
Abstract
Variants of lipoma are uncommon, although fibrolipoma and infiltrative lipoma have been well documented. This report describes two cases of rare angiolipoma in dogs and the first documentation of angiofibrolipoma and infiltrating angiolipoma in a cat and a dog, respectively. Tumors were solitary, and most were located on the thorax of middle-aged patients. Angiolipomas were composed of mature adipose tissue mixed with variable numbers of blood vessels. In addition to the adipose and vascular components, the angiofibrolipoma contained bundles of collagenous connective tissue. The infiltrative angiolipoma had a primary mass external to the muscle and was histologically similar to a mixed intramuscular hemangioma that was confined to the muscle. Both disrupted bundles of striated muscle and were associated with segmental degeneration and loss of myofibers.
Benign cutaneous neoplasms of adipose tissue occur in all species. Simple lipomas are common in dogs. Fibrolipoma and infiltrating lipoma are uncommon variants that have been reported in dogs and cats.6–8 Angiolipoma has been described in dogs.8 In humans, there are additional variants of lipoma and infiltrating lipoma.4,5,10 Here we describe three of those variants: angiolipoma (case Nos. 1 and 4), angiofibrolipoma (case No. 2), and infiltrating angiolipoma (case No. 5). A mixed intramuscular hemangioma that was initially diagnosed as an infiltrative angiolipoma is included for comparison (case No. 3). The signalment, lesion location, and tumor size are presented in Table 1.
