
Abstract
Abstract
Malignant bone tumours around the forearm are rare. Nowadays, oncological and surgical management of bone sarcomas of this region has improved significantly. Although the anatomical features are complex, limb-sparing surgery is possible with wide surgical resection. Biological reconstruction methods are promising in this anatomically unique region. In addition, meticulous soft-tissue reconstruction yields good functional results in the hand and wrist.
This study reviews malignant bone tumours of the forearm and their oncological and surgical management. Malignant bone tumours should be treated with a multidisciplinary approach based on chemotherapy, radiotherapy and limb salvage procedures.
Introduction
The forearm is an extremely rare location for primary bone sarcomas. 1 Extremity lesions are detected earlier than axial tumours, as they will present fine trabecular changes on plain radiographs. Signs of malignancy, such as osteolysis, cortical erosion, new bone formation and periosteal reaction, may be present on radiographs. 2 Patients usually complain of persistent, unexplained, non-mechanical resting pain and soft-tissue swelling. Malignant bone tumours are often localized to the metaphysis. 1
MRI with intravenous contrast is essential in staging, evaluation of response to neoadjuvant chemotherapy and long-term follow-up of the malignancies. CT is preferred to determine the aggressiveness of bone lesions, including margination, calcification and cortical disruption. Bone scintigraphy and positron emission tomography may help to detect active and aggressive primary lesions and metastases. A biopsy is the final diagnostic step in evaluating malignancies and should be performed following radiological staging and multidisciplinary assessment.
Ewing sarcoma, osteosarcoma and chondrosarcoma of the forearm are the most common malignant bone tumours in this anatomical area. Survival rates of these sarcomas have tended to increase in recent years, especially with the development of chemotherapeutic agents. 3 In addition, surgical methods including endoprosthesis, allografts, vascularized autografts and allograft-prosthetic composites reconstruction methods have contributed to improve the functional outcomes of these patients.
Anatomical consideration of the forearm
The anatomy of the forearm is very complex. It includes 19 muscles, which are classified as 11 extensor muscles and the eight flexor muscles. Most of the muscles originate close to the elbow and extend to the fingertips. The compartmental anatomy of the forearm includes a dorsal and volar compartment. Although the third and fourth compartments are defined according to the anatomical location of the muscles, for tumour staging, the musculature of the forearm can be divided into volar and dorsal compartments, which are separated by the interosseous membrane. 4
Due to the complex anatomical structures of the forearm, resection with wide margins continues to pose a challenge for orthopaedic oncologists. Clear surgical margins during initial surgery are essential for patient survival. Reconstruction of the bone and soft tissues after resection of the bone tumour is also vital for minimizing hand and wrist function loss. Meticulous tumour resection and soft-tissue reconstruction should be done in this complex anatomy and limited tissue volume.
Biopsy technique
Radius diaphyseal lesions are usually resected through a volar approach; this should be taken into account when planning a biopsy.
CT or ultrasound-guided core needle biopsy and open incisional biopsy are valuable options to obtain a representative and sufficient sample of tissue while not compromising the definitive treatment. The type of biopsy should be discussed for each patient. 5 The planning and execution of open biopsy surgery should be performed as carefully as the definitive surgical procedure. The biopsy incision should be placed so that it can be incorporated into the definitive surgical incision. The biopsy incision should be longitudinal and parallel to neurovascular structures. 6 If there is a soft-tissue mass encircling the radius, an incisional biopsy may be performed with a longitudinal incision over the mass. For midshaft lesions, a lateral incision is made between brachioradialis and extensor carpi radialis longus without contaminating the major neurovascular structures. The same principles pertain to ulna lesions. A dorsolateral approach (through the subcutaneous border of the ulna) along the olecranon to wrist is preferred for ulnar diaphyseal lesions. The biopsy should be planned so that the biopsy tract can be removed entirely at the final resection without resecting any crucial structures.
