
Abstract
Abstract
Purpose
To compare the histological healing and radiographic effects of tendons transferred to ossified or unossified bone using different tendon fixation techniques
Methods
Nine new-born piglets underwent bilateral tendon transfers to either the ossified boney calcaneal body or unossified apophysis. The tendons were fixed using metallic suture anchors, sutures alone or a bone tunnel. At six weeks of age, calcanei were harvested, radiologically imaged and then prepared for histology. A semi-quantitative aggregated scoring system with values ranging from 0 (poor) to 15 (excellent), was used to grade healing at the surgical enthesis and the apophyseal ossification was graded by five independent reviewers in triplicate using a modified (1 to 4) validated scoring system.
Results
Histologically, the cartilaginous transfers utilizing the tunnel and suture techniques also demonstrated the best average aggregated scores of entheses healing rivalling that measured in transfers using the classic bone tunnel technique (clinical benchmark), whereas suture anchor fixation demonstrated the worst healing in both the ossified and unossified samples. All three transfer techniques caused at least minor alterations in apophyseal ossification, with the most significant changes observed in the metallic suture anchor cohort. The tunnel and suture techniques demonstrated similar and more mild abnormalities in ossification.
Conclusion
Tendon transfers to unossified bone heal histologically as well as transfers classically performed through tunnels in bone. Suture fixation or tunnel techniques appear radiographically and histologically superior to suture anchors in our newborn porcine model.
Level of evidence
Introduction
Tendon transfers are common soft-tissue procedures utilized to improve function and/or dynamic anatomical alignment due to congenital, developmental or post-traumatic muscle imbalances, most commonly in paediatric hand and foot surgery. Talipes equinovarus and vertical talus are two congenital foot deformities in which tendon transfers have been reported.1–8 In both deformities, the tibialis anterior tendon is transferred, however, the tendon is transferred to different tarsal bones, in order to optimize the mechanical pull and correct residual deformity.2,9 In addition to being transferred into different bones, different surgical fixation techniques are used in each setting.1–8 In clubfeet, the tendon is transferred through a tunnel placed in the lateral cuneiform, thus it is recommended to wait until the cuneiform is ossified (three to four years of age) to ensure bone to tendon healing.1,10,11 However, in the procedure described by Dobbs et al 2 for vertical talus, the tendon is sutured to the cartilaginous surface of the talus and appears to heal without incident. This has led to the following questions: 1) how does the healing of a tendon transferred to ossified or unossified bone (cartilage) compare and do different tendon fixation techniques affect healing?; 2) what affect does each of the early tendon transfer techniques have on subsequent ossification?
To answer these questions, we utilized a previously described porcine model 12 to compare the histological and radiographic effects of tendons transferred using metallic suture anchors (new technique), suture fixation (similar to that described for vertical talus) and the classic bone tunnel (as described for clubfoot) to both ossified and unossified bone. Our null hypotheses was that no differences in histological healing or radiographic appearances will be found between fixation techniques. The purpose of this work was to increase our current understanding of the science behind these commonly performed paediatric transfers, in hopes to help guide the surgeon's choice of tendon fixation technique(s) in various clinical scenarios involving very young patients.
Materials and methods
Nine newborn (< 48 hours of age) mixed breed piglets 12 were anesthetized, placed in a prone position and the lower extremities prepped and draped for surgery. A midline posterior incision was performed extending proximal to the os calcis distal towards the midfoot. Posterior dissection was carried down until the flexor digitorum superficialis (FDS) was identified crossing superficial to the tendo-achilles. The FDS was freed from the underlying tendo-achilles then followed and dissected free from the surrounding soft tissues distally to the level of the metatarsals. The individual tendon slips were then transected. Single tendon slips were then transferred to either the unossified calcaneal apophysis (left) and/or through the ossified calcaneal body (right) as indicated by the specific procedure. All tendons were fixed under direct vision of the cartilaginous apophysis and boney calcaneus without radiographic imaging. Following all surgeries, piglets were recovered, and were returned to their sow, without any weight bearing restrictions or immobilization. Animals were euthanized and hind limbs collected for analysis at six weeks.
