
Abstract
A neonatal foal was presented with a 6.5-cm pedunculated mass arising from the upper deciduous incisors. The distal end was soft and covered by haired skin, whereas the proximal end was firm, covered with mucosal epithelium, and at the point of transection contained a fully developed tooth. Microscopically, the mass was covered by epidermis and mucosal epithelium and the remaining portion of the mass consisted of mature collagen, nonneoplastic fat and smooth muscle, and a single tooth within a bony socket. The mass is consistent with an oral choristoma and has features similar to those described for hairy polyp in humans.
Keywords
In humans, hairy polyps are uncommon, nonneoplastic growths that most often arise from the oronasopharynx. They are derived from the mesoderm and ectoderm and usually form a pedunculated mass diagnosed shortly after birth. 1–7,9 A choristoma is a mass of normal tissue in a location where it is not normally found. 4,6,7,9 In this study, we report a case from a neonatal foal of an oral choristoma that closely resembles a hairy polyp described in humans.
At birth, a neonatal female foal was presented with a pedunculated mass arising from the area of the upper deciduous incisors. The mass interfered with suckling and was surgically removed at its base, fixed in 10% formalin, and submitted for investigation.
Grossly, the mass was tubular, 6.5 cm long, and varied in thickness. At the proximal base, the mass was 2.9 cm, narrowed to 2.5 cm, and then gradually enlarged to 3.5 cm at the distal end. The mass was covered by a white to beige mucous membrane except for the most distal portion that consisted of a 2.5-cm-diameter patch of epidermis with thick, short, velvety hair (Fig. 1). The proximal one third of the mass was extremely firm, whereas the distal two thirds was soft and fluctuant. On cut section, the proximal portion of the mass contained a fully developed tooth with a calcified socket (Fig. 2).
Oral mass; foal. Pedunculated mass covered by mucosal epithelium and, on the distal end, haired skin.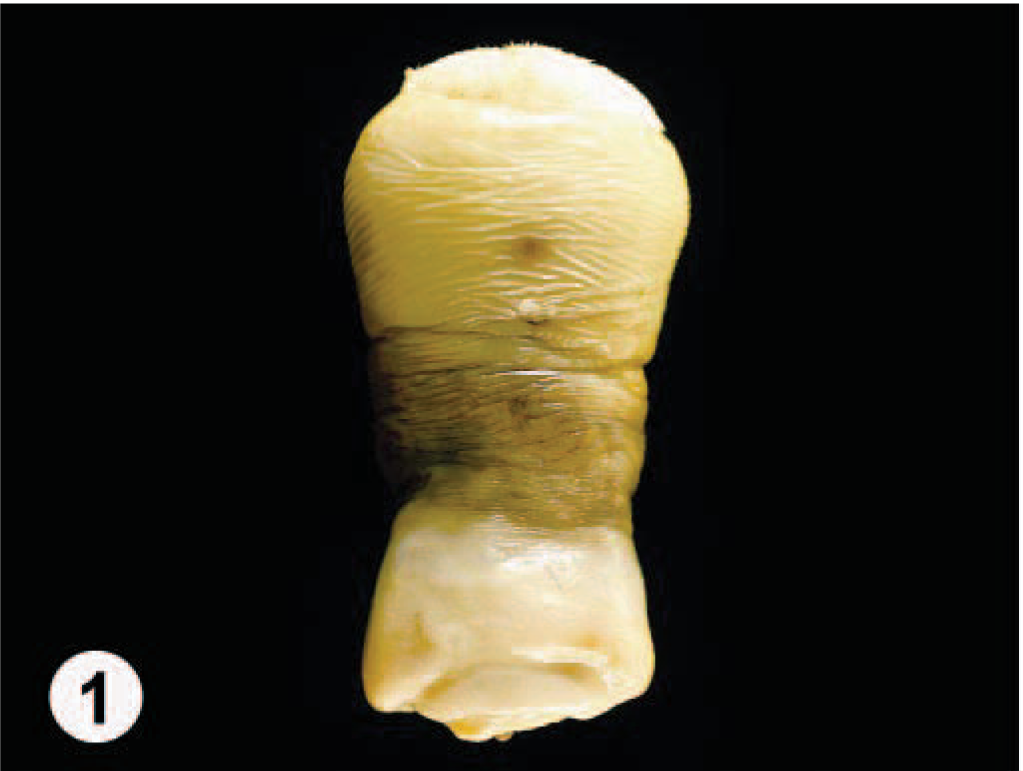
Oral mass; foal. A proximal section of the mass at the point of transection. Note the developing tooth within a bony socket.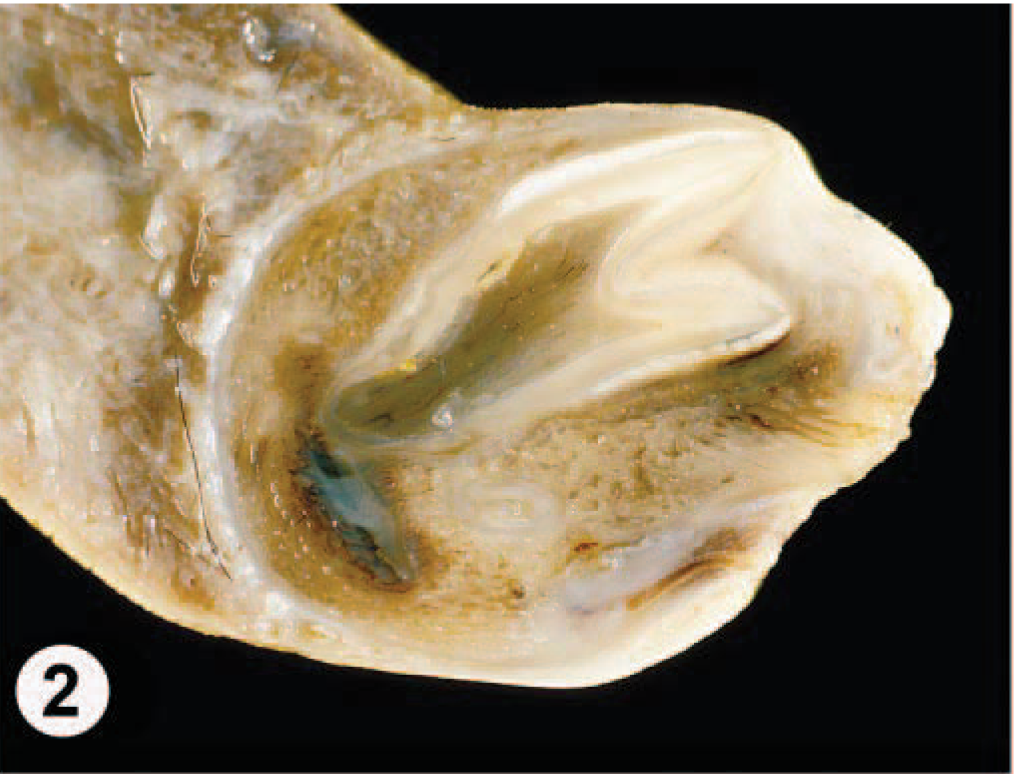
Histologically, the distal end of the mass contained an epidermis consisting of keratinizing, stratified squamous epithelium, sebaceous glands, and hair follicles. The epidermis made an abrupt transition to thick mucosal epithelium with prominent rete ridge formation that covered the remainder of the mass. The stroma consisted of abundant collagen, fat, smooth muscle, and blood vessels (Fig. 3). Multifocally, the proximal half of the mucosa was ulcerated and infiltrated by many neutrophils and fewer lymphocytes that extended well into the underlying stroma. The most proximal portion contained a fully developed tooth anchored in a socket of alveolar bone (Fig. 4). Radiographs of the upper dental arcade revealed a complete intact dentition. Therefore, the tooth within the mass was diagnosed as supernumerary.