Treatment
Orthopaedic oncologists prefer limb-salvage surgery in the majority of patients with malignant tumours involving the forearm. 7 Tumour-free margins should be obtained by wide surgical resection. Although a 1-cm margin has been recommended in the past, sarcomas grow longitudinally rather than in traverse fascial planes. With the help of adjuvant treatments, the smaller tissue cuffs may be sufficient in these cases. 2 Tumour-free margins can be achieved by limb-salvage surgery in most patients. The location of the tumour, size, proximity to neurovascular structures, distant metastasis, age and general condition of the patient should be taken into account for the decision of limb-salvage surgery or amputation. 8
Patients with Ewing sarcoma and osteosarcoma of the forearm can be treated with neoadjuvant (induction) chemotherapy followed by wide excision and adjuvant chemotherapy. Chemotherapy is used to diminish the tumour volume and eliminate micrometastases. Neoadjuvant chemotherapy improves long-term survival in patients with non-metastatic extremity osteosarcoma. 9 In addition, patients with a good response to chemotherapy have increased disease-free survival rates. 9
Osteosarcoma frequently occurs in the distal femur, proximal tibia and proximal humerus. Forearm osteosarcomas are relatively rare. 10 Symptoms around the forearm may be present for weeks, months or longer before the tumour is diagnosed. Since osteosarcomas are mostly radioresistant, radiotherapy should be kept only for selected cases.
Ewing sarcoma is a highly radiosensitive tumour. Local control should be maintained by surgical resection whenever possible to obtain wide margins with acceptable functional loss. When wide margins cannot be achieved, a post-surgical severe functional deficit predicted or an unresectable lesion is present, local control can be managed by definitive radiotherapy. 2 Radiotherapy can also be applied to maintain local control of the lesion in addition to surgical resection either pre- or postoperatively.
The forearm localization of chondrosarcoma is extremely rare. The most significant predictor of prognosis is its grade. The treatment of low-grade chondrosarcomas remains controversial. Very good results have been reported by intralesional curettage. 11 Reconstruction of the bone defect after curettage by graft packing or cementation is highly suggested. 11 A group of the authors is favoring wide resection in low-grade chondrosarcomas. 12 Wide or radical resection is highly recommended in the treatment of high-grade chondrosarcoma (Fig. 1).
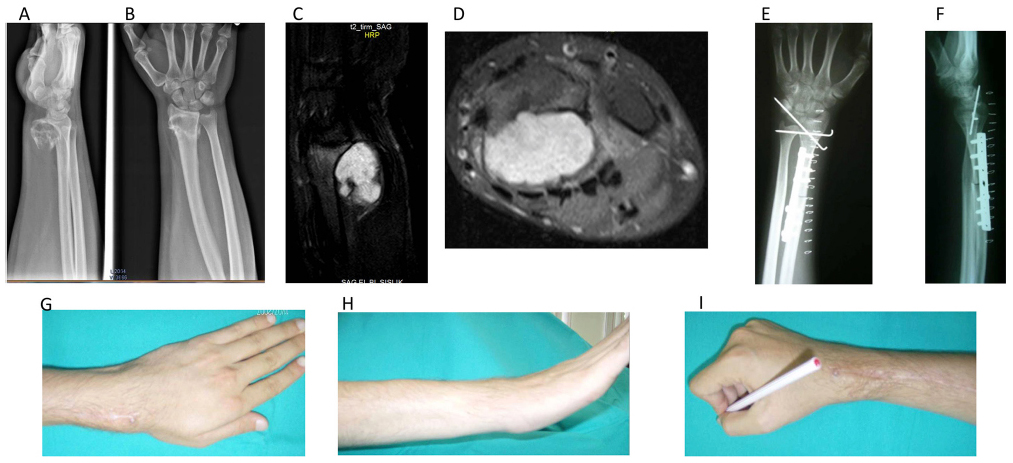
A 19-year-old male presented with chondrosarcoma of the distal radius. a) and b) preoperative radiographs showed a tumour mass; c) and d) preoperative MRIs demonstrated extra-compartmental extension of the tumour; e) and f) the patients underwent wide resection and biological reconstruction with an osteoarticular vascularized fibular graft; g), h) and i) at two years postoperative follow-up, the patient demonstrates good wrist function.