Procedures
Suture anchors
The FDS tendon was harvested as described above. A size 1.3-mm suture anchor (Micro Quickanchor, Titanium, 4-0 Orthocord; (Mitek/DepuySynthes, Raynham, MA, USA) was used to fix one slip of the FDS tendon to the medial surface of either the cartilaginous apophysis or boney calcaneal body via a Krackow type stitch run ∼2 cm high in the tendon (Fig. 1).
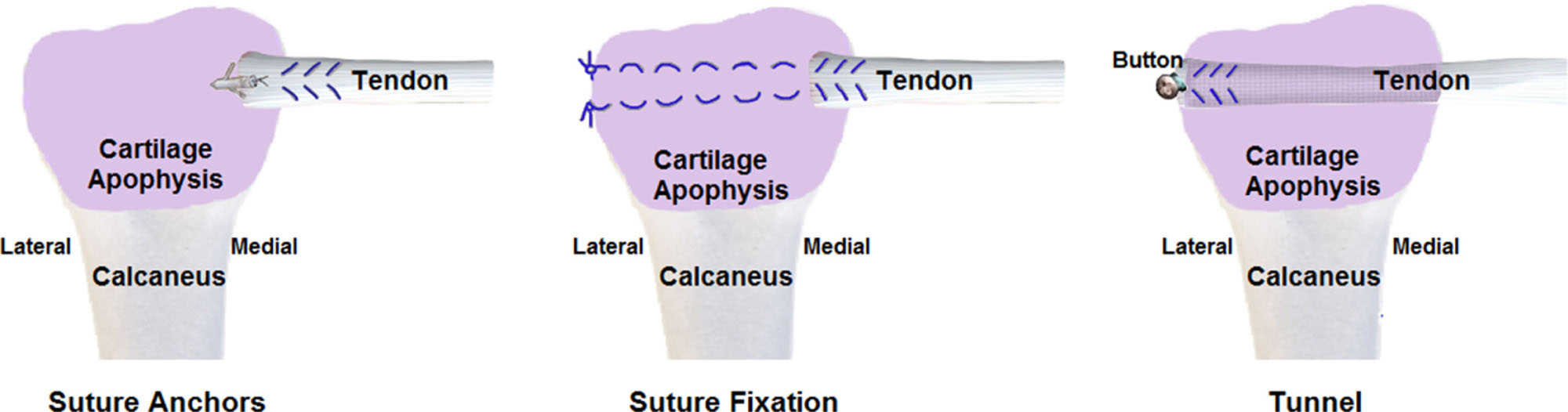
Illustration of tendon transfer techniques performed in this study. Matching osseous transfers were also performed through the ossified calcaneal body (not shown).
Suture fixation
The same sutures used in the suture anchors (4-0 Orthocord, Depuy Synthes, Raynham, MA, USA), were used to fix tendons in the same manner with a Krackow stitch. The attached needle was then used to pass the suture arms through either the apophysis (left side) or ossified bone (right side) without creating an expanded tunnel within the calcaneus. The tendon was then brought apposition to the medial surface of the calcaneus, without pulling the tendon into or below the medial surface of the calcaneus. The suture arms were then tied over the cartilaginous or boney block on the lateral side of the calcaneus (Fig. 1).
Classic tunnel
The non-absorbable suture (4-0 Orthocord, Depuy Synthes, Raynham, MA, USA) was also placed using a Krackow stitch in this cohort. However, an 18-gauge syringe needle was then used to create a tunnel, either through the cartilaginous apophysis (left side) or through the ossified body of the calcaneus (right side). The free ends of the running suture were then placed through the syringe needle in a medial to lateral fashion. The tendon was then pulled through the tunnel (created by the 18-gauge needle) exiting the lateral side of the calcaneus and held in place by tying a custom stainless steel button to the free end of the tendon slip, resting on the lateral side of the calcaneus. No excessive tension was applied to any of the tendon transfers. Wounds were closed in a non-layered horizontal mattress fashion using large gauge monofilament suture (#2 Prolene; Ethicon, Rariton, NJ, USA) due to rapid animal growth and tensile strength needed to maintain closure and recovered as described above (Fig. 1).