Signalment, lesion location, and tumor size.∗
DSH = domestic short hair; C Bay Ret = Chesapeake Bay Retriever; BTC = Black and Tan Coonhound; MC = male castrated; F = female; M = male.
Angiolipomas were solitary subcutaneous nodules composed of thin-walled blood vessels randomly distributed throughout lobules of well-differentiated adipose tissue (Fig. 1). Endothelial cells lined the vessels. Many vessels were dilated and filled with erythrocytes, and some vessels were branched. Fibrin clots were occasionally present in vascular spaces. No mitotic figures or atypical cells were observed. The patient in case No. 1 developed lymphosarcoma 1 year after tumor removal and was euthanized 18 months later. A necropsy was not performed. Routine physical examinations revealed no recurrence of the angiolipoma. The surgical incision in case No. 4 healed normally, and the dog was tumor free and in excellent health 14 months after tumor removal.
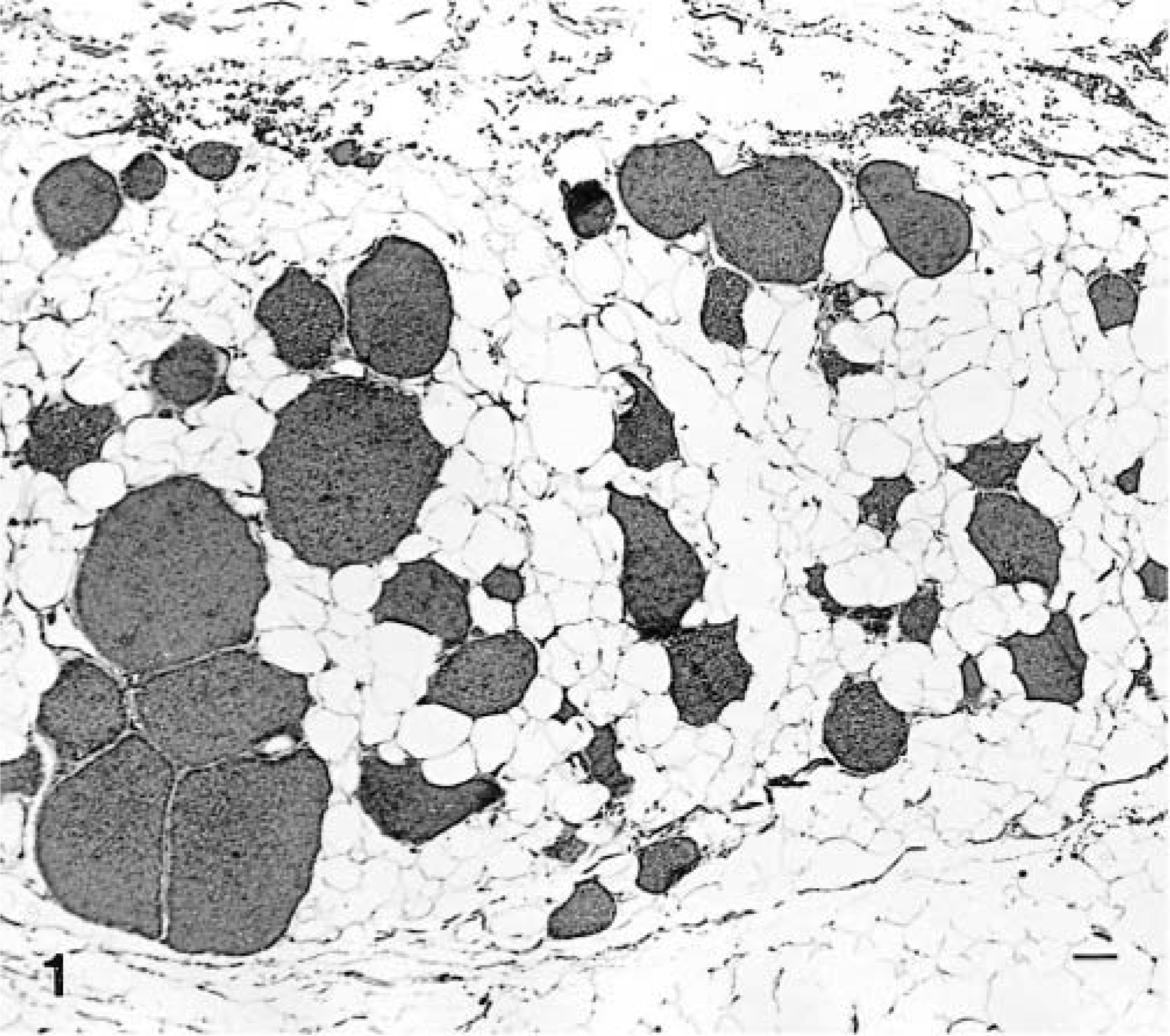
Angiolipoma; dog; case No. 1. The tumor is composed of lobules of mature adipocytes admixed with blood vessels. HE. Bar = 200 μm.