Resection techniques
In limb salvage, vascular reconstruction takes precedence, followed by bone reconstruction and soft-tissue reconstruction. Surgical margins should be wide and allow maintenance of hand function, whenever possible. 8 Talbert et al 13 reviewed 78 patients with sarcoma in the distal extremity and recommended resection with 1-cm margins followed by radiation therapy. On the other hand, Bray et al 14 reviewed 25 patients with sarcoma of the forearm and hand and recommended > 1-cm margins without radiation therapy. Pradhan et al 15 found that patients with high-grade osteosarcomas of the upper distal extremities have a higher amputation risk than other limb sites. In the literature, approximately 5% to 10% of malignant upper extremity tumours were treated with amputation. 2 Prior unplanned excision resulting in tumour contamination and high-grade tumour with neurovascular involvement are indications for amputation. It should be noted that performing limb salvage surgery on tumours in this location may not always be possible due to the involvement of critical structures.
Reconstruction techniques
After resection of the tumour, reconstruction in limb preserving surgery is commonly applied using biological or non-biological methods, including fibular autograft, allograft, recycling bone with or without vascularized fibula graft, one-bone forearm and arthrodesis methods (Fig. 2). Due to excellent adaptation, a free vascularized fibula graft is a good choice for reconstruction of forearm bone defects following tumour resection. 16 In addition, the use of a vascularized bone graft provides mechanical support (Fig. 3). Vascularized bone grafts can be used to reconstruct bone defects longer than 6 cm in the radial or ulnar diaphysis and distal radius. 17 It also provides rapid bone healing and union, adequate graft hypertrophy and resistance to chemotherapy, radiotherapy and infection.
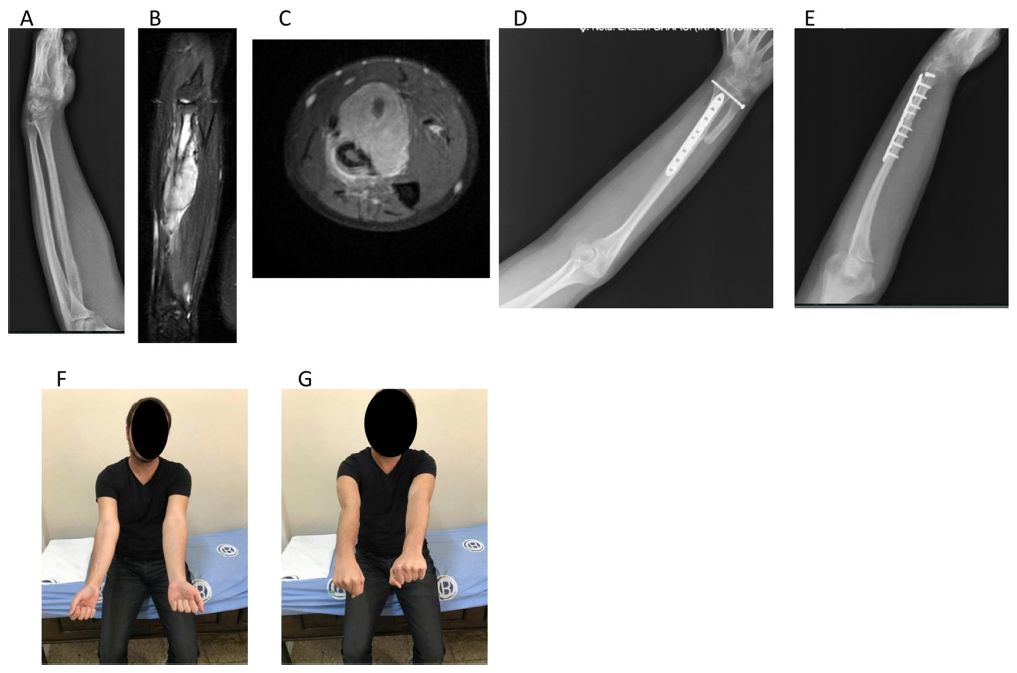
A 20-year-old male with radius diaphyseal Ewing sarcoma: a), b) and c) preoperative plain radiograph and MRIs showed a lesion involving the radial diaphysis and extending to soft tissue; d) and e) the patient underwent wide resection and reconstruction by one-bone forearm method; f) and g) a 12-month postoperative follow-up, the patient demonstrates good pronation and supination of the forearm.