Calcaneal processing
The calcanei of all nine animals were harvested at six weeks of age. To evaluate any disturbances in the ossifiction of the calcaneal apophyses, lateral images of the calcanei were taken utilizing high resolution Faxitron imaging (UltraFocus Digital Radiography System with DXA; Faxitron, Tuscan, Arizona). The calcanei samples were then sectioned in the sagittal plane and fixed in neutral buffered formalin for three days, followed by decalcification in 15% EDTA for two to three weeks. The anchors, buttons and pin tips were then removed. Finally, the samples were processed through to 70% ethanol and embedded in paraffin, and 5-µm sections were taken. Sections were stained with hematoxylin-eosin and Masson's trichrome and viewed using both transmitted and polarized light.
Histological analysis
A semi-quantitative grading system, 12 was used to grade healing at the enthesis. This is an aggregated scoring system with values ranging from 0 (poor) to 15 (excellent) enthesis healing (Table 1). Scoring was carried out by an experienced musculoskeletal histopathologist (M.D.) and another co-author (S.B.). Because the type of fixation was clear on histology, the authors were not able to be blinded when assessing the samples. Due to the low sample size (n = 3) in each cohort only descriptive statistical mean scores and ranges were performed.
Histological grading scheme utilized in assessing tendon transfer healing

Scoring the radiographic appearance of the calcanei
The radiographic images were deidentified and provided to five independent readers who graded the apophyseal appearance using a modified one to four grading system previously described 12 (Fig. 2; supplementary material). Each reader scored each image in triplicate at three separate settings.
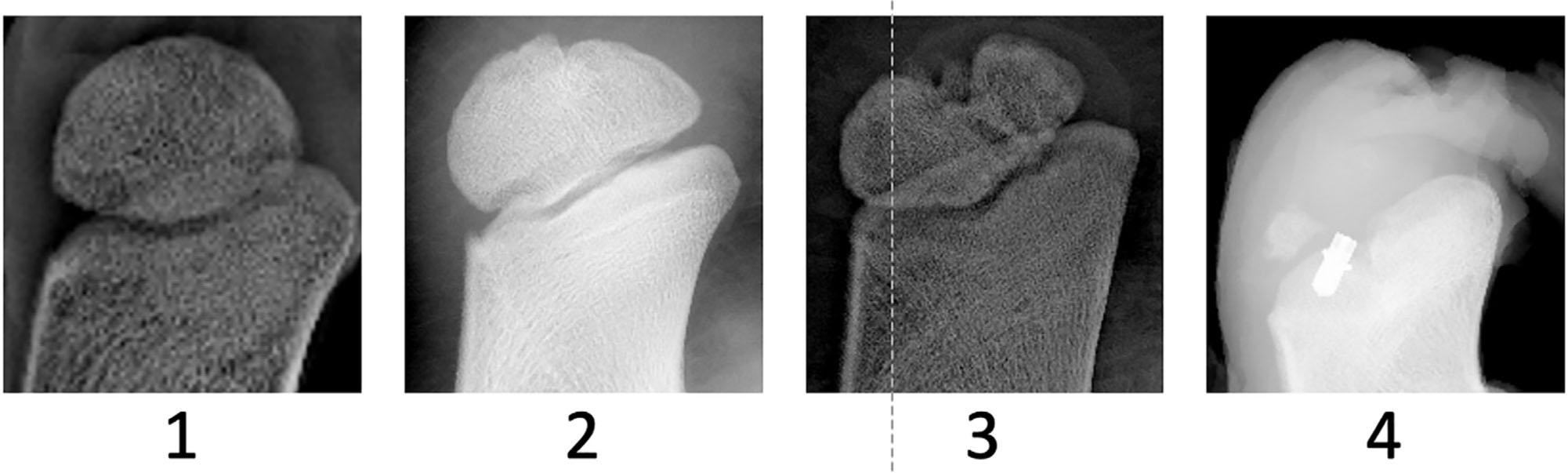
Representative examples of each of the radiographic scores utilized for samples in this study.
Statistical analysis
A descriptive analysis reporting the overall mode of modes (most common reported score for each sample) and percentage agreement between the five raters score for each sample were reported.
Results
Histology results
Suture anchors
In tendon suture anchored to bone and cartilage (mean overall scores 5.7 (range 5-7 for bone; 3-8 for cartilage) out of 15, for both), there was poor inter-digitation (< 50%) of the tendon fibres into the bone and cartilage interfaces, respectively. In both groups, the tendon fibres appeared disorganized with low collagen fibre density.
