
Abstract
Two 5-year-old grade male horses presented with epiphora, rhinorrhea, conjunctival and nasal mucosal hyperemia, and dorsal and thoracic macropapular rash. Skin biopsies were collected from the affected areas, and serial sections were evaluated following hematoxylin and eosin and immunoperoxidase histochemistry staining by using a murine monoclonal antibody of the immunoglobulin G2A isotype recognizing the 30- kDa membrane protein of equine arteritis virus (EAV). In both horses, lesions consisted of mild to moderate diffuse superficial dermal edema and vasculitis with mild perivascular lymphocytic infiltrates, occasional endothelial hypertrophy, and single-cell necrosis of tunica media myocytes. Immunohistochemically, a few endothelial cells, myocytes, and pericytes containing intracytoplasmic EAV antigen were identified. Immunoperoxidase histochemistry of skin biopsies can be used as an ancillary test for the clinical diagnosis of equine viral arteritis in horses, especially when a cutaneous macropapular rash is evident.
Vasculitis is a relatively frequent finding for the pathologist evaluating equine tissues. Equine arteritis virus (EAV) induces panvasculitis, occasionally associated with a macropapular rash. 3 5 Equine herpesvirus 1 (EHV-1) infects the endothelium, medial myocytes, and pericytes of blood vessels in various tissues and organs of fetuses, foals, and adult horses. This vascular lesion is an important feature of EHV-1–associated encephalomyelopathy. Other equine viral agents producing vascular lesions are the African horse sickness orbivirus, which localizes within the endothelium and macrophages, and the Hendra disease morbillivirus; morbillivirus-infected horses may exhibit severe pulmonary hemorrhage and systemic vascular lesions resembling EAV vasculitis, with formation of endothelial syncytia and virus localization within endothelia. The arbovirus agents of Eastern, Western, and Venezuelan equine encephalitides may cause cerebral and visceral vasculitis. All these diseases may be characterized by systemic vasculitis. 3 In addition, purpura hemorrhagica presents with severe vascular involvement, 6 as does listeriosis in foals. 12 This manuscript describes the diagnosis of EAV infection in two horses with cutaneous macropapular rash and vasculitis by use of monoclonal antibody immunoperoxidase histochemistry identification of EAV viral antigen on formalin-fixed, paraffin-embedded skin biopsies.
Two 5-year-old grade male horses, imported to the North of Italy from Eastern Europe, presented with epiphora, rhinorrhea, conjunctival and nasal mucosal hyperemia, and diffuse macropapular rash extending to the dorsum and lateral thorax. Skin biopsies were collected from the affected areas and fixed in 10% buffered formalin.
The tissues were dehydrated with alcohols and xylene and embedded in paraffin. Five-micrometer serial sections were mounted on glass slides for histopathological and immunohistochemical evaluation. Sections were stained with hematoxylin and eosin for histopathological evaluation. For immunohistochemical evaluation, serial sections were processed using two different murine monoclonal antibodies. Both monoclonal antibodies were of the immunoglobulin G2A isotype, and both reacted with the envelope glycoprotein C of equine herpesvirus 1 (courtesy of Dr G. Allen, Gluck Equine Research Center, University of Kentucky, Lexington, KY) and a 30-kDa membrane protein of EAV (courtesy of Dr A. Glaser, New York State Diagnostic Laboratory, Cornell University, Ithaca, NY), respectively. Both antibody preparations were diluted 1:5 in phosphate-buffered saline containing 4% horse serum. Immunohistochemistry slides were counterstained with hematoxylin. The technique has been previously described in detail. 7 Positive controls consisted of lung tissues from foals containing EHV-1 and EAV antigens, respectively.
In both horses, lesions were mild to moderate and consisted of diffuse superficial dermal edema and mild perivascular lymphocytic infiltrates (Fig. 1), with occasional endothelial hypertrophy and single-cell and fibrimoid necrosis of tunica media myocytes. Immunohistochemically, a few endothelial cells, myocytes, and pericytes containing finely granular intracytoplasmic EAV antigen (Fig. 2) were identified in both samples. Both skin biopsies were negative for EHV-1.
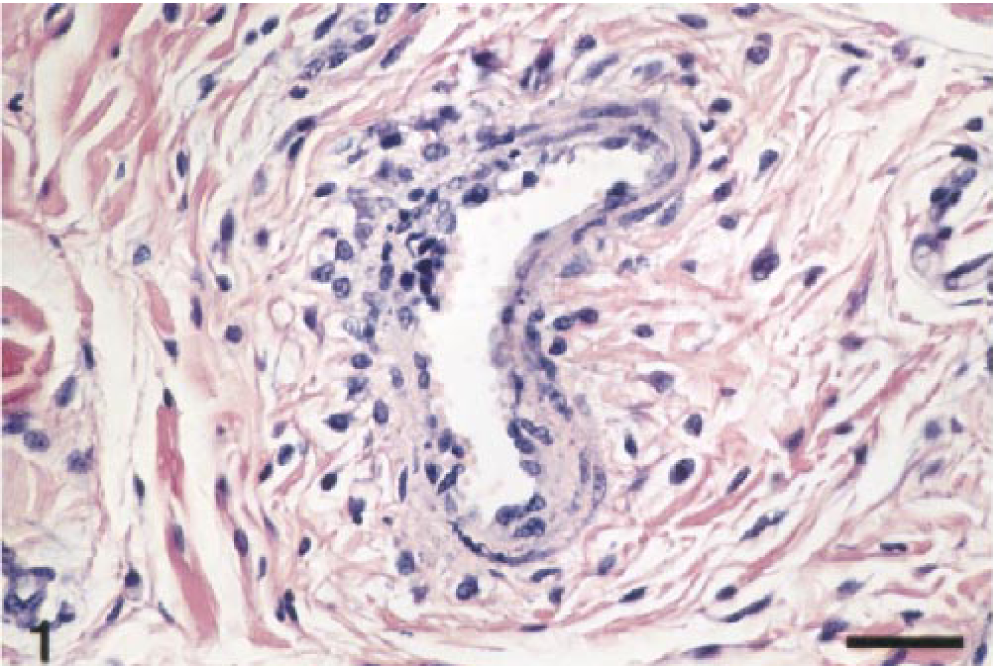
Horse dermis. Mild vasculitis characterized by endothelial swelling, fibrinoid necrosis and medial and perivascular lymphocytic infiltrates. Hematoxylin and eosin. Bar = 80 μm.
