
Abstract
The barrier function of mammalian skin is maintained by intercellular stratum corneum lipids. In human patients with atopic dermatitis, an abnormal lipid barrier results in dry skin and increased transepidermal water loss. At this time, it is not known if a defective lipid barrier is present in atopic dogs. Normal and atopic canine skin were postfixed in ruthenium tetroxide and studied using transmission electron microscopy to determine structural differences within stratum corneum lipids. Intercellular lipid lamellae were graded on a semiquantitative scale. The deposition of stratum corneum lipid lamellae in atopic canine skin appeared markedly heterogeneous compared with that seen in normal canine skin. When present, the lamellae often exhibited an abnormal structure. The continuity and thickness of the intercellular lipid lamellae were significantly less in nonlesional atopic than in normal canine skin. These preliminary observations suggest that the epidermal lipid barrier is defective in atopic canine skin. Additional studies are needed to further characterize the biochemical defect and to possibly correct it with nutritional and/or pharmacologic intervention.
The barrier function of mammalian skin is maintained by epidermal lipids, especially those interspersed between the layers of the stratum corneum. In mammalian stratum corneum, epidermal lipids consist of ceramides, cholesterol, cholesterol sulfate, fatty acid esters of cholesterol, free fatty acids, and sphingosine. 3 Disruption of this barrier function by compounds (e.g., detergents, solvents) or disease states (e.g., ichthyoses, atopic dermatitis) can alter the relative concentration of these lipids and result in an increase in transepidermal water loss.
Human patients with atopic dermatitis (AD) commonly exhibit dry skin, a phenomenon known as atopic xerosis. 2,9 In this condition, the lipid barrier of the skin is compromised by delayed and incomplete extrusion of lamellar bodies that results in a change in the lipid composition of the stratum corneum. 4 A marked decrease in stratum corneum ceramides has been found in the skin of human patients with AD, 6 and a novel enzyme with sphingomyelin deacylase activity has been discovered recently in the skin of humans with AD. 5 This enzyme competes with sphingomyelinase and beta-glucocerebrosidase for sphingomyelin or glycosylceramide substrates and thus contributes also to the deficiency in epidermal ceramides seen in atopic skin. 5 Taken together, these abnormalities of the lipid barrier are suspected to increase contact of allergens with epidermal immune cells and to lead to a Th2 predominant immune response. 7
The purpose of this pilot study was to investigate whether ruthenium tetroxide postfixation electron microscopy was a suitable technique for visualizing stratum corneum intercellular lipids in canine skin. Moreover, we wished to determine whether dogs affected with AD, compared with normal dogs, also exhibited abnormal stratum corneum lipids.
Punch biopsy specimens (6 mm) were obtained from the lateral thorax of five normal dogs and from clinically normal skin of five dogs diagnosed with AD, based on Willemse's criteria 11 and exclusion of similar pruritic diseases. Normal dogs were all Beagles and atopic dogs were of various breeds. In each group, there was a mixture of male and female dogs, and all animals were neutered or spayed. All dogs were between 1 and 6 years of age. Skin biopsy specimens were snap-frozen in liquid nitrogen and stored at −70 C until processing. Frozen skin sections (20 µm) were cut on a cryostat, mounted on positively charged slides, air dried, and fixed in Trump's fixative (4% formaldehyde, 1% glutaraldehyde in phosphate buffer). Sections were postfixed in 0.25% phosphate-buffered ruthenium tetroxide (Polysciences, Warrington, PA) for 45 minutes at 4 C to preserve and stain epidermal lipid. The sections were dehydrated through graded ethanol solutions, cleared in acetone, and infiltrated with and embedded in Spurr's resin. Thin sections (800–1,000 Å) were mounted on copper grids and examined on a Philips EM208S transmission electron microscope operating at an accelerating voltage of 80 kV.