Angiofibrolipoma, a variant of fibrolipoma, was diagnosed in case No. 2. The nodule was located in the subcutis beneath the panniculus carnosus muscle. In addition to adipose and vascular tissue, this tumor also contained bands of collagenous connective tissue (Fig. 2) with low to moderate cellularity. The bands stained blue by the Masson's trichrome method, indicating that they were composed of collagen. A hematoma and suture-associated granuloma developed at the site and were surgically excised. The cat is in good health 29 months after surgery.
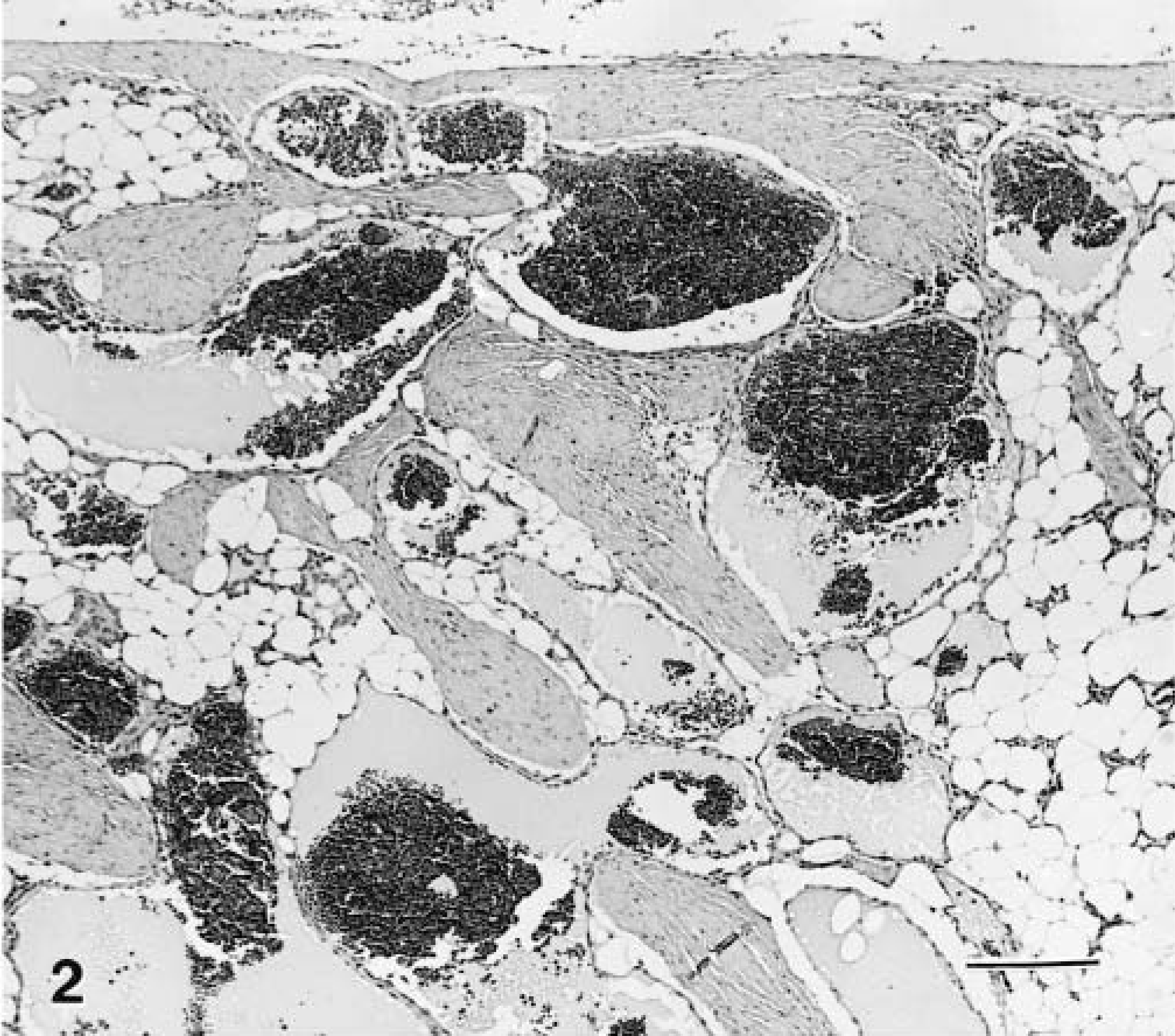
Angiofibrolipoma; cat; case No. 2. The tumor is composed of lobules of mature adipocytes, blood vessels, and bundles of collagen. HE. Bar = 200 μm.
In case No. 3, the mixed intramuscular hemangioma was initially diagnosed as an infiltrating angiolipoma. The tumor was unencapsulated and involved the superficial muscles of the thorax. It was composed of mature adipose and vascular tissues that were proliferating within bundles of striated muscle (Fig. 3). In one bundle, the tumor was composed entirely of vascular tissue (Fig. 4). Muscle fibers were invaded with segmental replacement by adipocytes and small vessels (Fig. 5). Confinement to the muscle was the rationale for the change of diagnosis. The surgical site healed without complication and the dog was in good health 9 months after surgery. The patient has been lost to follow-up due to death of the owner.