Suture fixation
When tendon was sutured to bone (meanoverall score 7.3 (range 7-9) out of 15), the samples exhibited medium-good (25% to 100%) inter-digitation at the bone-tendon interface, however, collagen fibres were disorganized with only medium collagen fibre density. Interestingly, when tendon was sutured to cartilage healing was improved (meanoverall score 10.3 (range 8-12) out of 15), and the group exhibited medium-good (25% to 100%) inter-digitation at the cartilage-tendon interface with medium collagen and moderate orientation scores in the tendon.
Tunnel fixation
When tendon was passed through a bone tunnel meanoverall score 9.3 (range 8-11) out of 15), the samples exhibited medium (50% to 74%) inter-digitation bone-tendon interface with moderate alignment and medium collagen density. A periosteal reaction and periosteal thickening was observed around the site of the bone tunnel. Similarly, when tendon was passed through a cartilage tunnel (meanoverall score 10.3(range 10-11) out of 15), these samples exhibited medium (50% to 74%) inter-digitation bone-cartilage interface with moderate alignment and medium-high collagen density. A periosteal reaction and periosteal thickening was observed around the site of the cartilage tunnel.
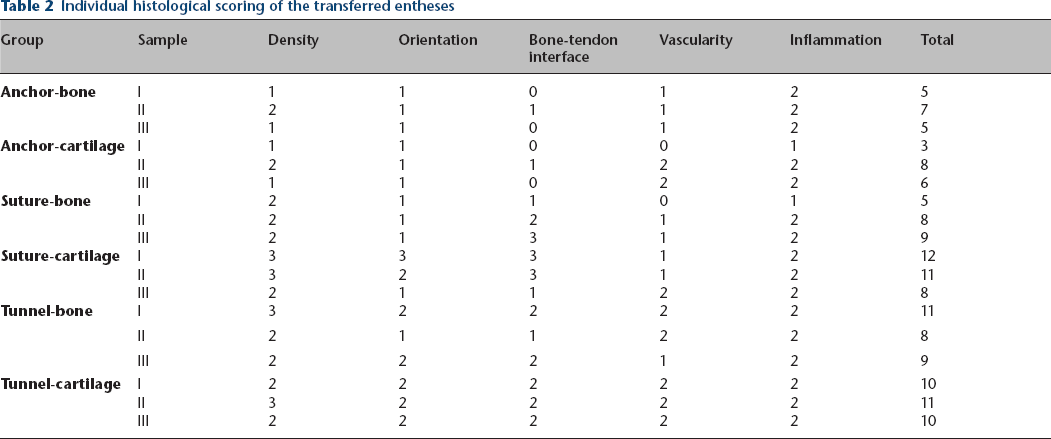
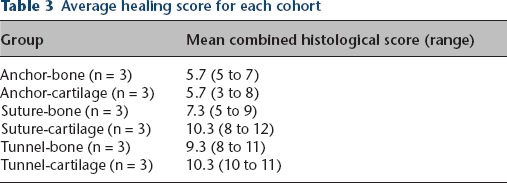
Examples of poor and good histological healing can be found in Table 2. Examples and summary of the individual histological scoring is found in Figure 3 and Table 3. Representative histological findings for each cohort is found in Figure 4.
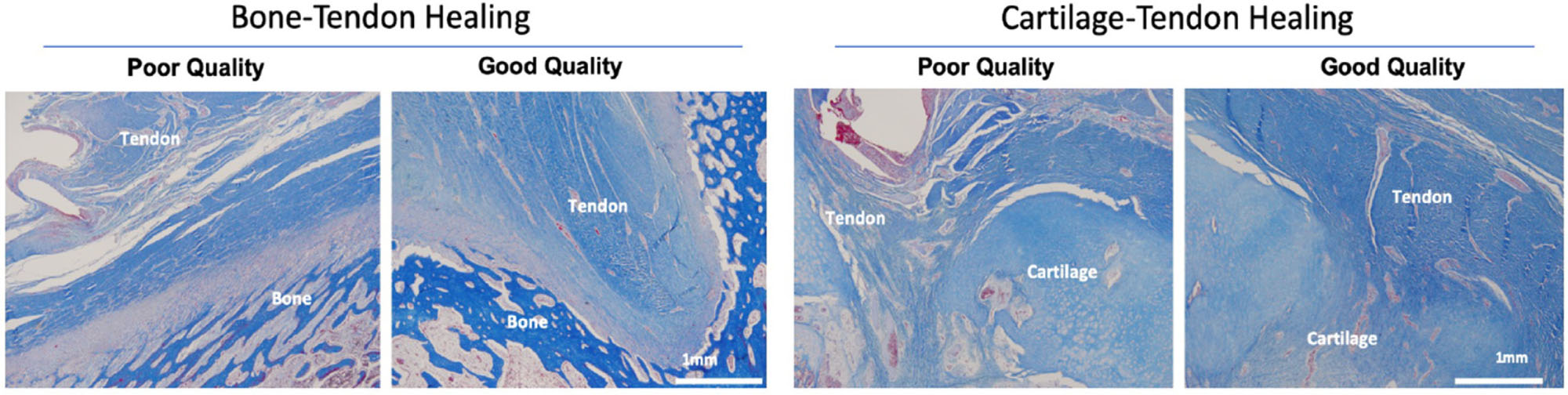
Histological examples of good and poor histological healing. The poor healing samples (left in each pair) demonstrate low collagen fibre density, disorganized alignment, poor inter-digitation and abundant vascularity, whereas the good healing samples demonstrated moderate-high collagen fibre alignment, medium fibre density, good inter-digitation and minimal vascularity.