At least five electron micrographs from all specimens were taken of the lower and middle stratum corneum at magnifications of 17,000–40,000. All photomicrographs were examined in a blinded fashion by two of the investigators and the stratum corneum lipid lamellae were graded on a semiquantitative scale. The continuity of lipid deposition was scored on each photograph as follows: 1 = very patchy and interrupted lipid layers; 2 = intermediate between 1 and 3; 3 = some interruption in the lipid layers; 4 = intermediate between 3 and 5; and 5 = continuous uninterrupted lipid layers. The thickness (number of bilayers) of lipid deposition at sites where lipids were present was estimated as follows: 1 = few lipid bilayers; 2 = intermediate between 1 and 3; 3 = moderate number of lipid bilayers; 4 = intermediate between 3 and 5; and 5 = high number of lipid bilayers. The scores from each investigator were averaged. Both the continuity and thickness of lipid bilayers were compared between normal and atopic specimens using a nonparametric t-test (Mann-Whitney test; Prism, GraphPad, San Diego, CA).
Ruthenium tetroxide fixation permitted the visualization of stratum corneum intercellular lipids as multilayered lamellae in normal canine skin (Figs. 1–3). The intercellular lamellae were found within all levels within the stratum corneum. The number of lamellae differed between and within corneocytes. Lamellar bodies extruding lipid into the intercorneal spaces within the lower stratum corneum were present. The deposition of lipid in the stratum corneum of atopic canine skin was markedly heterogeneous (Fig. 4) compared with that of normal canine skin. Many areas within the AD stratum corneum were devoid of lipid. When present, the lamellae often exhibited an abnormal and/or incomplete structure (Fig. 5). Lamellar bodies extruding lipids were also present. An apparent retention of lamellar bodies in the cytoplasm of stratum granulosum cells was not noted (data not shown). When photomicrographs were evaluated using the 5-point semiquantitative scale, the values for both continuity and thickness of intercellular lipid were significantly less in the nonlesional atopic than in the normal canine skin (P = 0.0013 and P < 0.0001, respectively; Mann-Whitney test) (Table 1, Figs. 6, 7).
Semiquantitative scores ∗ for continuity and thickness of lipid lamellae in canine skin.
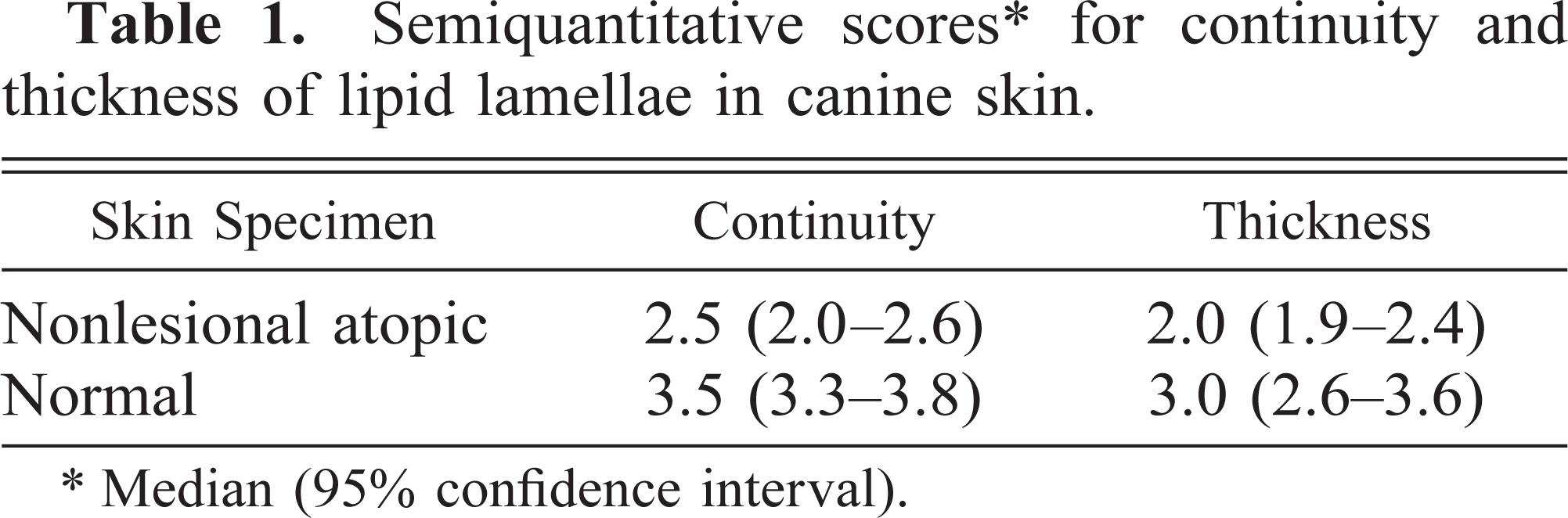
∗ Median (95% confidence interval).
