
Abstract
Abstract
Purpose
To investigate the success rate of the Tübingen hip flexion splint (THFS) for the treatment of developmental dysplasia of the hip (DDH), of different severity as per the Graf classification, among infants younger than six months of age. The type and incidence rate of complications associated with THFS treatment were also evaluated.
Methods
The following databases were searched using keywords and limited for age less than six months: PubMed, Embase, Web of Science, Cochrane Library, and SinoMed, between inception and July 2020. Articles were screened and extracted by two researchers, and the quality of the included literature was evaluated (methodological index for non-randomized studies criteria). R studio 1.3 was used for statistical analysis. The review process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results
After screening, eight articles were included in the analysis, contributing 1211 hips (875 patients). The overall success rate of THFS treatment is 91% (95% confidence interval (CI) 0.82 to 0.95). The success rate by Graf type is as follows: type-II, 98% (95% CI 0.94 to 1.00); type-III, 96% (95% CI 0.88 to 1.00); and type-IV, 32% (95% CI 0.18 to 0.47). Complications (24/1211, 2%) included transient femoral nerve palsy (n = 1); avascular necrosis of the femoral head (n = 9) and residual acetabular dysplasia (n = 14).
Conclusion
THFS treatment is successful for Graf type-II and –III, but low for type-IV, with a low rate of complication. THFS may be an effective treatment option for DDH among infants less than six months of age. However, those with Graf type-IV require close monitoring.
Level of Evidence
III
Introduction
Developmental dysplasia of the hip (DDH) is one of the most common hip disorders in children, with an incidence rate ranging between 0.06% and 76.1%. 1 Hip abduction braces, such as the Pavlik harness (PH), 2 Tübingen hip flexion splint (THFS), 3 von Rosen splint, Craig splint and Frejka pillow, are commonly used to manage DDH among infants less than six months of age. The common goal of these devices is to maintain a normal alignment of the hip to stimulate the development of the acetabulum. 4 The PH is the most widely used device in the early management of DDH, maintaining the hip in a position of 90° to 10° of flexion and 40° to 50° of abduction to achieve a normal coverage of the femoral head. Although the rate of successful reduction of the hip using a PH is high at 84% to 99%,2,5 treatment-associated complications have been reported, including hip joint reduction failure, femoral nerve palsy6–8 and avascular necrosis of the femoral head (AVN), which has been reported in up to 30% of cases.9–12 In 1990, Bernau 3 introduced the THFS, which maintains the hip joint in a position over 90° of flexion and 40° of abduction. 13 The THFS has been shown to have a similar reported treatment success rate to the PH but a lower incidence rate of AVN. 14 As such, the use of the THFS has gained popularity among paediatric orthopaedic surgeons, and it is increasingly being recognized as a useful treatment option for infants with DDH.
Our aim was to conduct a systematic review and meta-analysis: 1) to evaluate the success rate for the THFS used for the treatment of DDH of different severity, as defined by the Graf classification, 15 among infants less than six months of age; 2) to determine the associated rate of complications; and 3) to guide decisions regarding the selection of hip orthosis to use for the management of DDH among infants less than six months of age.
Materials and methods
Search strategy
We conducted a structured search of the following databases, from their inception to 31st July 2020: PubMed, Embase, MEDLINE (OVID), Web of Science, Cochrane Library and Sinomed. We combined subject words and keywords using Boolean operators to search with no limitations on the year of publication and language. We also searched relevant reference lists and relevant journals and translated non-English articles. Our search adhered to the Preferred Reporting Items for Systematic Review and Meta-analysis guidelines for a systematic review of success rates. 16
Inclusion criteria and exclusion criteria
The inclusion criteria were as follows: age less than six months at the beginning of treatment; DDH confirmed by ultrasound (US) diagnosis, including the Graf classification type (II, IIC, IID, III or IV); 15 treatment using the THFS as an abduction splint; and inclusion of treatment outcome and complication data. The exclusion criteria included: age more than six months at the beginning of treatment; pathological dislocation of the hip; studies from which statistical data could not be extracted; and studies with a methodological index for non-randomized studies (MINORS) quality evaluation score lower than eight points. 17
Quality evaluation using the MINORS checklist
The quality of included studies was assessed using the MINORS item quality evaluation checklist, 17 based on the following 12 indicators: a clearly stated aim; inclusion of consecutive patients; prospective data collection; endpoints appropriate to the aim of the study; unbiased assessment of the study endpoint; follow-up period appropriate to the aim of the study; loss to follow-up < 5%; prospective calculation of the study size; adequate control group; temporary groups; baseline equivalence of groups; and adequate statistical analysis. The first eight items apply to both comparative and non-comparative studies, while the last four apply only to comparative studies. The items are scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and adequate). The global ideal score was 16 for non-comparative studies and 24 for comparative studies. 17 Two researchers (FC and HWX) scored the literature independently according to the MINORS criteria checklist. In the event of a conflicting evaluation of an article, after discussion, the two evaluators proposed a common score.
