
Abstract
Purpose:
Clubfoot is a common disabling condition that is prevalent across all populations. Approximately, one out of 750 children globally suffers from clubfoot, and around 150,000 to 200,000 children are born with clubfoot every year with 80% of the cases occurring in developing countries. Clubfoot can result in mobility impairments when not properly managed and researchers have argued that understanding knowledge and perceptions are key components to early identification and effective management of clubfoot. The study explored the barriers to clubfoot management from the perspectives of caregivers and healthcare providers in Duayaw Nkwanta, Ghana.
Methods:
A total of 26 participants made up of 22 caregivers of children with clubfoot and six healthcare providers were purposively sampled for the study guided by a set of inclusion and exclusion criteria. Qualitative data were collected using a semi-structured interview guide through in-depth face-to-face interviews. Interviews were transcribed and analyzed thematically and presented as findings.
Results:
High cost of treatment, long travel distance, long hours spent at the treatment facility, non-availability of clubfoot treatment services, late reporting of clients for treatment, and non-compliance of parents/caregivers with treatment protocols were identified as the barriers to effective management of clubfoot.
Conclusion:
These findings have substantial implications for current interventions to effectively manage clubfoot in Ghana.
Introduction
Clubfoot is a common disabling condition that is prevalent across all populations. 1 It is a complex congenital deformity of the foot characterized by adductors, cavus, varus, and equinus. Although the exact cause of clubfoot is unknown, some studies attribute it to genetic and environmental factors.2,3 The strongest risk factor is documented to be the male sex with a ratio of 2:1 affectation.4,5
Globally, research suggests that the prevalence rate of clubfoot is 1 per 1000 live births, although there are variations found between different races and ethnic groups.2,4 In the United States, an overall prevalence rate was found to be 1.29 per 1000 live births out of which the white population recorded 1.38 while Hispanic and non-Hispanic blacks recorded 1.30 and 1.14 per 1000 live births, respectively. 6 Based on the incidence of clubfoot in Sweden of 1.4 per 1000 newborns, 7 it is estimated that 200–300 children with 1 or 2 club feet are born in the Netherlands every year. 8 In addition, the prevalence of clubfoot varies across ethnic populations, from 0.39 cases per 1000 births in Chinese populations to 7 cases per 1000 births in Hawaiians and Maoris. 9 A recent study estimated clubfoot birth prevalence in lower-middle-income countries to be 1.11 (0.96, 1.26) in Africa, 1.74 (1.69, 1.80) in the Americas, 1.21 (0.73, 1.68) in South-East Asia (excluding India), 1.19 (0.98, 1.40) in the Eastern Mediterranean region, and 0.94 (0.64, 1.24) in the West Pacific (excluding China). 3
In sub-Saharan Africa, a study by Smythe et al. 3 found a pooled prevalence of 0.96 to 1.26 per 1000 live births. Studies show relatively higher rates in some countries such as South Africa and Nigeria recorded at 3.5 and 3.4 per 1000 live births, respectively.10,11 The incidence of clubfoot in Malawi has been reported to be two to three per 1000 live births. 12 A study conducted in Uganda estimated clubfoot prevalence to be relatively lower at 1.2 per 1000, with the male:female ratio of prevalence being 2.4:1. 13
Studies on the occurrence and prevalence of clubfoot are limited in Ghana. Boakye et al. 14 reported a relatively lower prevalence of clubfoot at 1.2 per 1000 live births. A more recent study in Northern Ghana estimated the prevalence at 0.9 per 1000 live births.
