
Abstract
Nodular thyroid hyperplasia was found in a 4-year-old male cynomolgus monkey (Macaca fascicularis). The monkey was clinically normal; however, necropsy revealed multiple variably sized nodules in both lobes of the thyroid gland. In contrast to the fairly uniform diameter of the lumen of follicles in the surrounding gland, the diameter of the follicular lumen within the hyperplastic nodules was highly variable and ranged from nonexistent to cystlike. Occasionally, in the larger follicles there were papillary infoldings of epithelium. The hyperplastic nodules were partially encapsulated by a fibrous capsule and showed little compression of the surrounding tissue. The follicular cells and colloid comprising the hyperplastic nodule were immunohistochemically positively stained with the antibody for thyroglobulin. Ultrastructurally, the cells forming follicles had numerous microvilli along the luminal surface, and lysosomal bodies and dilated rough endoplasmic reticulum in the cytoplasm. All these morphologic findings are consistent with nodular thyroid hyperplasia, which is rare in nonhuman primates.
Nodular thyroid hyperplasia is characterized by formation of nonneoplastic nodules in the thyroid and has been reported in humans, horses, cats, dogs, and the rhesus monkey (Macaca mulatta). 1–4 In the two cases reported in the rhesus monkey, thyroid nodular hyperplasia was associated with clinical laboratory findings of hyper- or hypothyroidism, as frequently is the case in humans. Based on the sparcity of reports of thyroid nodular hyperplasia in nonhuman primates, the finding is considered rare. This communication describes a case of nodular thyroid hyperplasia of unknown etiology found in a cynomolgus monkey.
The animal was a facility-born, 4-year-old male cynomolgus monkey (Macaca fascicularis) that was used in a short-term toxicity study for a candidate drug. Based on the very short period of drug exposure (28 days) and the lack of thyroid gland changes in the other dosed monkeys, the nodular thyroid hyperplasia was not considered to be associated with drug administration. The monkey was fed a specified amount of pelleted diet (PS, Oriental Yeast Co., Ltd. Tokyo, Japan) and had free access to city water. Physical appearance, body weight, hematology, and blood chemistry had been periodically monitored since birth, including the study period; however, no abnormalities had been found. The monkey was euthanatized by exsanguination under ketamine and xylazine combined anesthesia and necropsied. Representative tissue samples were fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned at 2 µm, and stained with hematoxylin and eosin (HE) using standard procedures. The thyroid tissue was also stained immunohistochemically for thyroglobulin (rabbit polyclonal antibody, DAKO Japan Co., Kyoto, Japan) and calcitonin (rabbit polyclonal antibody, DAKO Japan Co.) using the labeled streptavidin–biotin method (LSAB™ kit, DAKO Japan Co.). For electron microscopic examination, small pieces of the thyroid tissue were postfixed in 4% glutaraldehyde and 2% osmium tetroxide solution, processed to epoxy resin–embedded ultrathin sections, and stained with uranyl acetate and lead citrate.
At necropsy the thyroid glands were bilaterally enlarged, and each lobe had two grossly visible nodules 3–10 mm in diameter (Fig. 1). The body weight at necropsy was 4.8 kg, and the combined thyroid weight was 1.12 g, the latter being approximately three times the values obtained from weight- and age-matched monkeys.