Screening and data extraction
According to the predetermined inclusion and exclusion criteria, two researchers independently screened and extracted the data. Disagreements were resolved by consensus between the authors. The following data were extracted for analysis: the characteristics of the study, including the first author, year of publication, country of origin, number of patients, type of study and timing of measured outcomes; and the clinical characteristics of patients, including age at the time of diagnosis, sex, Graf classification of the DDH, treatment duration, treatment success rate and incidence of complications.
Outcome measures
The criteria for successful treatment were as follows: stable and concentric reduction achieved; Graf type-I on US examination; no signs of acetabular dysplasia on anteroposterior pelvis; no sign of hip instability or dislocation on clinical examination; and no subsequent treatment was needed during the follow-up period. Treatment was considered to have failed if: subsequent closed reduction and hip spica cast immobilization were required; presence of residual acetabular dysplasia; and re-dislocation or subluxation over the follow-up period. The type and incidence rate of treatment-related complications were recorded, including AVN, femoral nerve palsy and skin lesions.
Statistical analysis
R studio 1.3 (RStudio Inc., Boston, MA, USA) was used for statistical analyses. Heterogeneity was assessed using the chi-squared statistic, with thresholds of ≥ 25%, ≥ 50% and ≥ 75% indicating low, moderate and high heterogeneity, respectively. A random-effects model was used to evaluate treatment outcomes when heterogeneity between studies was moderate or high (chi-squared > 50%), with a fixed-effect model used when heterogeneity was low. 18 The 95% confidence interval (CI) was used to measure the effect size. Outcomes were compared between Graf types (II, III and IV). The treatment success rates between the groups were compared using the Mann-Whitney U test (SPSS 21.0, IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered significant for all analyses. Publication bias was evaluated using Egger's test, with no publication bias considered for an Egger's test > 0.05.