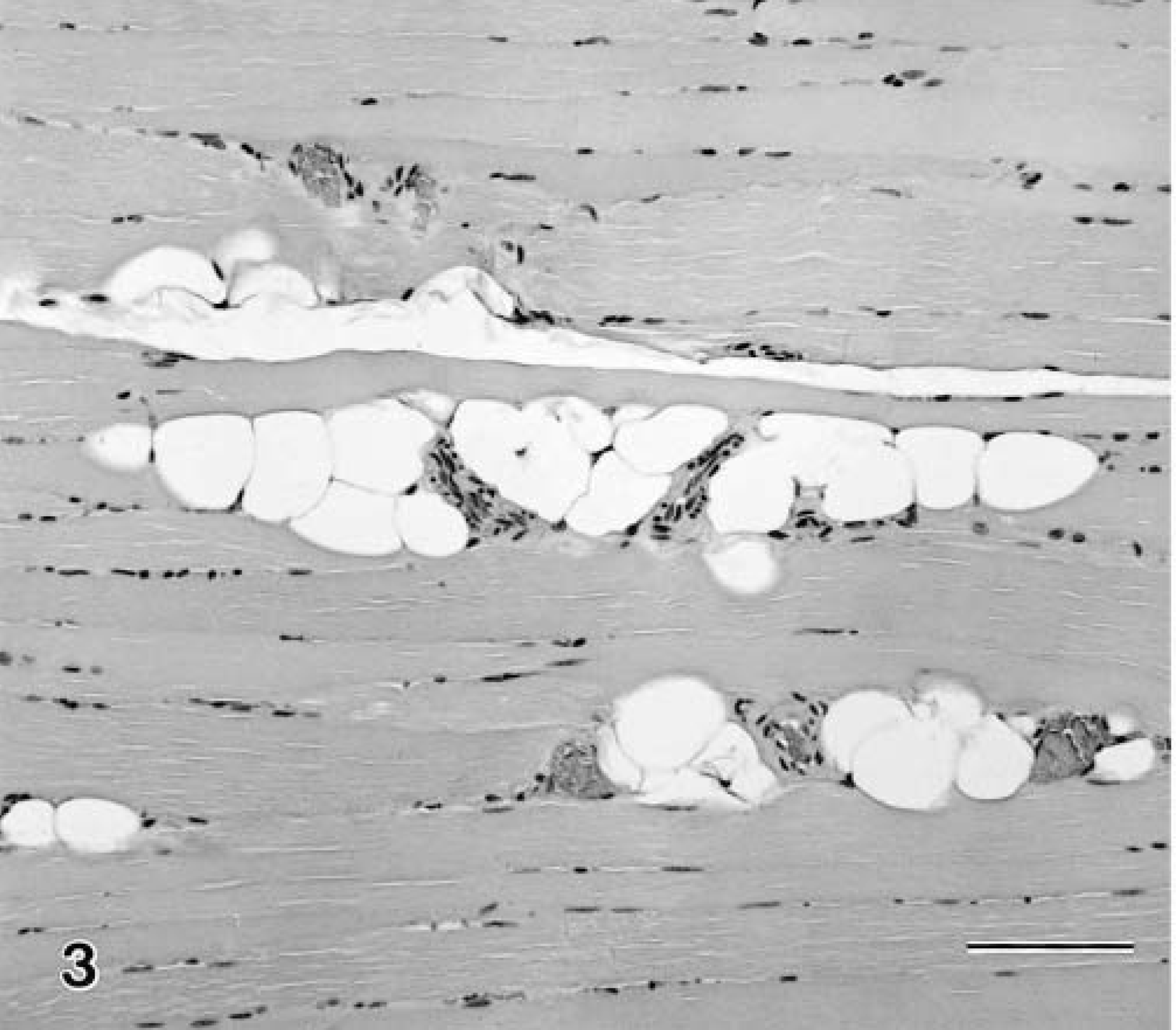
Mixed intramuscular hemangioma; dog; case No. 3. Blood vessels and mature adipocytes are infiltrating the muscle bundles. HE. Bar = 100 μm.