Oral mass; foal. A section of surface epithelium and underlying stroma. Note the abrupt transition from a thick mucosal epithelium to haired skin and epidermis. HE. Bar = 200 µm.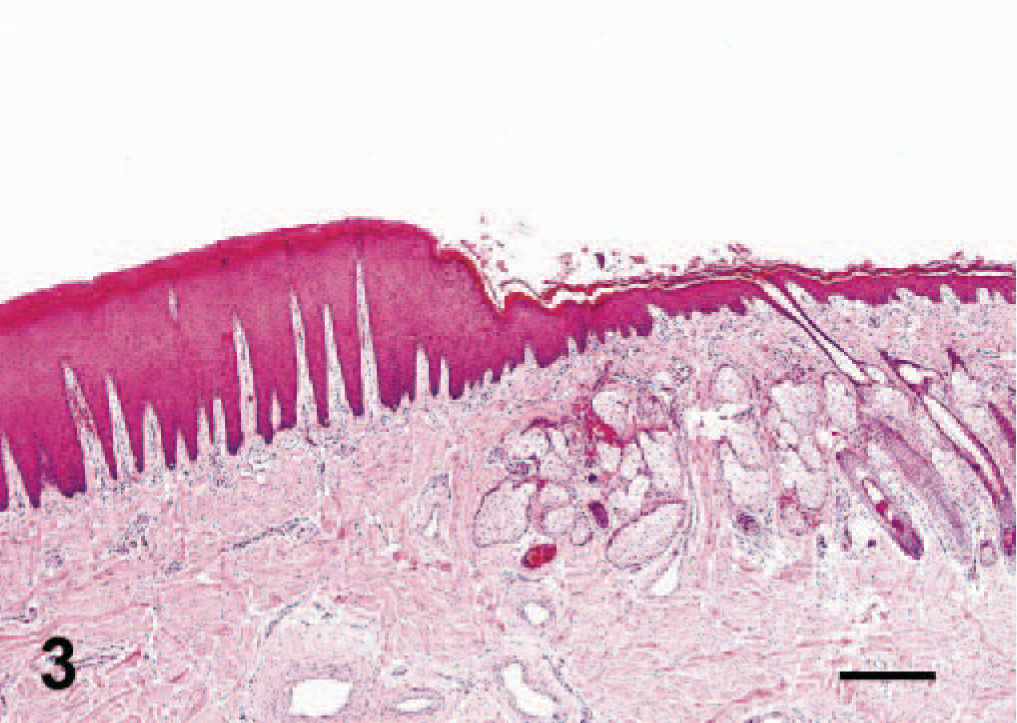
Oral mass; foal. The proximal section of the mass contains a fully developed tooth (T) within a bony socket (S). Arrows indicate mucosal epithelium. Azan stain. Bar = 2.5 mm.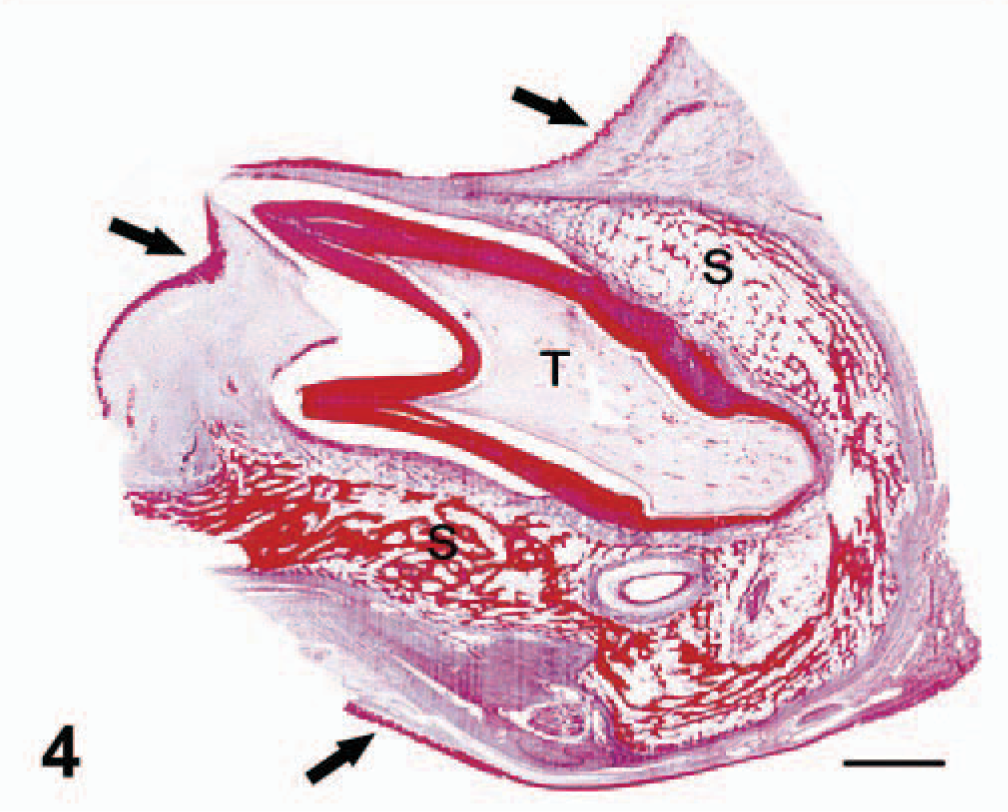
There have been over 137 cases of hairy polyp reported in humans, most arising from the oronasopharynx. 1 They are typically diagnosed at birth as a pedunculated mass that interferes with breathing or suckling. Hairy polyps are reported six times more commonly in females than males. 1,2,4,7 There may be an association with other congenital abnormalities such as ankyloglossia, cleft palate, absence of the uvula, abnormal facial development, atresia of the carotid artery, and osteoporosis. 6,7,9 However, they are not associated with a particular syndrome, 6 and there is no genetic predisposition. 4,6 Typically, they form an elongated mass ranging in size from 0.5 to 6.0 cm. 6,7 Microscopically, they consist of a core of fibroadipose stroma that contains cartilage, bone, muscle, and salivary glands covered by stratified squamous epithelium and hair follicles. 1,4,6,7 Treatment consists of surgical excision. There has been no documented case of metastasis and only one documented case of local recurrence. 4,7
There is considerable confusion in the literature regarding the classification of hairy polyps. They have been described as teratomas, hamartomas, dermoids, and choristomas. 1–7,9 Traditionally, a teratoma is a neoplastic lesion consisting of cells from all three germ layers: mesoderm, ectoderm, and endoderm. More recently, however, teratoma has come to mean a mass that consists of any two of the three germ cell layers. Some authors feel an important distinction between hairy polyps and teratomas is that the former are nonneoplastic and have only limited growth potential, whereas the latter are neoplastic and have the potential to metastasize. 