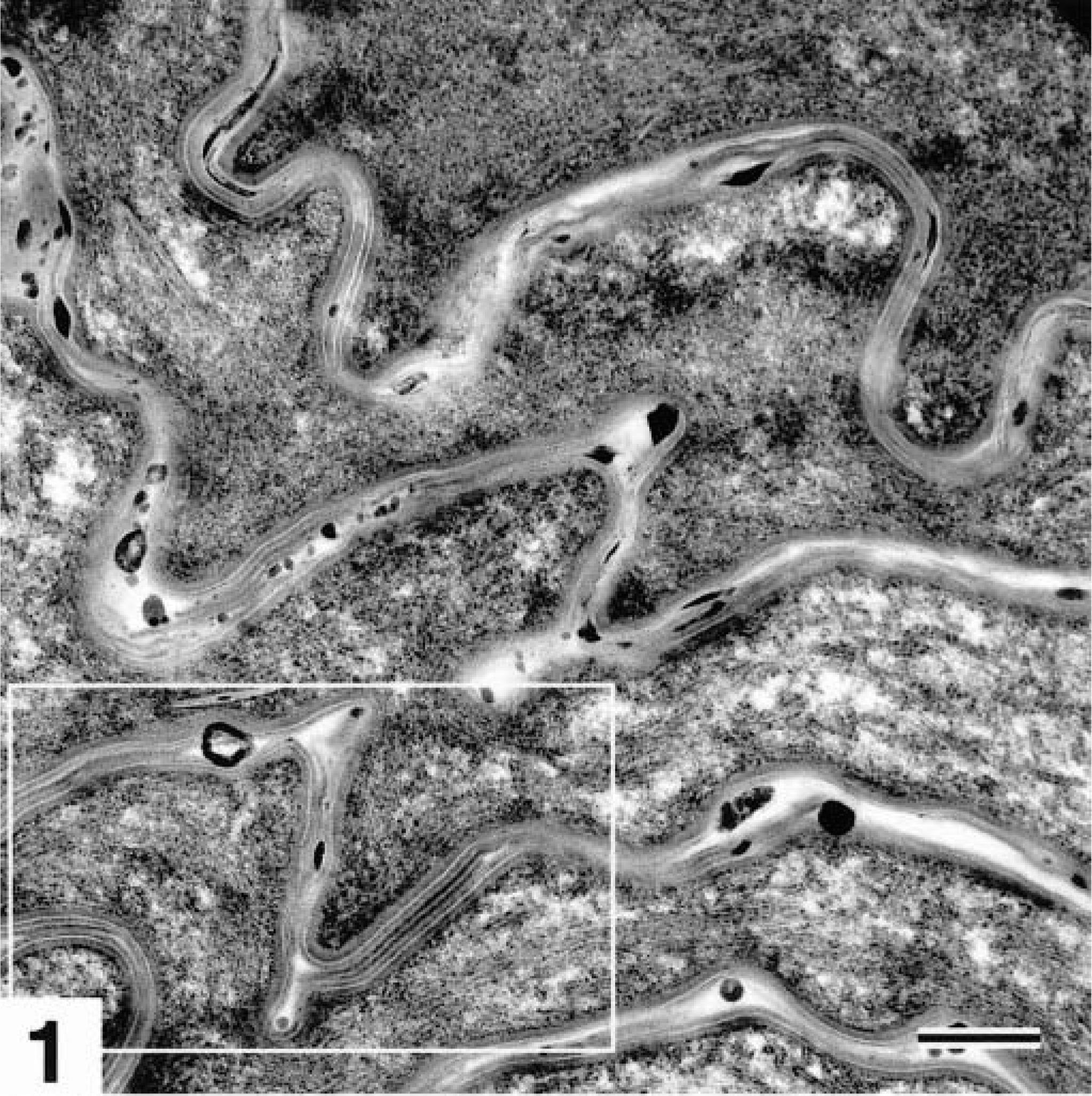
Transmission electron micrograph. Skin, stratum corneum; normal dog. Lipid lamellae can be seen in the space between keratinocytes (white box). Ruthenium tetroxide postfixation. Bar = 220 nm.