Research suggests that first-born babies are more at risk, and it can affect one foot (unilateral) or both feet (bilateral) in almost equal proportions. 15 The prevalence rate of clubfoot in sub-Saharan African countries such as Ghana highlights the need for effective management and/or strategies to curb clubfoot occurrence. Indeed, effective management of clubfoot could help address the stigma, discrimination, and social exclusion of children with clubfoot. 16 Moreover, effective management of clubfoot is identified as important for resolving the personal, social, and economic consequences of the condition to families. 17
Despite this, empirical evidence highlights some barriers to the treatment of clubfoot. Bedford et al. 18 found parental knowledge of the condition and available treatment, socio-economic problems, negative attitude of family members, and non-availability of logistics as significant barriers to the effective management or treatment of clubfoot. Also, a study by Alsiddiky et al. 19 identified a lack of knowledge about the condition and low awareness campaigns as the major hindrances to effective clubfoot treatment. In another study, the culture and beliefs of patients were found to be strong barriers to clubfoot management. 20
However, within the Ghanaian context, there is scarce literature from the perspective of parents/caregivers and healthcare providers directly involved in child deliveries, referrals, and treatment of clubfoot on the barriers to clubfoot management. Available studies have mainly focused on establishing the prevalence of clubfoot, 5 as well as the clinical treatment outcomes of the Ponseti method in the management of clubfoot. 14 Therefore, this study sought to address the identified gap in knowledge regarding the barriers to the effective management of clubfoot, from the perspectives of parents/caregivers and health care providers in Duayaw Nkwanta, Ghana.
Methods
A case study design was employed using a qualitative approach to conduct the study on the barriers to clubfoot management. The study population comprised parents/caregivers of children with clubfoot and healthcare providers directly involved in deliveries, referrals, and treatment of clubfoot cases. The sample size for parents/caregivers of children with clubfoot was drawn from the registry of patients attending the Clubfoot clinic in the orthopedic department of the St John of God Hospital, Duayaw Nkwanta. This hospital was chosen because it provides the right respondents, that is, parents/caregivers and healthcare providers required to achieve the objectives of the study.The decision to conduct this study at the hospital was informed by the fact that a significant percentage of children with clubfoot visit the clubfoot clinic for rehabilitation and other interventions regularly. Twenty-two parents/caregivers of children with clubfoot and six healthcare providers, made up of one each of the following categories: a medical doctor, a physiotherapist, a physiotherapy assistant, a midwife, a community health nurse, and a health counselor were also selected for the study. This brought the total number of respondents to 28.
Purposive and simple random sampling methods were used to recruit respondents. A purposive sampling technique was used to select the population setting and it is a type of non-probabilistic sampling method that is drawn from that part of the population that is close at hand and who was appropriate for the study based on the sound judgment of the researcher. Hence, purposive sampling method was employed in arriving at the selection of the clubfoot population. The simple random sampling method provided an opportunity where each member of the population got an exactly equal chance of being selected. This method was used to recruit the parents/caregivers from the register at the clubfoot clinic and the healthcare providers for the study. The healthcare providers included individuals who provide rehabilitation and other interventions to children with clubfoot at the clubfoot clinic.
The researchers conducted two in-depth face-to-face interviews using a semi-structured interview guide to collect data from the parents/caregivers of children with clubfoot and the healthcare providers at the clubfoot clinic or homes of parents/caregivers depending on where they preferred the interview to take place. Each interview with a respondent took 30-45 min until a point of saturation was reached. The interviews were conducted in the English language; however, a special interpreter was hired to interpret for respondents who had difficulties speaking and understanding the English language for clarity and understanding. Overall, the researchers used 3 months for the interviewing and data collection. The interviews were audio-taped and recorded along with field notes. The recorded interviews were transcribed into written forms. Transcripts were organized into dominant themes that were obtained from the questions that were asked. The themes were examined in duplicates with each examiner unaware of the summary of the other. The researchers divided themselves into groups of two to read a selected number of transcripts and both members of each group were made to read all the transcripts independently. The entire team then met to discuss prominent themes and to find a solution to the coding disagreement. One team member read all the transcripts and led the discussion. The transcript was divided into sections that helped in the management of the data. The summaries from each team were compared with the others, and differences among their summaries were resolved. Direct quotations of some of the responses have been presented in the findings. Overall, there were increased agreement levels of explanations and emphasis among authors.
Results
Demographic characteristics of respondents
A total of 28 participants who took part in the study which comprises 22 parents/caregivers of children with clubfoot and 6 healthcare providers. The majority (8), of the parents/caregivers, were aged between 41 and 50 years with females (18) recording the highest number. Among the children with clubfoot whose parents/caregivers responded to the questionnaire, the majority (12) were aged below 6 months with males (14) recording the highest number among children with clubfoot. An equal number of the healthcare providers (two) have between 1–2 years and 5–7 years of practice experience, respectively, as summarized in Table 1.
Respondents’ demographic characteristics.