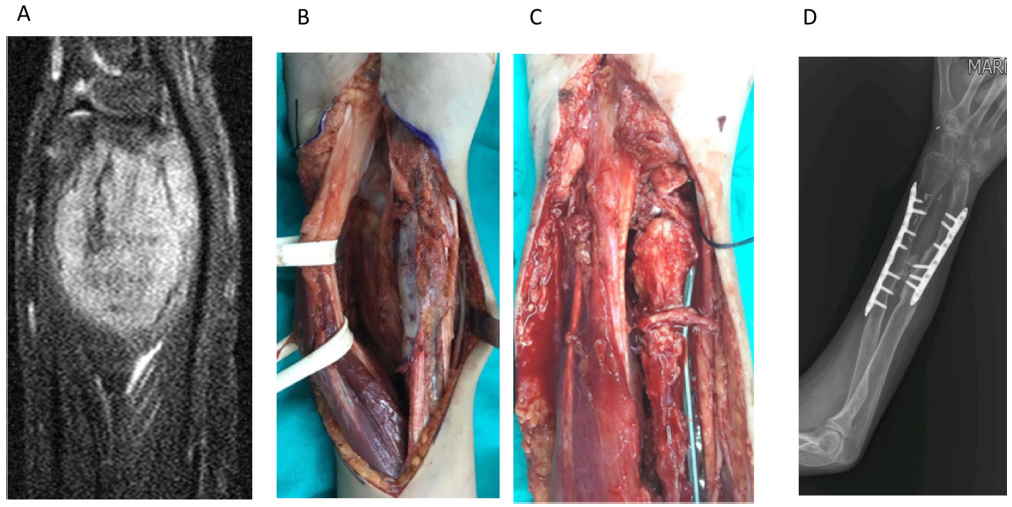
A 12-year-old male with distal radius osteosarcoma: a) MRI showed intra- and extraosseous extension of the lesion; b) and c) the patient underwent wide resection and biological reconstruction with osteoarticular vascularized fibular graft; d) union of the fibular graft with the host bone and a good anatomical match between the fibular head and the carpal bones are observed at long-term follow-up.
The distal radius is a common location for benign and malignant bone tumours. For distal radius, joint reconstruction using fibula head has been reported. 18 There is an initial anatomical match between the fibular head and the carpal bones. The fibular head transfer along with the shaft is a good procedure to replace the radio-carpal joint but is technically demanding 18 (Fig. 4). Onoda et al 18 reported eight tumour patients with reconstruction using vascularized fibular head grafts. They detected high complication rates, including infection, pseudoarthrosis and volar subluxation. However, this method may be a good option in selected patients.
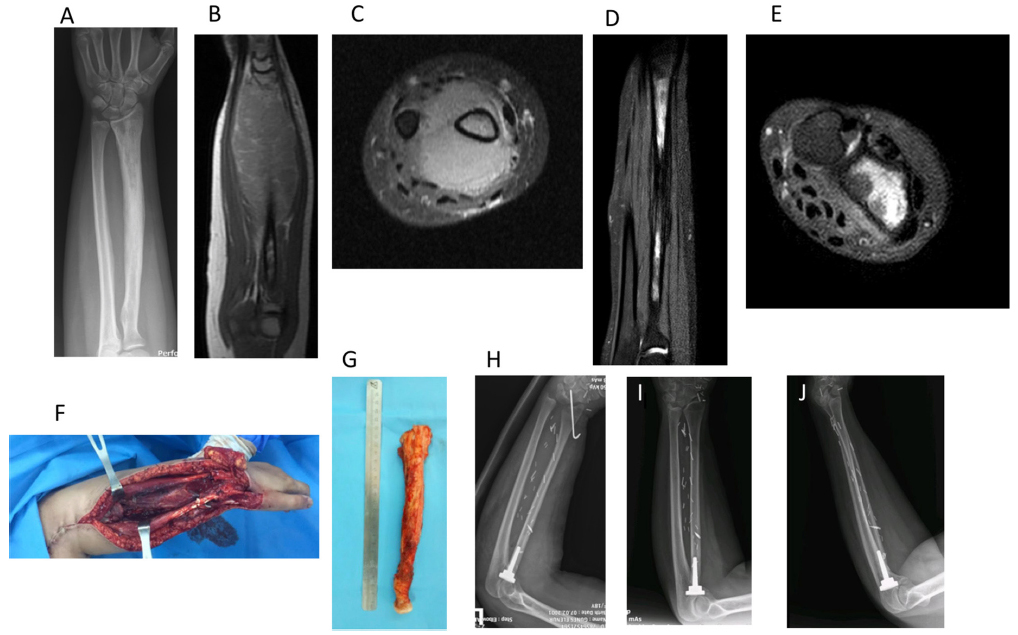
A 16-year-old female with radius diaphyseal Ewing sarcoma: a) preoperative plain radiograph; b) and c) initial; and d) and e) post-chemotherapy MRIs showed significant radiological response to neoadjuvant chemotherapy; f), g) and h) the patient had wide resection and biological reconstruction with osteoarticular vascularized fibular graft. A radial head prosthesis was also applied; i) and j) long-term follow-up radiographs demonstrated a good congruence at elbow and wrist joints
Patients treated with fresh-frozen allograft and rigid fixation have shown good functional and oncological outcomes. 19 This is generally preferred for wrist and elbow tumours. Intercalary allografts are used more often than osteoarticular allografts. Although these allografts can provide improved stability and function, they also present complications like nonunion, infection and graft resorption. 19
One-bone forearm reconstruction is a viable option to salvage the limb and to achieve good stability and a functional forearm. 20 The proximal part of the ulna is typically fixed to the distal part of the radius. The procedure attempts to create a single osseous bridge between the ulnohumeral and radiocarpal joints. This technique has postoperative complications including nonunion but may still be used successfully for limb salvage. 20