Transmission electron micrograph. Skin, stratum corneum; normal dog. Detail of Fig. 1. Well-formed lipid lamellae fill the intercellular spaces (white box). Ruthenium tetroxide postfixation. Bar = 110 nm.
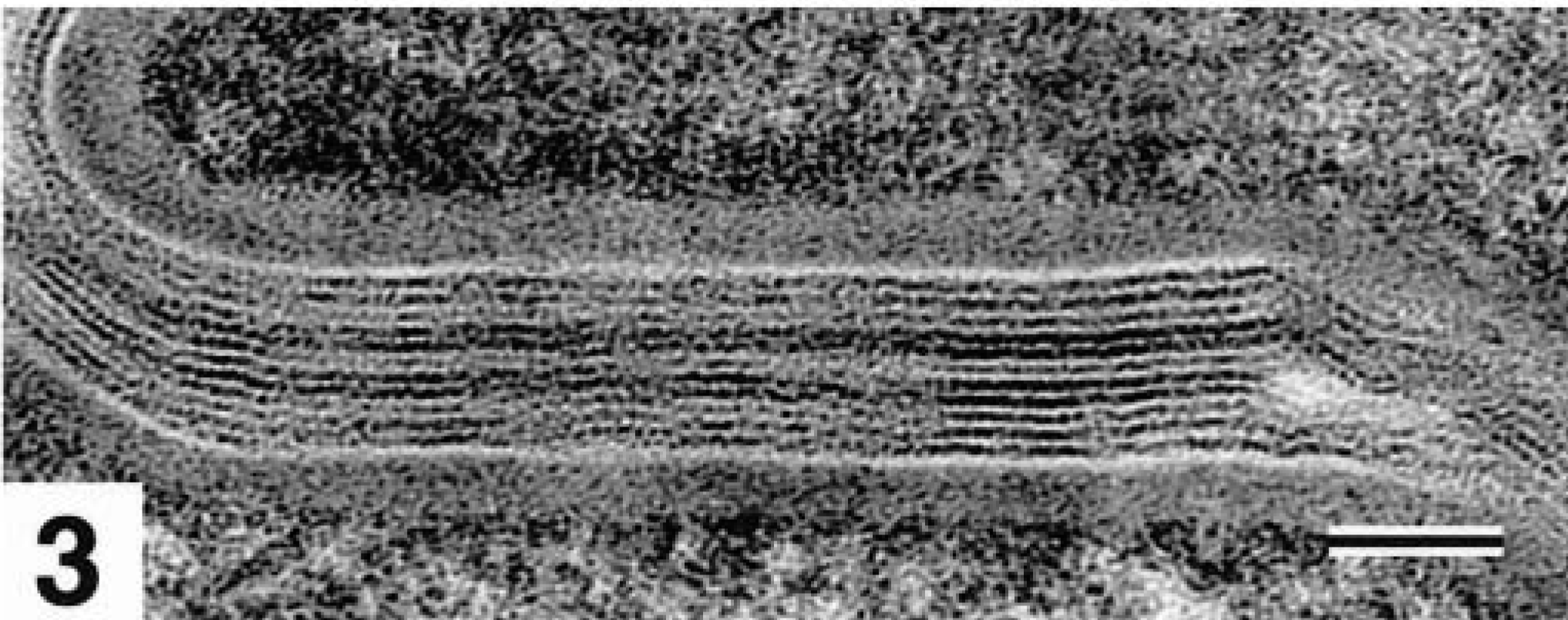
Transmission electron micrograph. Skin, stratum corneum; normal dog. Detail of Fig. 2. Intercellular lipid lamellae are composed of alternating layers of polar lipid heads (electron dense, black) and nonpolar regions (electron lucent, white). Ruthenium tetroxide postfixation. Bar = 50 nm.