3,7 Hamartomas are also nonneoplastic but by definition a hamartoma consists of tissue types that are characteristic of that location. The presence of haired skin, bone, and muscle in a mass arising from oral mucosa precludes a hairy polyp from being classified as a hamartoma.
Dermoids, similar to hairy polyps, consist of two germ layers: mesoderm and ectoderm. This similarity has led some authors to designate hairy polyps as dermoids. 6 However, dermoids are usually cystic and because hairy polyps consist of a solid stroma, recent authors have classified hairy polyps as choristomas. 3,4,7,9
The pedunculated mass arising from the oral cavity in this foal is best classified as a choristoma. Histologically, the mass consisted of well-differentiated, nonneoplastic cells, excluding its classification as a teratoma, which is a true neoplasm. The use of the term dermoid, although technically not incorrect because this mass consists of both mesoderm and ectoderm, is potentially confusing. In veterinary medicine, the term dermoid usually connotes a choristomatous lesion of the eye 8 or cystic lesions found in the subcutis, especially in Rhodesian Ridgeback dogs. 10 Use of the term dermoid is better left for these more specific situations. Finally, hamartoma is not appropriate because the mass consisted of haired skin, smooth muscle, bone, and a tooth, none of which arise from the oral mucosa. Therefore, this mass is most accurately diagnosed as a choristoma resembling hairy polyp in humans.
Footnotes
T. J. Steinbach is a Major and M. G. Mense is a Lieutenant Colonel in the US Army. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Army or the Department of Defense.