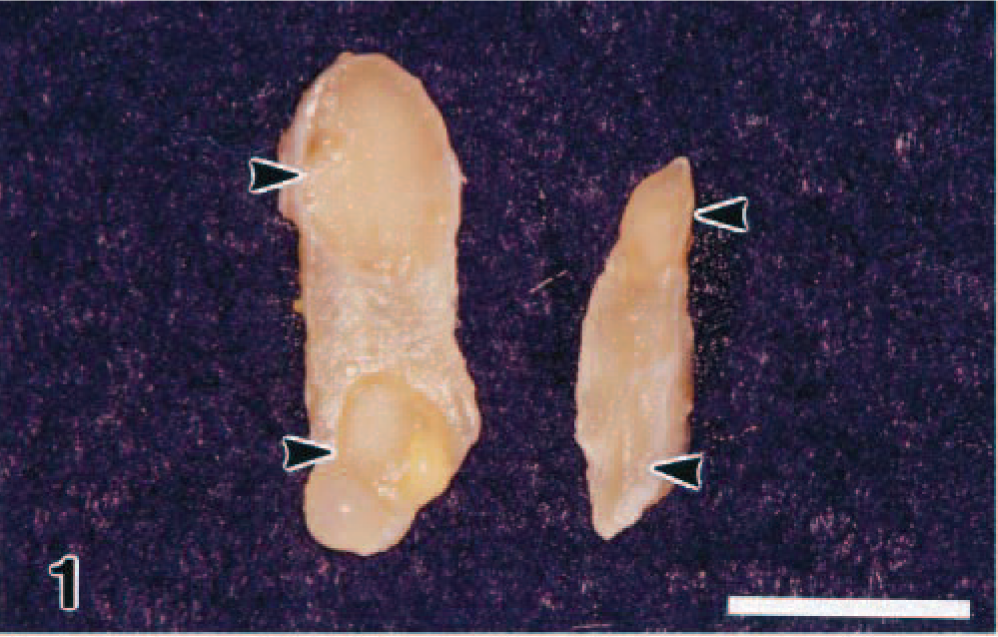
Thyroid gland, cut surface; monkey. Two nodules (arrowheads) are present in each lobe. Bar = 1 cm.
In contrast to most cynomolgus monkeys where the diameter of the lumen of the follicles generally shows uniformity, in this monkey the follicular lumens within the nodules showed marked disparity in size, ranging from nearly nonexistent to moderately cystically dilated (Figs. 2–4). Sometimes, the nodules were partially encapsulated by fibrous connective tissue (Fig. 3). Compression to the adjacent thyroid tissues, however, was rarely seen. Papillary projection into the follicular lumen was occasionally present in large follicles, and in contrast, the hyperplastic cells simulated solid-form arrangement when follicles were small or collapsed. There was no evidence of invasion, and mitotic figures were not evident.
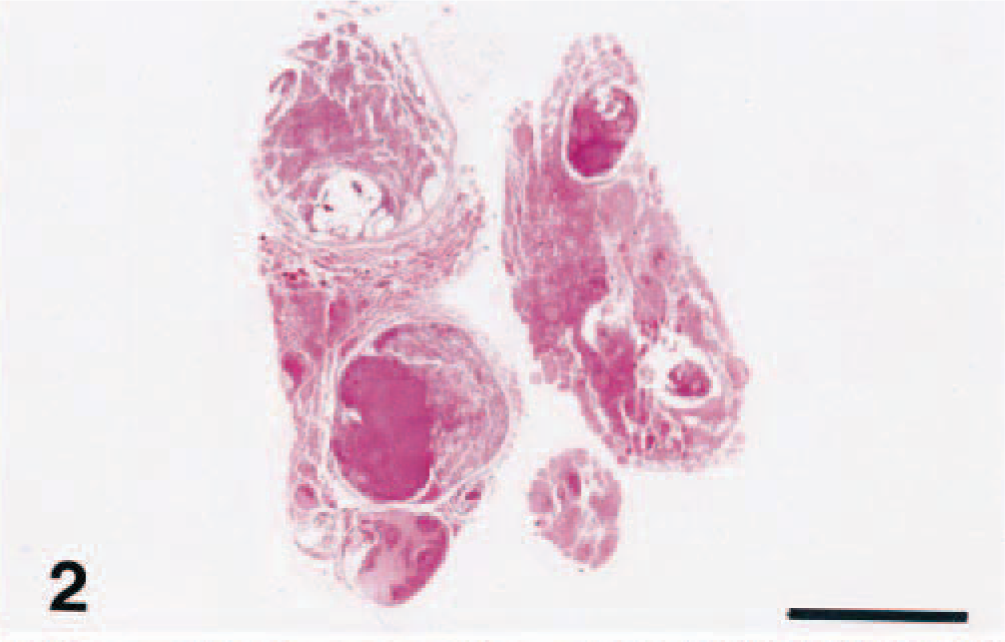
Thyroid gland; monkey. Both lobes have several nodules of various sizes. HE. Bar = 0.5 cm.