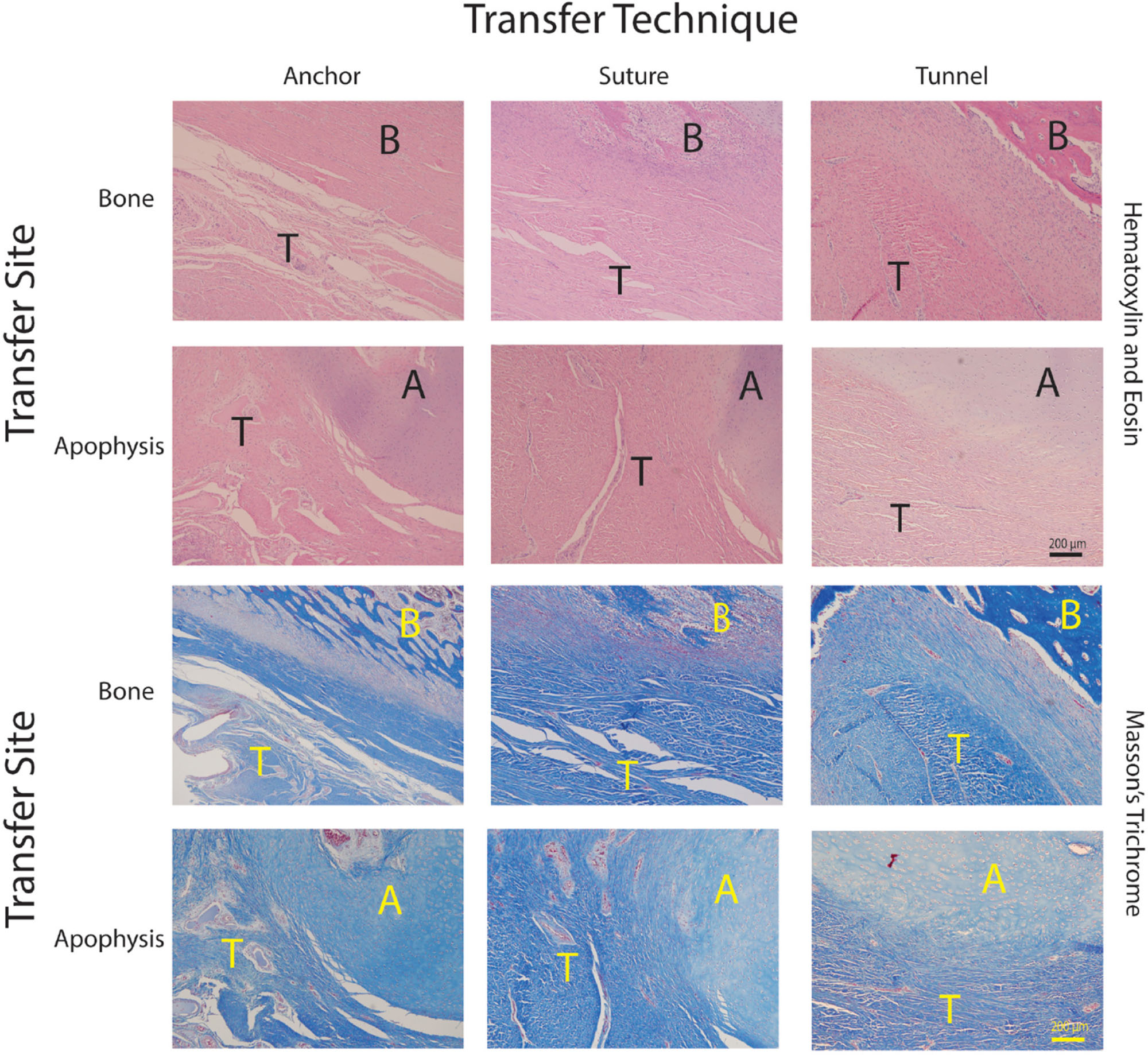
Representative summary of the histological findings for each cohort. Images at 100X, top pair Hematoxylin/Eosin, bottom pair Masson's Trichrome. Bone transfer site shown above apophyseal cartilage insertion site in each column for each fixation method (T, tendon; B, bone; A, apophyseal cartilage). Suture anchor (left column): tendon to bone (top) exhibited disorganized fibre orientation with poor (< 25%) inter-digitation at the bone-tendon interface and abundant vascularization. Tendon to cartilage (bottom) exhibited disorganized fibre orientation with poor (< 25%) inter-digitation at the bone-tendon interface and abundant vascularization. Suture fixation (middle column): tendon to bone (top) exhibited medium-good (25% to 100%) inter-digitation at the bone-tendon interface, however, disorganized fibre orientation with low-medium collagen fibre density whereas tendon to cartilage (bottom). The group exhibited medium-good (25% to 100%) inter-digitation at the cartilage-tendon interface with medium collagen and moderate orientation scores in the tendon. Tendon tunnel (right column): tendon to bone (top) exhibited good (50% to 74%) inter-digitation at bone-tendon interface with moderate alignment and medium collagen density as did tendon to cartilage (bottom) where the group exhibited grade 2 (50% to 74%) interdigitation bone-cartilage interface with moderate alignment and medium-high collagen density.
Individual histological scoring of the transferred entheses
Average healing score for each cohort
Radiographic results
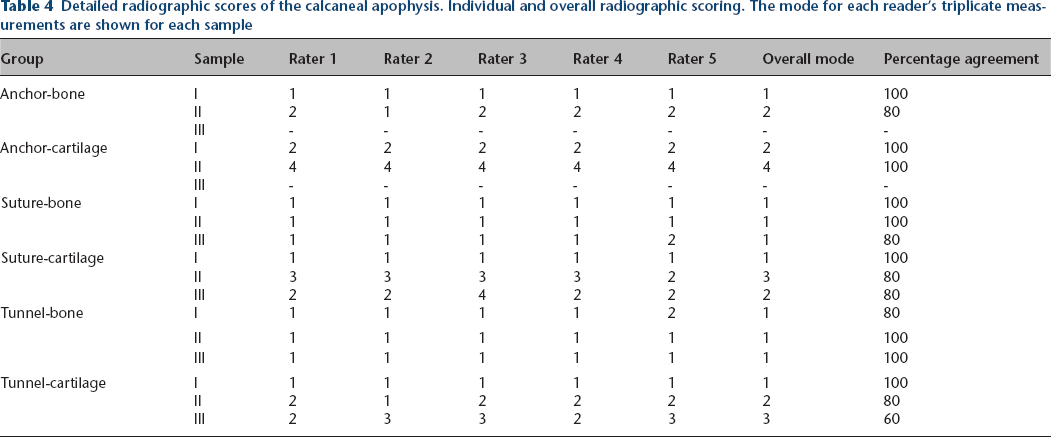
In all, 16 of 18 samples were available for radiographic review. The digital images of one animal (suture anchor), were unfortunately erased from the institutions data system, prior to being scored. An overall rater agreement of ∼90% was found using the four-point scoring system with 100% agreement in nine samples, 80% in six samples and 60% in one. The mode of the readers’ individual scores, overall mode and percentage agreement are shown (Table 4). Ossification of the calcaneal apophysis was minimally affected following transfers to the boney calcaneal body regardless of technique, while apophyseal sutures and tunnels had similar varying effects, and apophyseal achors demonstrated the most severe disruption (Table 4).