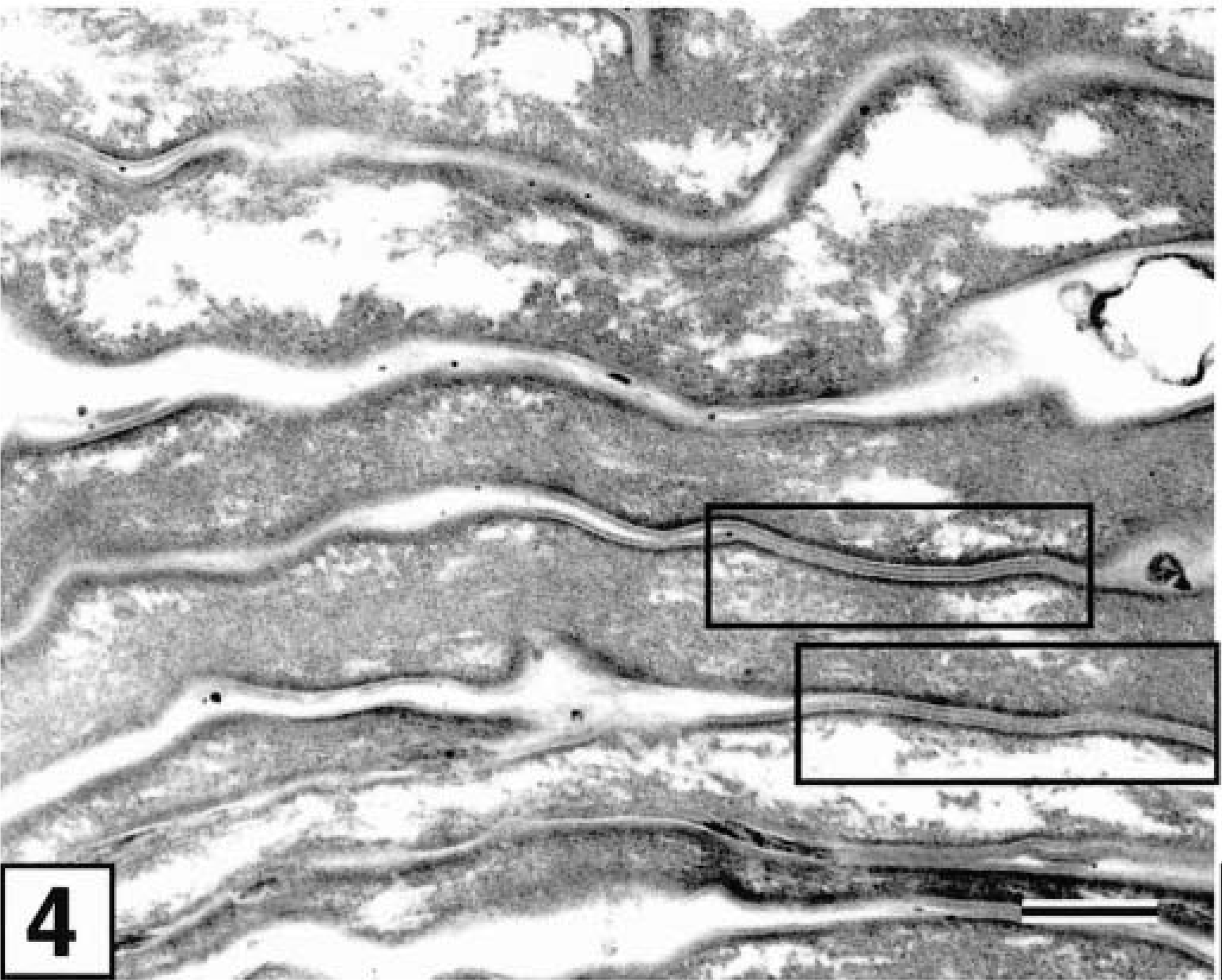
Transmission electron micrograph. Clinically normal skin, stratum corneum; dog with AD. The deposition of epidermal lipid lamellae is markedly heterogeneous and is seen only in a fraction of intercellular spaces (black boxes). Ruthenium tetroxide postfixation. Bar = 300 nm.