After wide resection, the exposure of essential structures such as nerves, vessels, tendons and bone can often necessitate soft-tissue transfer. Meticulous soft-tissue reconstruction is the leading factor contributing to high functional outcomes. Forearm soft-tissue reconstruction can be done with primary closure, skin grafts or free flaps. However, local pediculated flaps are not preferred. Free flaps can provide more durable and well-vascularized tissue than local or regional flaps. Various options for cutaneous flaps include anterior thigh flap, scapular flap and groin flap.21,22 Functional reconstruction of a limited muscle defect is usually done by tendon transfer. 23 Donor candidates for these tendon transfers are on the forearm. The determination of which tendon(s) can be transferred is mainly based on the localization of muscle defect. Occasionally, functional free muscle transfer is considered to provide a limited function. The procedure should help the child to open the hand and fingers when the wrist is in slight extension.
The most accepted method for restoring wrist extension after resection of the radial nerve is pronator teres to extensor carpi radialis brevis transfer. 24 The flexor carpi radialis, flexor carpi ulnaris and flexor digitorum superficialis transfers have also been described for radial nerve palsy. The palmaris longus or the ring finger flexor digitorum superficialis tendons can be transferred to extensor pollicis longus to restore thumb extension. 24
Oncological outcomes
Daecke et al 25 reported the clinical outcome of 33 patients with osteosarcomas of the peripheral upper extremities. The five-year survival rate was 86%, and the event-free survival rate was 65%. In our series of 114 patients with bone sarcomas, we found no significant difference in the survival rate of cases with upper versus lower limb bone sarcoma. 26
The five-year overall survival rate varied from 53% to 67% for upper distal extremities sarcomas in the literature.15,26 Approximately 15% to 38% of bone sarcoma patients may develop local recurrence and/or late-onset lung metastases.2,26 The standard approach for local recurrences is mostly radical amputation, whereas late-onset lung metastases are managed by resection and/or chemotherapy.
Conclusion
Bone sarcomas of the forearm are rare and continue to pose a challenge for orthopaedic oncologists. In these patients, the prodromal period may be extended due to the atypical clinical presentation. Wide surgical resection is required for limb-sparing surgery but resection and subsequent bone and soft-tissue reconstruction should be well planned due to anatomical difficulties in this region. Although various reconstruction techniques have been reported in the literature, biological reconstruction methods are promising. Meticulous soft-tissue reconstruction can be performed with primary closure, skin grafts, local grafts or free flaps. However, it should be kept in mind that free flaps are superior to local flaps in this region.
Treatment should be guided by a multidisciplinary team approach, and if a management strategy cannot be made with limb salvage, wide margins can be achieved by amputation.
Footnotes
OS: Concept, Design, Materials, Analysis and/or Interpretation, Literature search, Writing manuscript