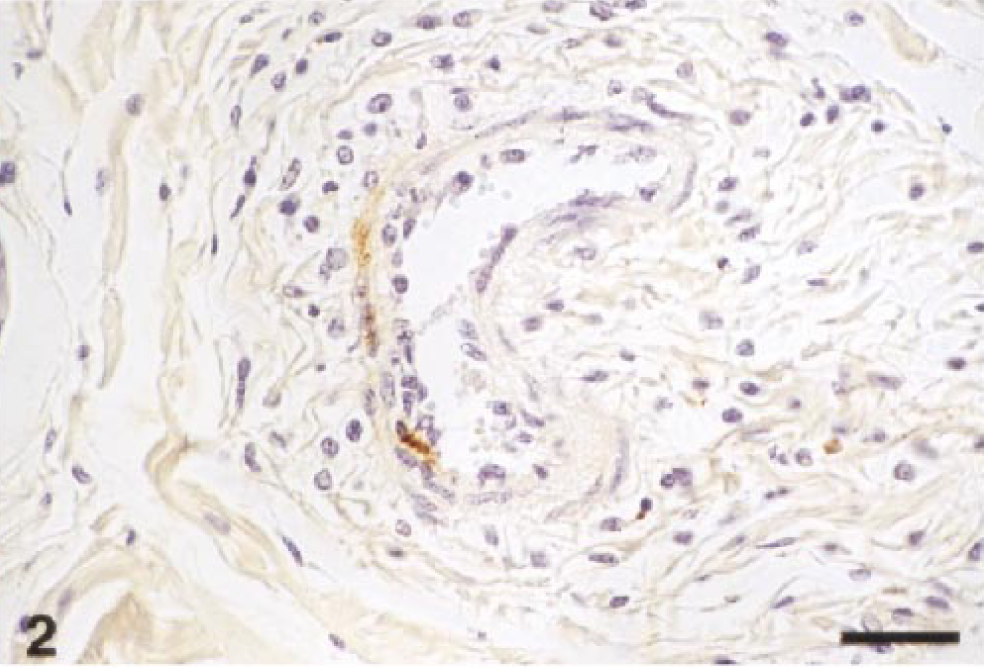
Horse dermis. EAV antigen is present within the cytoplasm of a myocyte and pericytes. Immunoperoxidase histochemistry and hematoxylin. Bar = 80 μm.
EAV is an arterivirus, 1 which causes panvasculitis, systemic disease, and abortion in horses. 3 5 Localization of EAV within the endothelium is observed in adult horses and foals 5–6 days after infection, and then the virus can extend to vascular myocytes and pericytes. 2–4 In experimental studies, EAV antigen persists within the blood vessels for at least 10 days following their infection. Moreover, EAV antigen persists in the systemic blood vessels and the renal tubular epithelium during the late phase of the infection. 2–4, 7 11 The mechanism of vasculitis induced by the EAV is poorly understood, but a direct cytopathic effect of the virus on endothelial cells and tunica media myocytes may play a major role in the early phase of infection. In addition, small T lymphocytes of perivascular infiltrates may induce cytolysis of EAV-infected vascular cells. This cytolytic activity may be mediated by class 1 major histocompatibility complex–restricted CD8+ T cells, as previously described in EHV-1–infected CBA (H-2 [k]) mice. 10 Immunocomplexes have not thus far been demonstrated within the affected blood vessels in EAV-infected horses.
Immunoperoxidase histochemistry of skin biopsies is an ancillary test for the clinical diagnosis of equine viral arteritis in horses, especially when a cutaneous macropapular rash is evident. The collection of blood and tissues for virus isolation and possibly for reverse transcriptase–polymerase chain reaction, 8 as well as the evaluation of paired sera samples to identify seroconversion, 9 should always be performed. In fact, during the early phase of infection, the virus is either not present or present only in small quantities within the blood vessels. 3 The quantity of viral antigen within the endothelium may be variable during any phase of the infection, especially in those situations when EAV cutaneous lesions are mild or absent. Collection of more than one sample is advised. Considering that the EAV antigen is not present in large quantities within organs and tissues, including skin, 3 4 7 immunoperoxidase histochemistry is preferable to fluorescent antibody evaluation of frozen tissue sections. Specifically, immunoperoxidase histochemistry enables the contemporaneous evaluation of lesions by localizing antigen within the context of morphologic changes, with easy distinction of cell types, certain identification of small quantities of viral antigen (Fig. 2), and recognition of occasional nonspecific staining.
Footnotes
Acknowledgements
I am grateful to Alexis Wensky-Roberts of the Image Lab for photography.