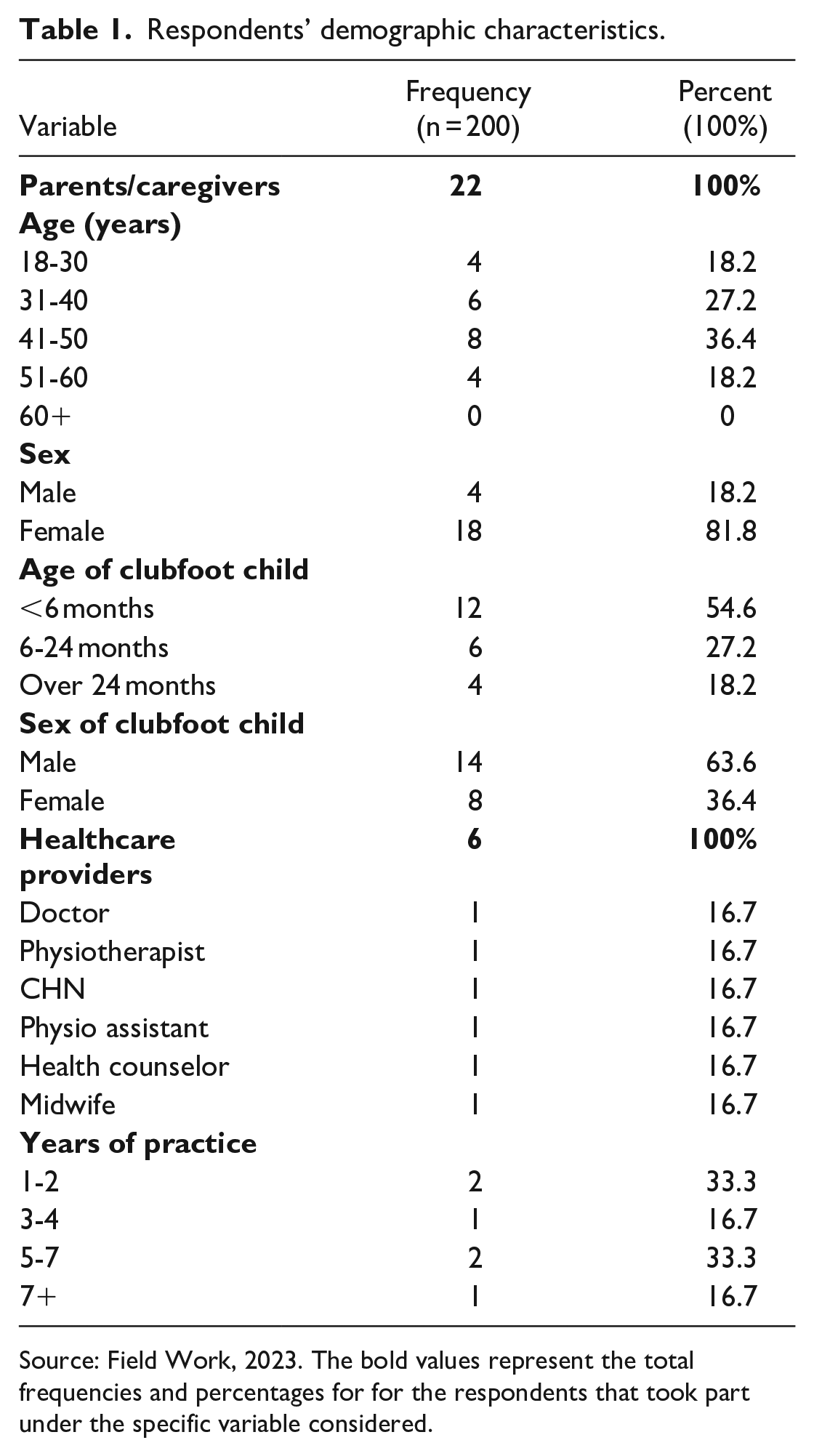
Source: Field Work, 2023. The bold values represent the total frequencies and percentages for for the respondents that took part under the specific variable considered.