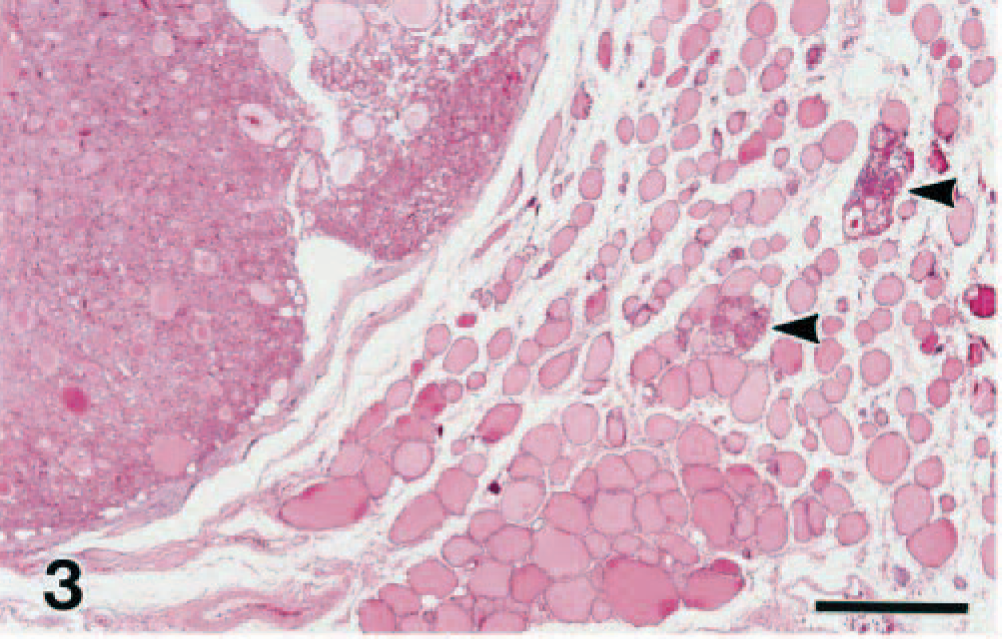
Thyroid gland; monkey. A large nodule at the left and two small lesions (arrowheads) are present. The large nodule is encapsulated with fibrous tissue and shows little compression to the adjacent thyroid gland. HE. Bar = 500 µm.
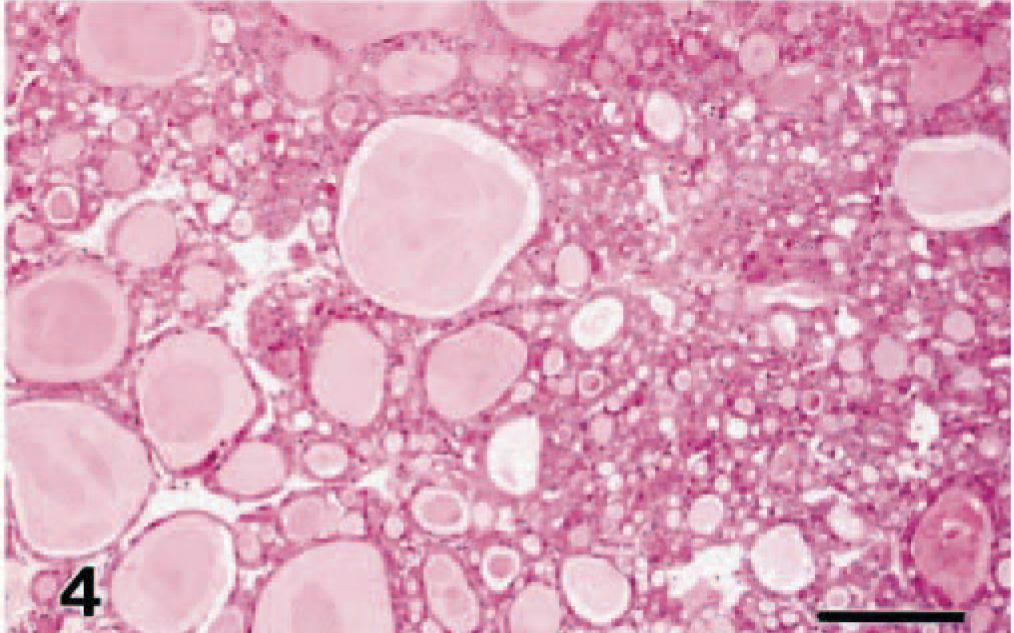
Thyroid gland; monkey. The thyroid epithelial cells in the nodules form follicles of various sizes. The cytoplasm is eosinophilic and granular. HE. Bar = 200 µm.