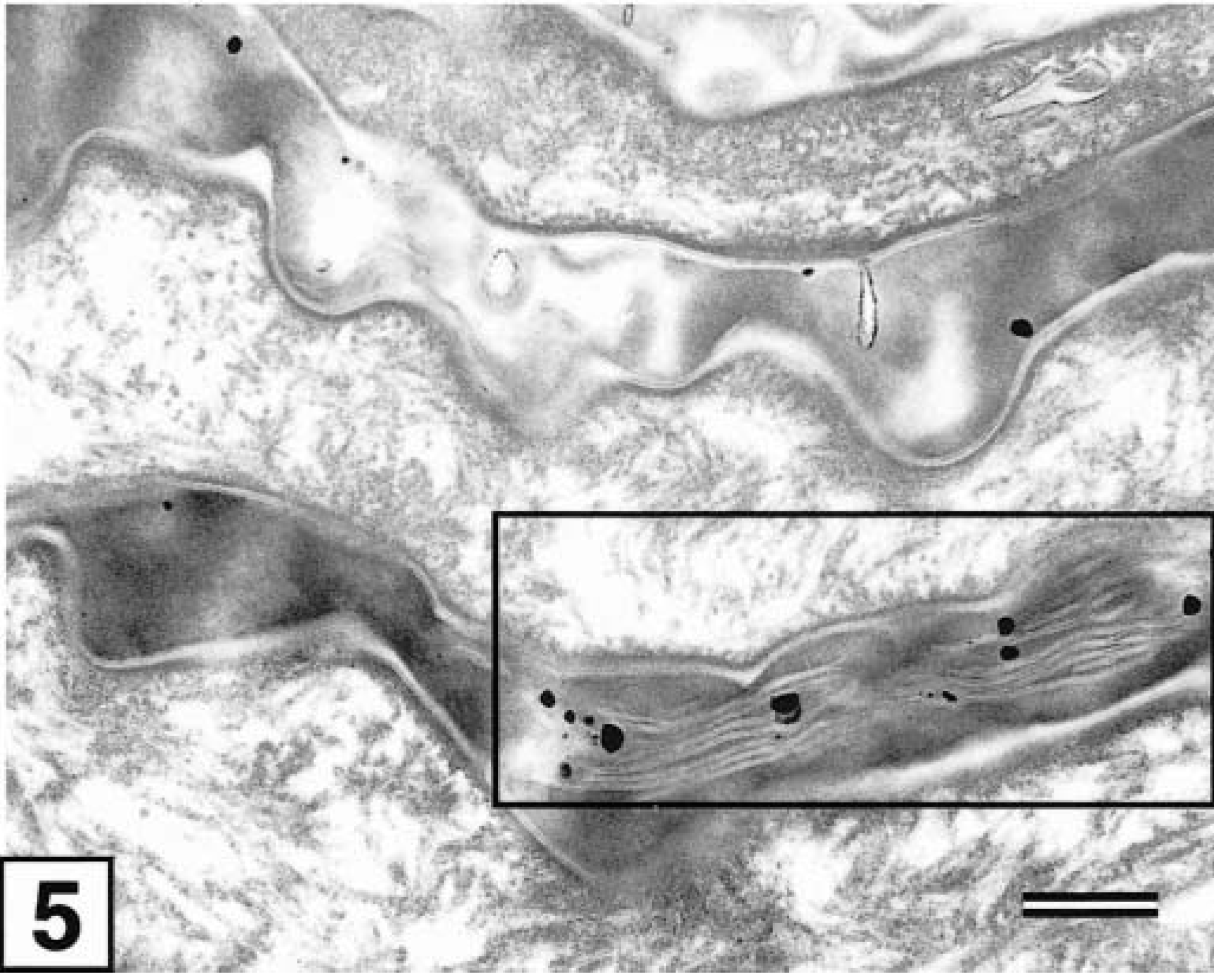
Transmission electron micrograph. Clinically normal skin, stratum corneum; dog with AD. When present, intercellular lipid lamellae usually exhibit an abnormal and incomplete structure (black box) compared with those of normal canine skin. Ruthenium tetroxide postfixation. Bar = 75 nm.