Perspectives of parents/caregivers on barriers to clubfoot management
The study found that parents/caregivers of children with clubfoot faced three major challenges in their quest to seek effective management and treatment for their children. The cost of treatment, travel distance transportation discomfort to the health facility, and the long hours spent at the treatment facility were the challenges they faced. These challenges according to the respondents, limited their ability to access quality healthcare management for their children with clubfoot.
Cost of treatment
High treatment cost was found as a major barrier to effective management of clubfoot in the study area. This includes the cost of consultation, casting materials, physiotherapy services as well as surgery if the need arises. To make matters worse, some female parents/caregivers also indicated that their partners did not support them financially in meeting the cost of treatment for their children with clubfoot. The situation is exacerbated by the non-availability of free clubfoot treatment services in major hospitals such as Teaching and Regional Hospitals, following the termination in July 2019 of a partnership between Cure Clubfoot Ghana—a non-governmental organization (NGO) and the Ghana Health Service. As a result, parents have to pay for full treatment since clubfoot is not covered by the National Health Insurance Scheme of Ghana:
. . . Even though the cost of treatment is covered by the NGO, I have to cover the cost of transport and payment for a guest house. This has a big toll on my finances, as the time spent on my child’s treatment does not allow me to work. (parent, individual interview) . . . the health insurance is also a huge problem for me, it does not cover the cost of treatment for clubfoot at least I would have managed with that. (parent, individual interview)
Long travel distance and transportation discomfort
Some parents/caregivers also shared the view that the long travel distance from their various villages to the healthcare facility was a huge barrier to the effective management of their children’s clubfoot. Parents/caregivers highlighted the fact that the treatment center was located at a far distance from their homes and villages. They revealed that they experienced transportation difficulties and discomfort due to the bad road network and drivers charging huge amounts of money due to the bad roads. They also expressed discomfort in carrying their children who are unable to walk in a limited-space vehicle and sometimes the unwillingness of some passengers to cooperate with them. As a result, they preferred staying home to avoid these discomfort and difficulties:
. . . I travel with my two-week-old baby from Agona Swedru to this place. We usually pick up about two to three different buses before we arrive at the treatment center. When I set off in the morning, I get to Duayaw in the evening spending about 7-9 hours on the road. Aside from the stress involved, the cost of transportation is high for me. (parent, individual interview) . . . sometimes some passengers do not recognize that we are carrying a sick child to give the benefit of the doubt. Asking them to push or adjust to create space for you is always met with bad comments. On top of this, the road network from my place to the facility is very bad so I would prefer not to go at all. (parent, individual interview)
Long hours spent at the treatment facility
Some of the participants indicated that they spend long hours at the treatment facility waiting to be served. They reported this as a challenge since it discourages them from visiting the facility regularly as indicated on their appointment sheet. They further revealed that the long hours get them tired making it very difficult for them to visit the subsequent days on appointments. Also, they revealed that due to the long hours, they tend to only visit the facility for treatment on their free days and not regularly as indicated on the appointment sheet:
. . . It’s very sad here since this is the only facility involved in clubfoot management, the is always a long queue that you have to wait several hours before you will be served. (parent, individual interview) . . . For me, I skip most of my appointments because of the stress of waiting for long hours to have my baby attended to, and then you are booked to come for the next two days. I find it difficult following the appointment but I try to do what I can. (parent, individual interview)
Perspectives of healthcare providers
From the perspectives of the healthcare providers, the study revealed three major barriers to the management of clubfoot in their facility. The respondents reported inadequate trained health personnel and absence of alternative treatment methods, late reporting of clubfoot cases for treatment, and the non-compliance of treatment protocols as the barriers to effective management and treatment of clubfoot. These barriers, according to the respondents, limited their ability to provide quality healthcare management and treatment for clubfoot in children.