The hyperplastic cells were cuboidal to columnar, with one nucleus. The cytoplasm was eosinophilic and granular where occasionally intensely eosinophilic droplet and needle-shaped crystals were observed. The lumen of the follicles contained eosinophilic colloid. Both hyperplastic epithelial cells and colloid were stained positively with antibody for thyroglobulin (Fig. 5), whereas there was no staining for calcitonin. The follicular epithelium in the surrounding nonnodular tissue was low cuboidal in height.
Ultrastructurally, the cells in the hyperplastic nodules had microvilli along the luminal surface, and lysosomal bodies and dilated rough endoplasmic reticulum in the cytoplasm (Fig. 6). The ultrastructural features of the epithelium in the surrounding follicles were characterized by the following difference from those within the hyperplastic nodules.
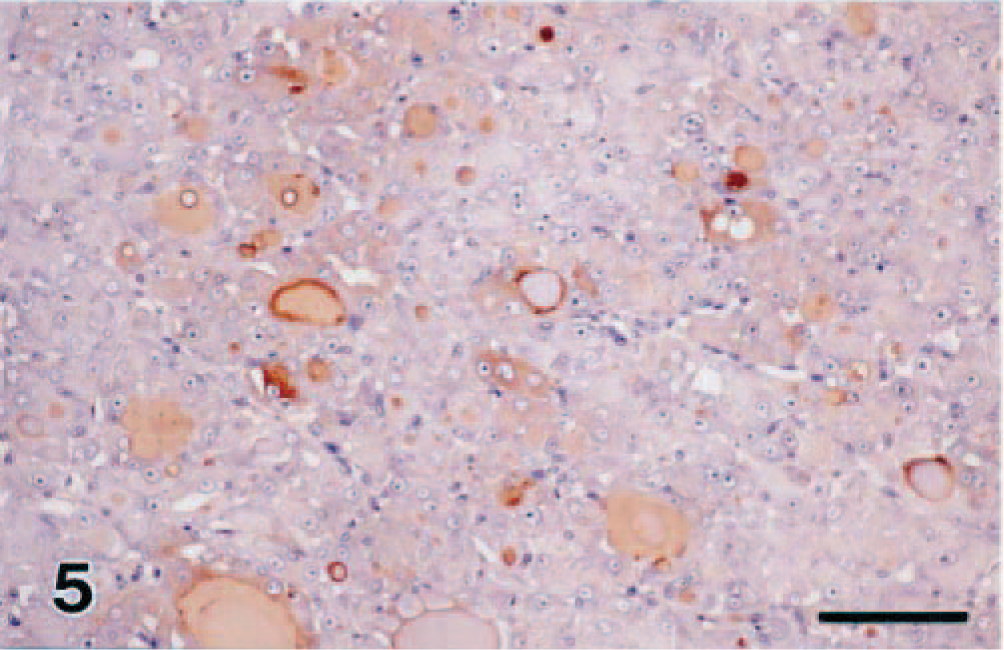
Thyroid gland; monkey. The thyroid epithelial cells and colloid are positive with antithyroglobulin. Immunohistochemistry. Bar = 100 µm.
