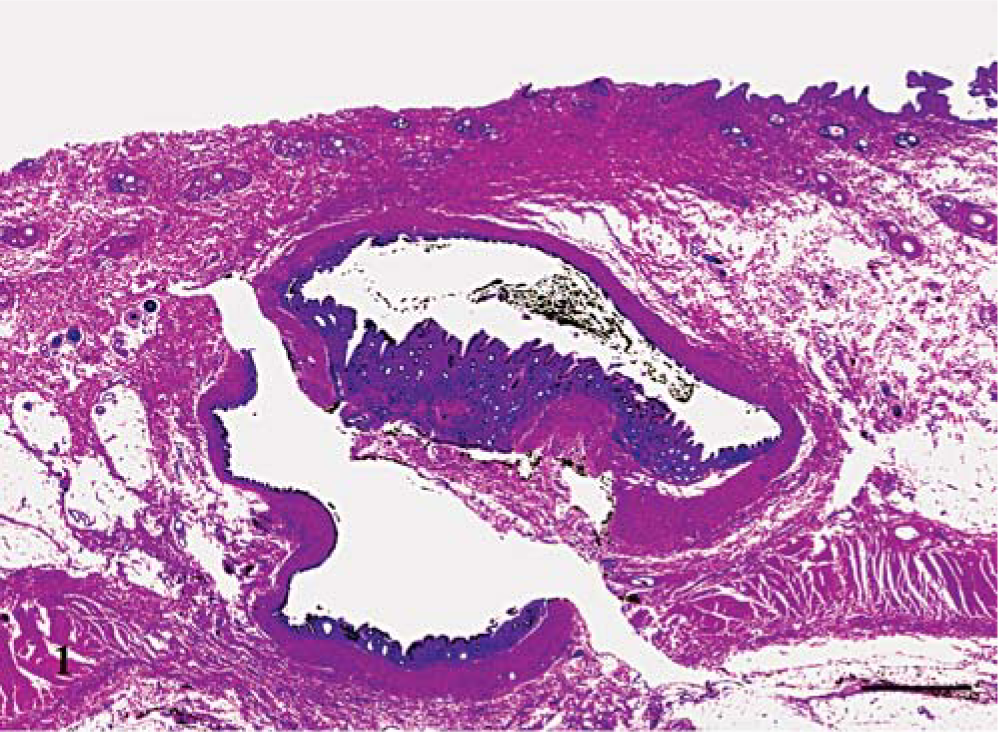
Haired skin; dog. An unencapsulated, circumscribed, bilayered, cystic mass expands the subcutis. Notice the section is fragmented, and there is a sagittal section of the inner wall of the collapsed cyst centrally. HE. Bar = 1 mm.
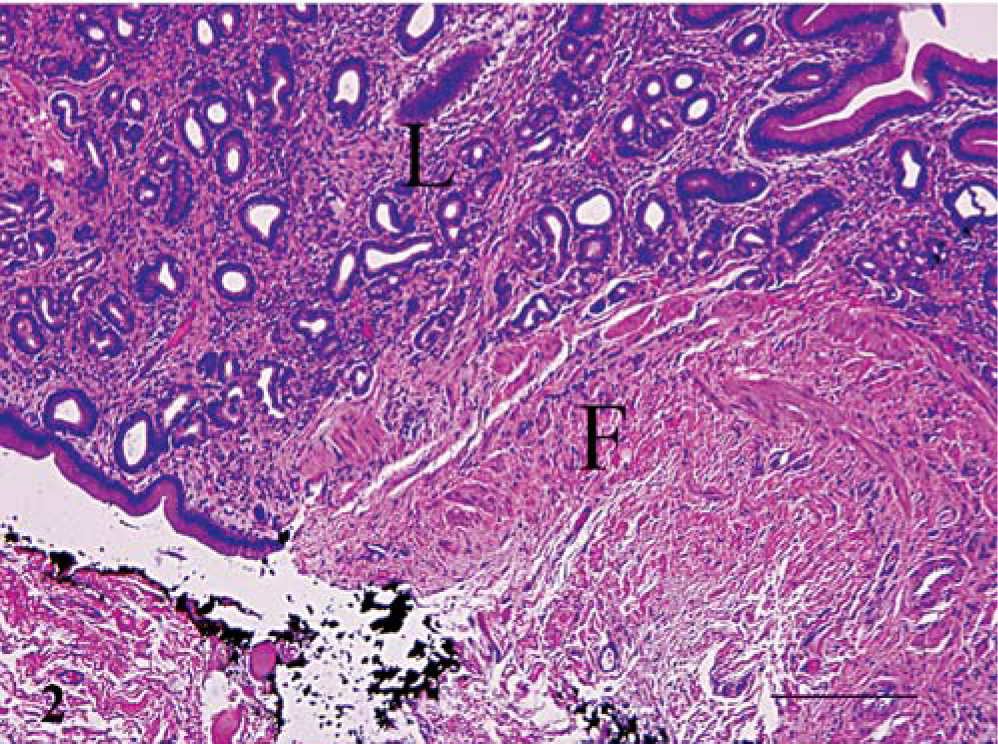
Subcutis; dog. The lining layer (L) consists of tall columnar, intestinal mucosa-like epithelium and crypt-like glands supported by lamina propria-like fibrovascular tissue with aggregates of lymphocytes and plasma cells bounded by a layer of fibromuscular tissue (F). HE. Bar = 200 µm.