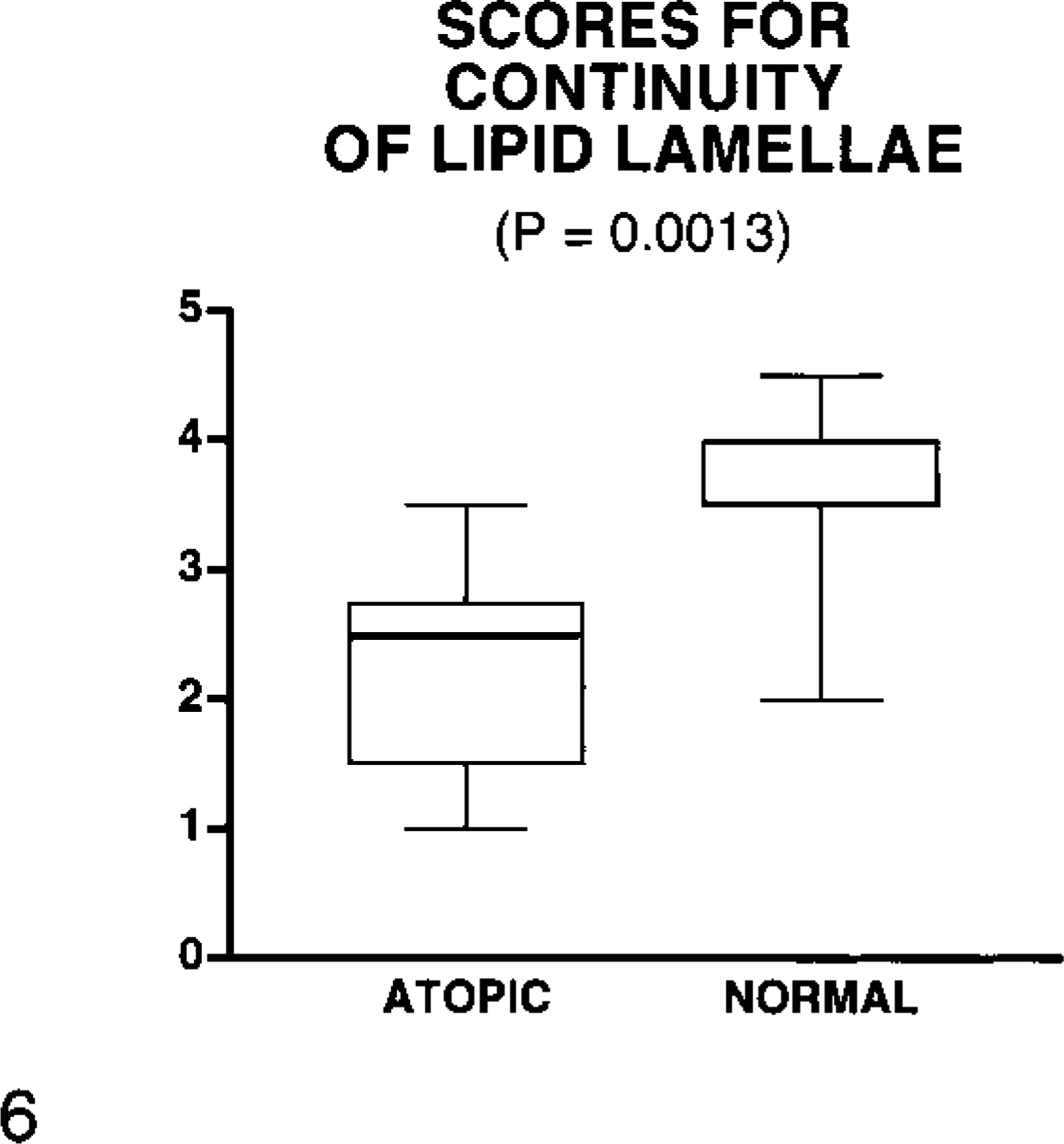
Box plot of semiquantitative scores for the estimation of the continuity of lipid lamellae in canine skin. Values for atopic dogs were significantly lower than those for normal dogs (P = 0.0013); whiskers denote the range of the values, the thickest line highlights the median, and the box represents the 25th and 75th percentiles.