Inadequate trained health personnel and absence of alternative treatment methods
The respondents revealed that the hospital has only one orthopedic surgeon who conducts the clubfoot surgeries and tenotomy for children with tight Achilles tendons to complete the final phase of casting to improve ankle dorsiflexion and, in addition, conduct all other orthopedic procedures in the hospital. This situation has led to the booking of clients who have to wait for several weeks and months to have their surgeries or tenotomies done. The respondents further revealed that rehabilitation professionals such as physiotherapists and occupational therapists involved in the management and treatment of clubfoot are woefully inadequate at the hospital. This, in their view, has led to a higher patient-to-practitioner ratio making it difficult to achieve intended treatment outcomes. The findings further indicated the non-availability of other treatment services besides the Ponseti method as a major barrier affecting the treatment and management of clubfoot. Healthcare providers who participated in the study said the Ponseti method is the only method used at the St. John of God Hospital in Duayaw Nkwanta. This treatment method according to the respondents is the current global gold standard for the treatment of clubfoot and has shown tremendous results. The respondents, however, indicated that the surgical method is rarely used in contemporary times in the management of clubfoot although it also proves to be effective sometimes:
. . . here, we only mostly use the Ponseti method in managing and treating clubfoot. The orthopedic surgeon here is only one and rarely sees clubfoot cases due to the caseload he has to attend to. (healthcare provider, individual interview) . . . We need the professionals, at least one more orthopedic surgeon, more physiotherapists, and occupational therapists as well. I believe when they come on board we will record improvement in clubfoot care and management. (healthcare provider, individual interview)
Late reporting of clubfoot cases for treatment
The late reporting of clubfoot cases for treatment by parents/caregivers was found as a major barrier to treatment according to the healthcare providers who took part in the study. This is because, according to the respondents, the feet of these children become very difficult to mobilize and manipulate when they grow older, especially after 2 years of age. This, according to the respondents, explains why late reporting of clubfoot cases constitutes a major barrier to the effective management of clubfoot. The healthcare providers were of the view that, for effective treatment of clubfoot, it must start as early as possible preferably before children start crawling or walking (from birth to about 6 months), or else it reduces better treatment outcomes:
. . . Some parents/caregivers who have children with clubfoot prefer to try herbal medication and only come to the hospital if it does not work. (healthcare provider, individual interview) . . . Sometimes it’s sad that by the time they report the condition might be complicated and there’s little you can do. Clubfoot is such that there are better treatment outcomes if the parents report to the facility within the first 6 months but sometimes they report when the condition gets worse. (healthcare provider, individual interview)
Non-compliance with treatment protocol
Non-compliance to treatment protocols on the part of parents and caregivers was also revealed by healthcare providers as a challenge that has undesirable impacts on the treatment of clubfoot. Some healthcare providers shared that some parents/caregivers did not comply with treatment both at the casting and bracing period. After casting, health workers indicated advising parents/caregivers to prevent the Plaster of Paris (POP) from getting wet. However, this was often not adhered to by parents/caregivers especially during the bathing of children, thus resulting in the POP breaking down. To compound the situation, because most parents/caregivers of children with clubfoot live far from treatment centers, they often have to wait until about a week or more to report to the hospital, which sets back children in their treatment phases because the POP loses its tension and cannot hold the manipulated feet in place. Recurrence was also mentioned by some healthcare providers as a further challenge to non-compliance to the treatment protocol. They emphasized that, in situations where parents/caregivers relax on treatment protocols, especially at the bracing phase, some children get recurrent clubfoot. This, they revealed, is because parents get excited when they notice signs of feet being corrected, and as such, do not continue wearing the brace for the required time, making the condition relapse. In other instances, some healthcare providers reported that some parents forget that the condition is congenital and could relapse if they do not continue the use of the brace till the right time:
. . . Some of the parents do not adhere to the advice we give them, P.O.P for instance are not supposed to come into contact with water but parents will report to the facility with the P.OP removed because it has come into contact with water, in cases, it’s not removed, you will see that it has lost its tension and cannot hold the manipulated foot in place. (healthcare provider, individual interview) . . . The parents/caregivers normally skip treatment by missing and failing to come on the right appointment days, they complain of the distance to the healthcare facility, it’s a huge challenge to treatment outcomes. (healthcare provider, individual interview)
Discussion