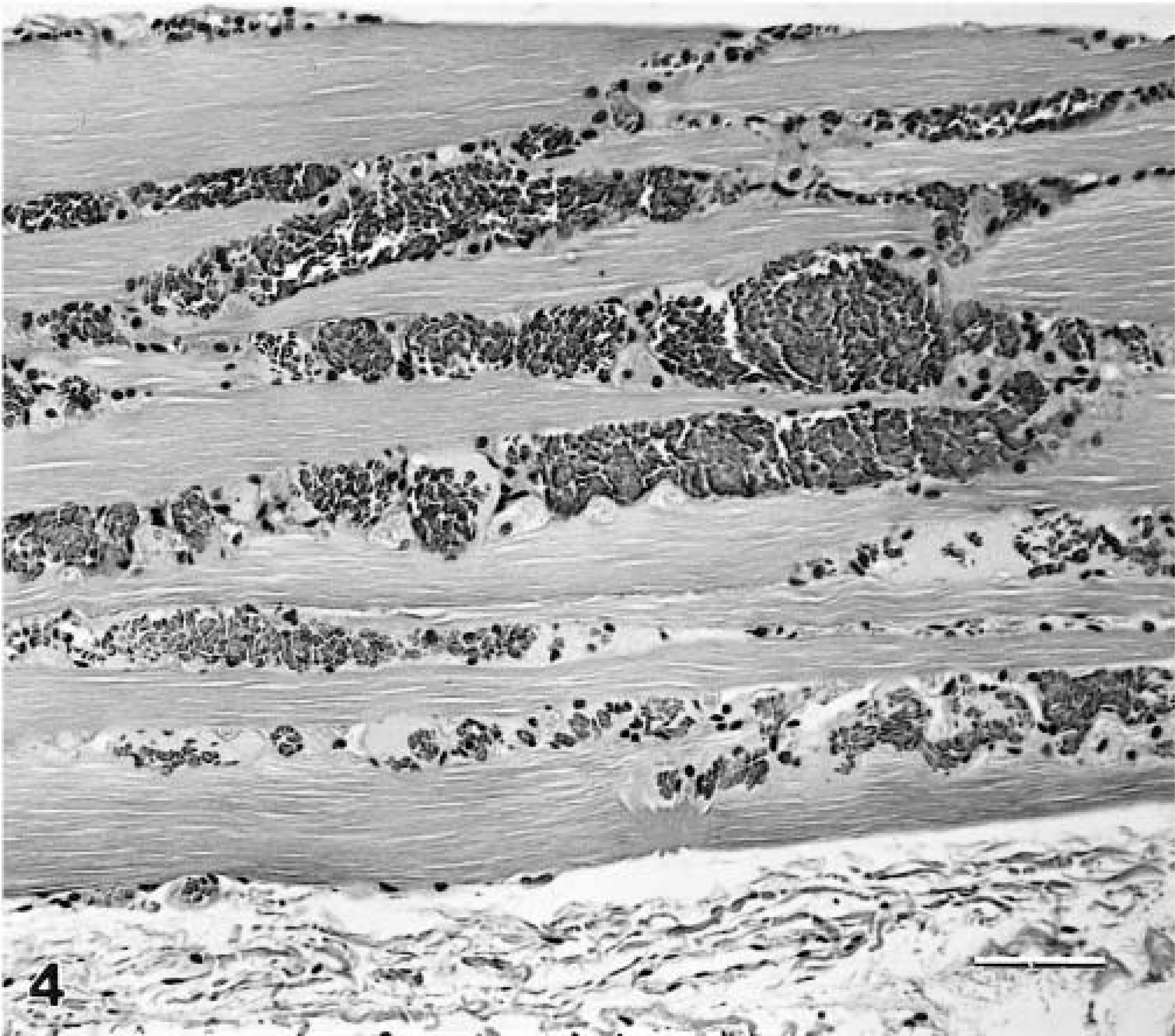
Mixed intramuscular hemangioma; dog; case No. 3. In this muscle bundle, the tumor is composed of infiltrating blood vessels. HE. Bar = 100 μm.