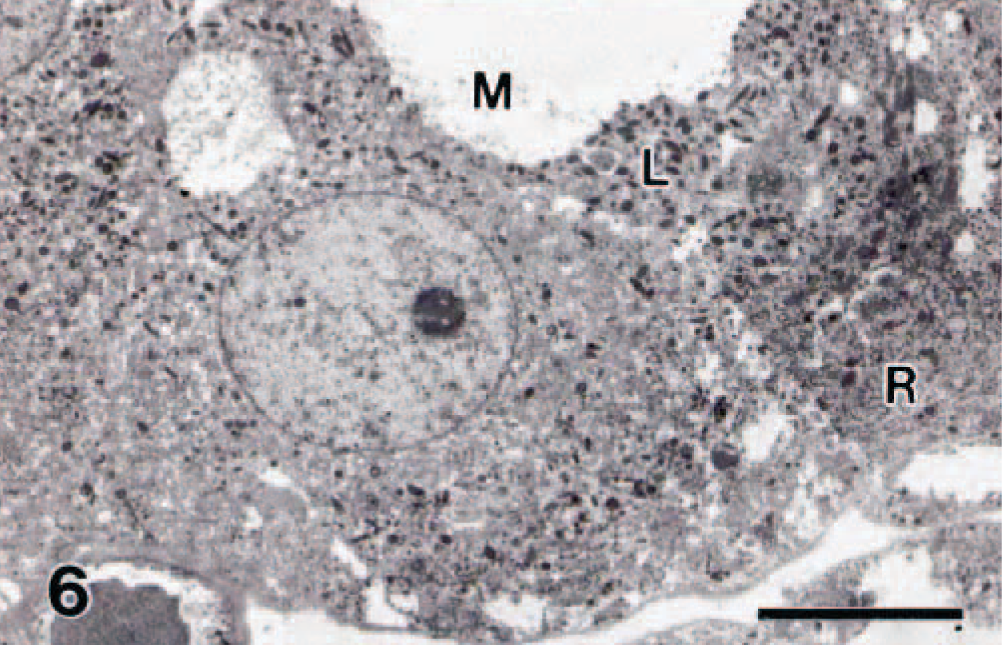
Thyroid gland; monkey. The cells are arranged in a follicular form. Noted are microvilli (M) along the luminal surface, and lysosomal bodies (L) and dilated rough endoplasmic reticulum (R) in the cytoplasm. Bar = 5 µm.
All these gross and histologic features are consistent with those for nodular hyperplasia described in humans as well as in animal species. Nodular thyroid hyperplasia is characterized by formation of multiple nodules that are composed of hyperplastic follicles. In domestic animals multinodular goiter and adenomatous goiter are both applied interchangeably to nodular thyroid hyperplasia, 2,3 and in humans synonyms for nodular hyperplasia further extend to nodular goiter, adenomatoid goiter, and adenomatous hyperplasia. 5 As these terms imply, it is sometimes difficult to differentiate nodular thyroid hyperplasia from follicular cell adenoma solely on the basis of morphologic findings. As a general rule, hyperplastic nodules are multiple, partially, or not at all encapsulated and variable in histologic appearance and arrangement; show comparable growth patterns with the adjacent normal tissue; and do not compress the surrounding parenchyma. Adenomas, in contrast, tend to be solitary, well encapsulated, and fairly uniform in histologic appearance and arrangement and show independent growth patterns from the adjacent normal tissue and compression against the surrounding parenchyma.
In humans nodular thyroid hyperplasia is the one most commonly found in a region where endemic iodine deficiency is seen. 5 Nodular thyroid hyperplasia in animals is often clinically endocrinologically quiescent and is thus found as an incidental lesion that appears to be the result of alternating periods of hyperplasia and colloid involution in the thyroid glands. 2,3 However, the true nature of nodular hyperplasia has not yet been fully elucidated. As for rhesus monkeys, the first case was reported to be associated with congenital hypothyroidism 4 and the second case to result in hyperthyroidism. 1 In the present case iodine deficiency is most unlikely to be involved because the animal was fed a commercial diet that was also given to other monkeys showing no histologic evidence of goiter. Whatever the underlying causes, it seemed that the nodular thyroid hyperplasia found in the present case maintained the normal functional state of the thyroid based on the normal growth curve and physical signs.
Footnotes
Acknowledgements
We gratefully acknowledge the technical assistance of Dr. T. Koujitani and Ms. I. Mise and review of the manuscript by Dr. K. Tanaka.