Detailed radiographic scores of the calcaneal apophysis. Individual and overall radiographic scoring. The mode for each reader's triplicate measurements are shown for each sample
Discussion
The findings in this study provide histological evidence that a tendon transferred to an ossified bone (as has been recommended classically in clubfeet) or to an unossified bone (cartilage) can heal quite well. However, the tendon fixation technique can make a difference on the enthesis healing. In both the ossified and unossified bones, the use of suture anchors demonstrated the poorest histological healing. In agreement with the previously described clinical procedures in clubfoot and vertical talus, the classic tunnel technique appeared best in ossified bone (as is commonly used in the standard tibialis anterior transfer to the cuneiform), whereas suture fixation (described in the vertical talus) appeared just as good to the tunnel technique in the unossified bone. Our data suggests that each fixation technique affects subsequent ossification in the unossified bone, but that the suture anchor had the most severe effect.
In addition to answering a scientific curiosity, the results of this study provide valuable information that may help guide earlier surgical interventions, as earlier correction of muscle imbalances might prevent structural deformities from developing. While the Ponseti method has become the treatment of choice for idiopathic clubfoot treatment,13–17 its success in maintaining deformity correction is dependent on long-term brace compliance. 18 Even in Ponseti's own hands, up to 40% of children treated required tibialis anterior tendon transfer (TATT).11,19 In our previous clinical work, we have found brace tolerance and compliance to be difficult in our, non-Iowa, non-American population.20,21 As a result, we have considered exploring the novel surgical approaches after casting to prevent recurrences that might provide families with an alternative to bracing. Similarly while the Ponseti method can obtaincorrection in non-idiopathic clubfeet, most clinicians struggle to maintain correction despite bracing.22–29 Potentially earlier and better balancing of forces may provide longer lasting corrections. While TATT is clearly not a panacea that corrects every relapse, 30 understanding how to safely perform such transfers at a young age is the first step in exploring any alternative treatment protocol. Outside of clubfeet, these findings may have similar implications in other pathologies, i.e. brachial plexopathy, that abnormal muscle imbalances cause underlying skeletal deformities that might be avoided with earlier intervention, however, further investigation is needed.
Limitations of this study should be pointed out. Firstly, the sample sizes for each technique are too small (n = 3) to clearly define which method of tendon transfer results in the ‘best’ healing with the ‘least’ apophyseal injury, and do not allow more than a descriptive statistical analysis. However, even with these limited numbers, our findings suggest that suture anchors should not be used for fixation as it demonstrated the poorest histological healing of all the techniques and the lowest radiographic score (despite loss of one image). Apophyseal tunnel and suture techniques were found to alter subsequent apophyseal ossification to varying degress, with less disruption of ossification in the tunnel cohort than would have been expected from our previous report. 12 This could be the result of examining the bisected calcaneii (including both histological and radiographic imaging of the samples) in the previous study and imaging of intact calcaneii in the current study. Despite assessing histological healing in the current study, we did not assess the mechanical properties of the transfers which will be important clinically. Future work will focus on the technique (tunnel versus suture) that produces the best mechanical result and has the least impact on final apophyseal ossification.
In closing, this work provides histological support for findings in previous investigations that have clinically demonstrated that tendons can heal to unossified bones. These data also show that tendon fixation technique affects both enthesis healing and subsequent ossification. However, just because tendons can heal to unossified bones, the authors do not mean to suggest that they should be clinically transferred earlier. Further investigation is necessary to understand the ultimate mechanical and ossification effects of the procedures and to determine in whom earlier tendon transfer might clinically benefit.
Footnotes
Acknowledgements
None of the authors have a conflict of interest with this work.
SB: Histologically scored tendon healing, Radiographically-scored calcanei, Histological figure preparation, Writing, Editing.
EL: Helped in tissue preparation, Histological processing, Radiographically-scored calcanei.
TC: Oversaw animal surgery/recovery/processing, Critical review/edit of manuscript.
MD: Histologically scored and interpreted histological tendon healing, Critical review/edit of manuscript.
HC: Radiographically scored calcanei, Critical review/edit of manuscript.
MW: Radiographically scored calcanei, Critical review/edit manuscript.
MAH: Oversaw project beginning to end, Mentored KK, Collated and presented data, Writing, Editing.