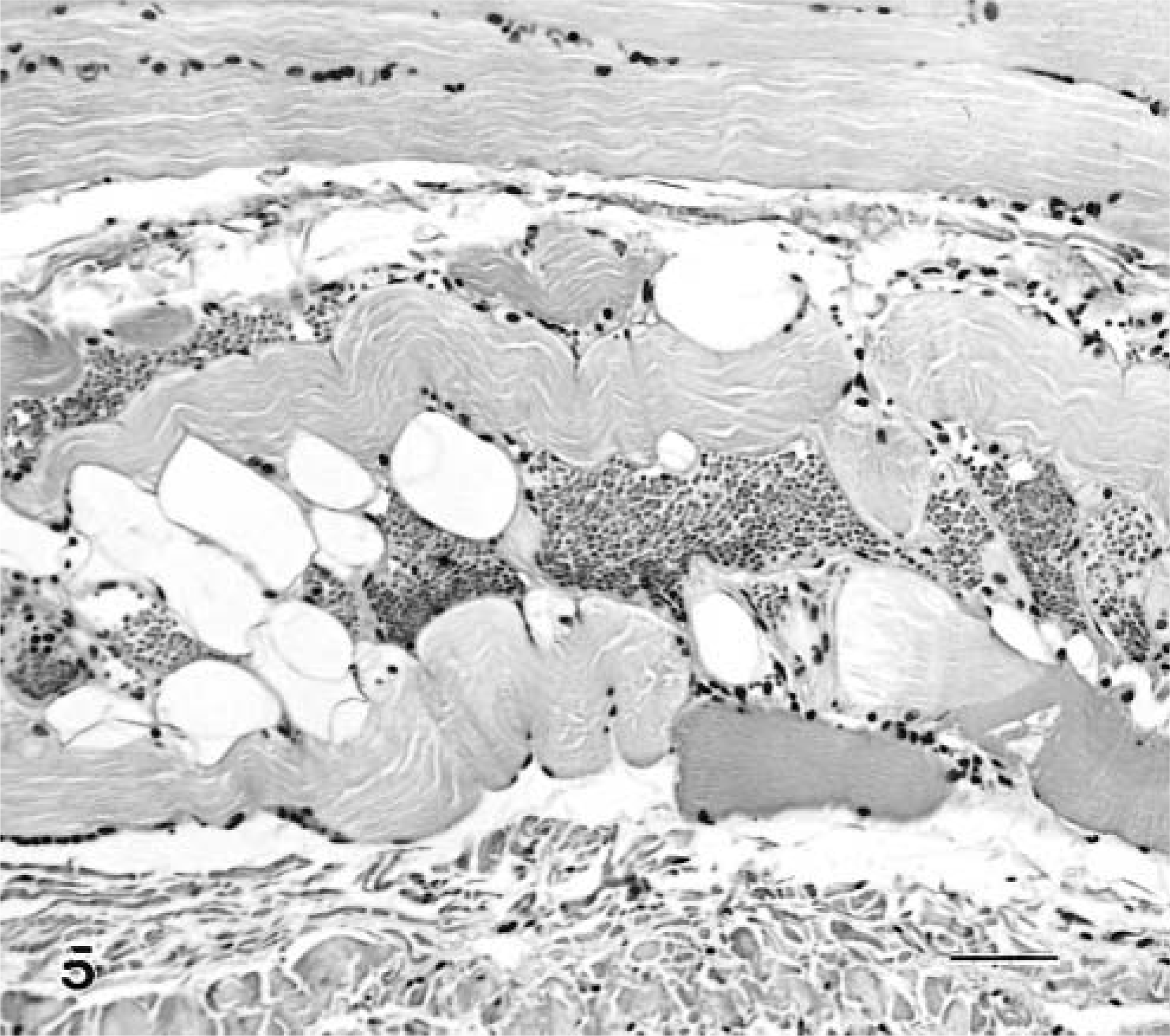
Mixed intramuscular hemangioma; dog; case No. 3. Mature adipocytes and blood vessels are infiltrating myofibers with segmental fiber degeneration. HE. Bar = 100 μm.
The infiltrating angiolipoma in case No. 5 was located in the right submandibular area. The surgeon indicated that the mass had an invasive growth pattern and could not be completely resected because the tumor encompassed the carotid artery. The bulk of the tumor was located external to the muscle (Fig. 6). An additional histologic finding in this tumor was the presence of fibrin thrombi in a few vascular spaces. The patient was reported in good health 1 week after surgery.