Several studies have revealed the cost of treatment as a major challenge for parents/caregivers of people living with clubfoot experience.21,22 The outcome of these studies corroborates with the findings from this study which revealed that caring for children with clubfoot had a toll on the finances of parents/caregivers. Given this, caregivers find it difficult to bear the cost of treatment for children with clubfoot. A similar study conducted in Malawi reported that disability in clubfoot leads to dependency on another individual within the family, which has a great impact on financial and socio-economic status. 23 This makes parents/caregivers resort traditional medicine that are not effective and consequently complicate their condition. The long-distance travel and transportation difficulties also posed a critical barrier to the management and treatment of clubfoot in the healthcare facility. Caring for children living with clubfoot was found to be time-consuming, with distance being a further constraint, especially for working parents/caregivers who may have to visit healthcare facilities frequently for reviews. A similar study conducted in Uganda also revealed that the overwhelming majority of parents indicated that they found it expensive to bring their children for plaster-casting every week. 24 Majority of the participants were found to travel long distances to seek treatment for their children with clubfoot. In Ghana, clubfoot services are limited to specific geographical areas. The Komfo Anokye Teaching Hospital in Kumasi, for example, and the few public facilities that provide clubfoot services in the middle and northern sectors often are located in big cities and towns. This means parents/caregivers travel long distances to access quality care for their children with clubfoot and often skip appointment days due to distance for treatment and reviews. Parents and caregivers who traveled short distances were more compliant with treatment. 25 Again, the bad nature of roads from the rural areas to the healthcare facility poses health risks and lots of inconveniences for parents when commuting to the treatment facility with their children for treatment. A previous study conducted in Kenya reported that the effect of distance from a service facility was evident as expected, especially considering the lack of transport and bad roads. Travel distance and bad roads further impede frequent treatment and reviews. The lack of frequent treatment and reviews has a tremendous impact on effective treatment and management outcomes. This finding is consistent with several studies that found traveling distance to a health facility as a barrier to the treatment and management of clubfoot.20,26,27 Also, Beardsley et al. 28 reported in his study that, as the economic costs of treatment attendance increase with distance, the ability of clients to continue treatment diminishes.
Another barrier to the management and treatment of clubfoot is the long hours they spend at the treatment facility. Parents spend so much time at the care facility to the detriment of their livelihood and economic activities. This finding was confirmed by the healthcare providers that there inadequate personnel with the specialties involved in the treatment and management of clubfoot hence only a few practitioners attend to a lot of patients. The long wait could be due to the heavy caseloads of the hospital as it is the only public health facility in the district that offers treatment for clubfoot and specialist care. These findings agree with the work Kingau et al. 25 conducted among clubfoot patients in Kenya which reported that the number of clinics is not enough for the effective management of clubfoot leading to overcrowding and longer waiting times. From the perspectives of the healthcare providers on barriers encountered in the treatment and management of clubfoot in their facilities, inadequately trained personnel with the required specialties in clubfoot management and the absence of alternative treatment methods in their facility posed a barrier and obstacle. Surgeons, rehabilitation professionals such as physiotherapists, and occupational therapists who are involved in the management and treatment of clubfoot are woefully inadequate in the hospital. The lack of alternative treatment services besides the Ponseti method at the facility was also revealed as a major barrier affecting the treatment and management of clubfoot. Although the respondents admit the Ponseti method to be the gold standard for the treatment of clubfoot, other methods such as surgery have also been proven to be effective and are rarely performed at the facility. This means the surgical method is not accessible or rarely accessible to parents/caregivers of children with clubfoot; hence, complications that could otherwise be corrected with surgery and other forms of treatment methods other than the Ponseti method were left untreated. This finding is consistent with that of other studies which found the Ponseti method to be the dominant form of treatment for clubfoot, with the other treatment options not readily available and accessible.4,20,29 The finding, however, contrasts with the work of Kingau et al. 25 in Kenya, who reported that, at the Talipes Clinic in Nairobi, service providers are still using more traditional surgical and conservative methods of management of clubfoot. This study further revealed that the late report of clubfoot cases for treatment by parents/caregivers was a barrier for healthcare providers to effectively provide treatment and management services. This suggests that due to the late reportage of clubfoot cases to the hospital for early treatment, the feet of these children become very difficult to manipulate and mobilize when they grow older, especially after 2 years of age. This is due to the complications that set in as the child gets older. In a related study, it was established that regardless of the treatment method, late reporting of patients with congenital clubfoot resulted in the development of abnormalities in the foot structure and function that affect them into adulthood. 30 The works of various researchers have established complications of late reportage of clubfoot cases to include recurrent or residual deformity, pain, limited ankle and subtalar range of motion, and limitation of activities, among others.31 –33 Furthermore, the evidence available in the literature has established that congenital clubfoot should be treated as soon as possible to come up with the most reliable results. 34 Also, effective management should commence at or as near as possible to birth. 26 The aim is to correct the impairment, improve mobility, and thus allow normal social participation.26,35