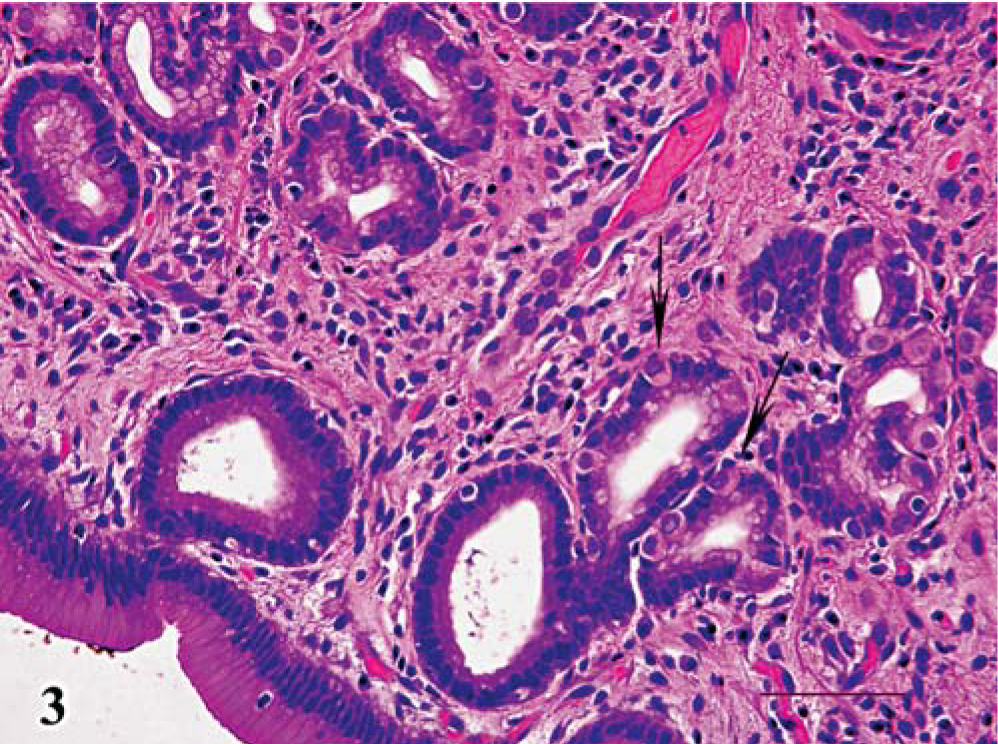
Subcutis; dog. Crypts include polygonal cells with moderate amounts of eosinophilic granular cytoplasm and large oval basal nuclei (arrows). HE. Bar = 100 µm.
The composition of the tissue nodule was better defined by results of histochemical and immunohistochemical procedures. The presence of collagen and smooth muscle bundles in the outer layer was confirmed by blue and red staining, respectively, using Masson's trichrome method. Many of the spindled cells in the outer layer also exhibited strong cytoplasmic immunopositivity for SMA. Similar to that of normal intestine, concentric bands of subepithelial elastin fibers were evident using Verhoeff's elastin method. The presumed neuroendocrine origin of the polygonal crypt cells was supported by strong cytoplasmic immunopositivity for synaptophysin. Although mucus cell differentiation was not evident using HE staining, there was rare luminal epithelial cell mucicarmine positivity.
The differential diagnosis for this nodular lesion of well-organized intestinal tissue within the subcutis of the flank includes congenital choristoma (congenital rest) and traumatic or surgical implantation. The dog had belonged to the same family since it was 8 weeks old, and there was no history of trauma or herniation. The only surgical procedure performed prior to the biopsy was a routine midline abdominal approach ovariohysterectomy. Also, within the peripheral tissue, there was lack of inflammation and reactive fibrosis, suggesting that the intestinal tissue had not been traumatically or accidentally surgically transplanted to the site. Therefore, we favor the diagnosis of congenital subcutaneous intestinal choristoma, and believe this to be the first report of this entity in any nonhuman species.