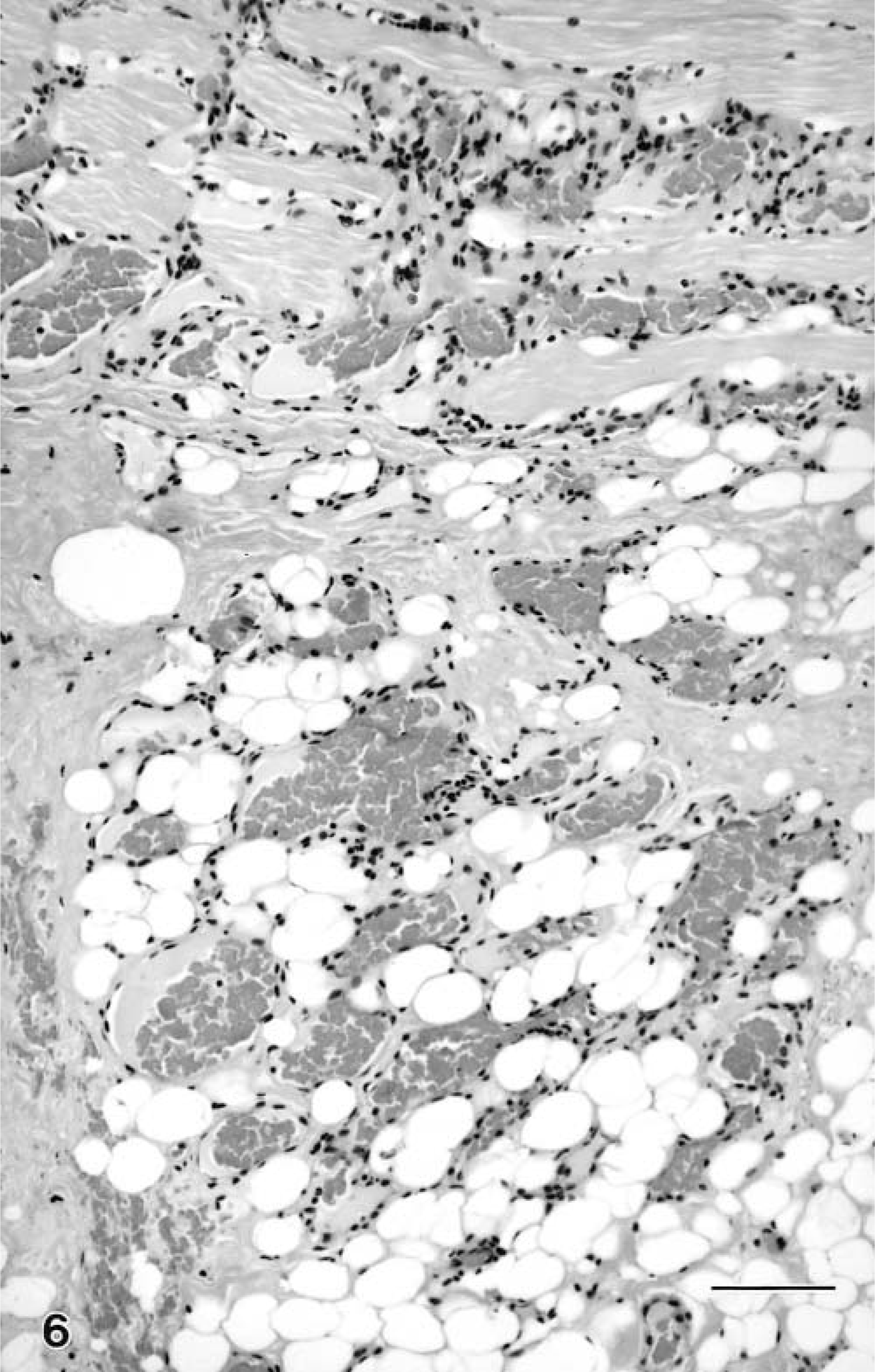
Infiltrating angiolipoma; dog; case No. 5. The tumor is composed of mature adipocytes and blood vessels with fibrous stroma. Neoplastic tissue extends into the muscle bundle. HE. Bar = 100 μm.