The study again revealed that non-compliance with treatment protocols by parents/caregivers was a major barrier to the effective management of clubfoot in the study area. Non-adherence may not be limited to only non-compliance with treatment protocols by parents/caregivers but not strictly following the Ponseti regime of intervention by healthcare providers can also affect the treatment and management of clubfoot. According to the healthcare providers, parents were not compliant with treatment both at the casting and bracing stage because some appeared relaxed on treatment protocols especially at the bracing phase, thus resulting in children developing recurrent clubfoot. To make matters worse, clinical attendance was not regular due to the location of treatment centers. The findings of the study indicate that parents and caregivers have a major role to play when it comes to the treatment and management of children with clubfoot to achieve the expected outcome. This view is largely consistent with that of earlier studies which have also documented that parents/caregivers have a major role in the treatment of children with clubfoot.36,37 Their compliance is imperative for achieving good results,38,39 and without the accurate and timely contribution and adherence to treatment protocols, the treatment goals cannot readily be achieved. 25 Suresh et al. 40 confirmed in their work that poor adherence leads to poor treatment results, reoccurrence of the deformity, and the development of more rigid foot deformities that are difficult to correct. The findings of the study and cited literature demonstrate the need for parents/caregivers to strictly follow the treatment regime for clubfoot, and for health professionals to encourage parents/caregivers and their families to regularly attend scheduled treatment appointments despite the challenge of proximity.
Conclusion
The study established some barriers to the effective management or treatment of clubfoot in Duayaw Nkwanta. Sampled parents/caregivers of children with clubfoot and health professionals working in deliveries, referrals, and treatment of clubfoot cases identified the barriers to effective treatment and management as high cost of treatment, long travel distance and transportation discomfort, long hours spent at treatment facilities, inadequate trained personnel and non-availability of clubfoot treatment services, late reporting of clients for treatment, and non-compliance of parents/caregivers with treatment protocols. Because of this, there is a need for effective stakeholder engagements to develop appropriate interventions that will help educate parents/caregivers on clubfoot. Knowledge plays a vital role in how early a parent/caregiver identifies the condition and reports to the appropriate health center for effective management of the condition. Moreover, there is a need to address the high costs of clubfoot treatment. One way of achieving this could be making sure that treatment for clubfoot is covered by Ghana’s National Health Insurance Scheme. In addressing the challenge of inadequate healthcare personnel involved in the treatment and management of clubfoot, the Ministry of Health and its stakeholders such as the Ghana Health Service must train more practitioners with a specialty in clubfoot management to augment the shortfall in the healthcare system. In addition, the long travel distance and transportation discomfort could be addressed by the government through the Ministry of Health by setting up and equipping more treatment facilities for clubfoot in the study area as well as nearby towns. There is also the added need to explore the adoption of other treatment methods for clubfoot such as the surgical method to treat the condition in older children.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241262630 – Supplemental material for The perspectives of caregivers and health service providers on barriers to clubfoot management in Puri-Urban health facility in Ghana
Supplemental material, sj-pdf-1-cho-10.1177_18632521241262630 for The perspectives of caregivers and health service providers on barriers to clubfoot management in Puri-Urban health facility in Ghana by Shariphine Agoalikum, Enoch Acheampong, Peter Bredu-Darkwa and Sandra Bonah in Journal of Children’s Orthopaedics
Footnotes
Author contributions
SA designed the concept and worked on the study protocols. EA worked on the introduction and data analysis. PB-D took part in the field data collection and the write-up of the methods section. SB worked on the results and discussion part of the work also took part in data collection. All the authors have reviewed the work and given their consent for the submission of this article for publication. The authors participated solely in all stages of the study such as in developing the study design, data collection and analysis approach, and compilation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Committee on Human Research, Publication, and Ethics at the Kwame Nkrumah University of Science and Technology before commencing data collection. The Ethical Reference number is CHRPE/AP/292/20. The study also ensured issues of confidentiality, the anonymity of participants, and data are protected. Informed consent was obtained from all the participants before they were included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.