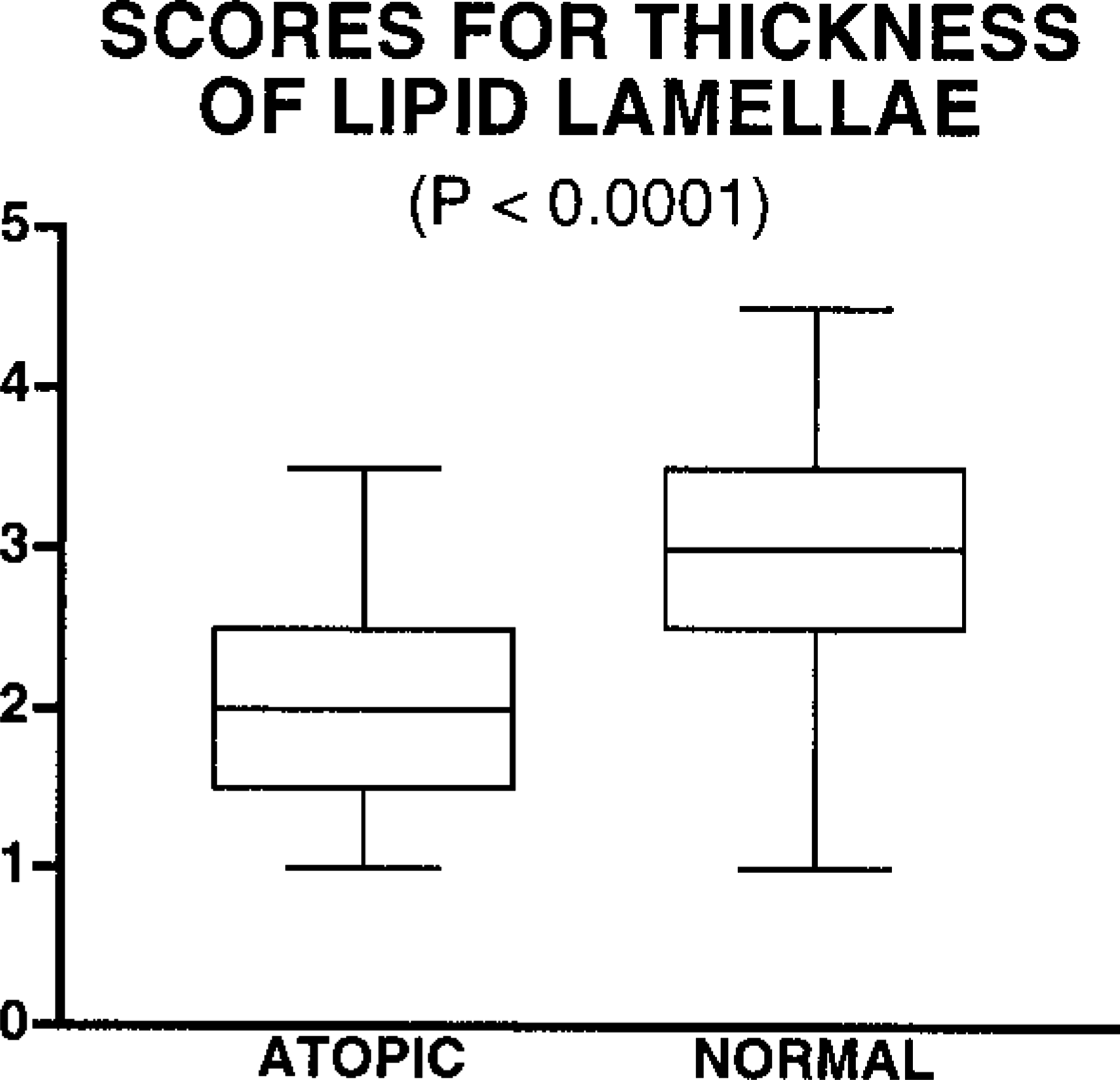
Box plot of semiquantitative scores for the estimation of the thickness of lipid lamellae in canine skin. Values for atopic dogs were significantly lower than those for normal dogs (P = 0.0013); whiskers denote the range of the values, the bar inside the box highlights the median, and the box represents the 25th and 75th percentiles.
Transmission electron microscopy of ruthenium tetroxide–fixed skin revealed extensive lipid lamellae deposition in the intercellular spaces of the stratum corneum in normal human, mouse, and pig. 1,8,10 The results of the present study confirm that ruthenium tetroxide fixation is a suitable technique for investigating epidermal barrier defects in canine skin. These preliminary observations suggest that lipid lamellae deposition is heterogeneous in atopic compared with normal canine skin. In addition, both the continuity and thickness of lipid lamellae in the skin of dogs with AD appear significantly less (P < 0.05) than those of normal dogs. Additional research is needed to further characterize the biochemical defect and to develop possible nutritional and/or pharmacologic interventions.