Differentiation of an angiolipoma with sparse vascularity from a simple lipoma and a highly vascular angiolipoma from a hemangioma infiltrating adipose tissue could both present a diagnostic challenge. Presence of large vessels not normally seen in lipoma and absence of nerves normally seen in adipose tissue are features that may allow differentiation.7 Presence of fibrin thrombi in human hemangiolipomas is a diagnostically significant feature that is absent in pure lipomas.4 Fibrin thrombi were seen in case Nos. 1, 2, 4, and 5. Absence of nuclear atypia and mitotic figures warrants consideration of nonneoplastic lesions, such as nodular hyperplasia, nevus, and hamartoma, in a list of differential diagnoses. Of these, hamartoma (when defined as a tumor-like malformation composed of mature or nearly mature components of the organ in which they occur) is appropriate but raises the issue of whether they are congenital or acquired lesions. Cytogenetic analysis of a group of human angiolipomas revealed that all examined lesions had a normal karyotype, supporting a hamartomatous origin, whereas simple lipomas in humans have characteristic clonal chromosomal aberrations.11 Pathogenetic analysis of canine angiolipomas has not been conducted. Human and canine angiolipomas are currently classified as neoplasms and are uniformly benign. Complete surgical excision is curative.
Angiolipomas in human beings are subdivided into solitary, multiple, and infiltrating types. Multiple lipomas are the most common type and occur predominantly in young adult males. The extremities and trunk are common sites.4,5 Age, sex, and site predilections for angiolipomas in dogs and cats are unknown. Canine angiolipomatous tumors in this report occurred in males, and the tumors were detected and removed early in the second hemidecade. The trunk is a common site for lipomas in dogs and apparently also for angiolipomas.7 Angiolipomas in human beings are often painful.4,5 No patient discomfort upon tumor palpation was recorded in the clinical histories of cases in this report. In human beings, angiolipomas are further subdivided into capillary, cavernous, mixed, and cellular patterns on the basis of the vascular component.5 The cavernous pattern predominated in case Nos. 1, 2, and 4. The cellular type may contain up to 90% vessels and must be differentiated from Kaposi's sarcoma or angiosarcoma.9 Human angiolipomas seldom exceed 2 cm in diameter, and the angiolipomatous tumors in case Nos. 1, 2, and 4 are similar in size.4 The subcutis is the primary site for angiolipomatous tumors in human beings and apparently in dogs; however, tumors composed of vascular, adipose, and/or connective tissues can occur in other sites, such as the head and neck,1 breast,3 and spinal cord.12 They have the potential to arise in any body structure having mesodermal tissue.
Classification of these tumors is based simply on their tissue components. A mass composed of mature adipose tissue is classified as a lipoma, and therefore, a mass composed of mature adipose, fibrous, and vascular tissue is classified as an angiofibrolipoma. Positive staining by Masson's trichrome method and/or negative immunohistochemical staining for smooth muscle actin allow for easy differentiation of an angiofibrolipoma from an angiolipoleiomyoma.
An infiltrating angiolipoma is a cutaneous mass composed of adipose tissue and blood vessels with a biological behavior similar to infiltrative lipoma. An intramuscular hemangioma is a tumor composed of blood vessels that develops within muscle. Most human intramuscular hemangiomas (>90%) are mixed with a variable adipose tissue component.2 Age, sex, and site predilections for intramuscular hemangiomas are similar to those observed in angiolipomas. Human intramuscular hemangiomas are larger than angiolipomas and tend to average 6.5 cm in diameter.2 Tumor sizes in case Nos. 3 and 5 are similar to this average diameter and are larger than the other angiolipomatous tumors described in this report. Determination of whether the mass has formed within the muscle or has invaded the muscle is subjective. Both are benign neoplasms. In human beings, they both tend to recur following incomplete excision. The classification of infiltrating angiolipoma may be in transition, e.g., a recent text proposed that they be classified as intramuscular hemangiomas,5 and another suggested that many earlier descriptions of infiltrating angiolipomas of muscle may be examples of intramuscular hemangiomas with a significant adipose tissue component.4 In case No. 3, absence of a well-defined mass external to the muscle tends to favor a diagnosis of mixed intramuscular hemangioma. Conversely, presence of a mass external to the muscle in case No. 5 supports a diagnosis of infiltrating angiolipoma.
Although angiofibrolipoma and infiltrating angiolipoma are not included in a recent edition of the monograph on classification of mesenchymal tumors of domestic animals,8 they are distinct neoplasms. Their vascular component warrants separate classification from the histologically similar fibrolipoma and infiltrating lipoma, respectively.