Results
Search results
Our search strategy identified 5692 articles. Of these, 121 were duplicates. Following screening on the pre-specified criteria, including full text review of retained abstracts, eight articles in English and one in German were included in our analysis.13,14,19–25 Two of these articles, by Kubo et al13,20 used the same study group with outcomes measured at the mid-term and end-point of the period of follow-up. The flow diagram of study selection is shown in Fig. 1.
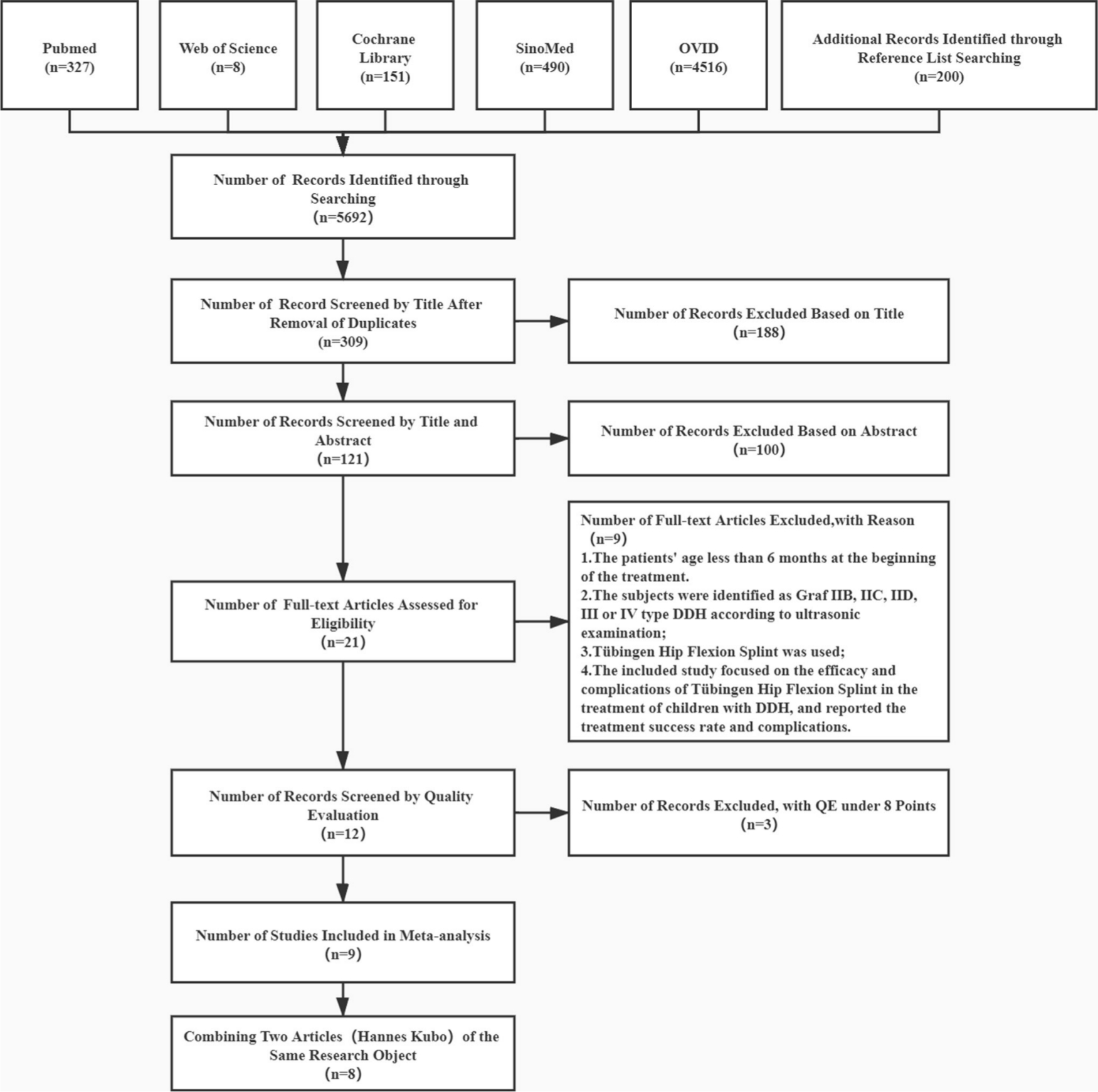
Study screening and selection process.
Basic characteristics of included studies
The characteristics of the studies included in the analysis are presented in Table 1, including the quality of the study and the incidence of complications reported. Overall, the eight articles reported on 875 patients contributing 1211 hips with a confirmed diagnosis of DDH. The male-to-female ratio was 1:41.
Basic characteristics of included literature
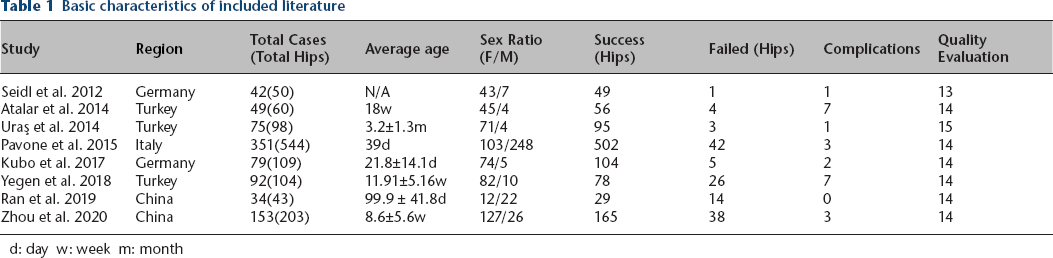
d: day w: week m: month
Outcomes of the meta-analysis
Overall, the rate of success rate of THFS treatment among infants younger than six months of age was 91% (95% CI 0.82 to 0.95; p < 0.01; 1078/1211 hips), with high heterogeneity between studies (chi-squared = 92%) (Fig. 2a and Table 2). Of the eight articles included, six reported outcomes for the different Graf DDH types. For type-II DDH, the success rate was 98% (95% CI 0.94 to 1.00; p < 0.01), with high heterogeneity between studies (chi-squared = 78%). A successful outcome was obtained for 368/380 type-II DDH hips, with a failed treatment in 12/380 hips (Fig. 2b and Table 2). For type-III hips, the success rate remained high at 96% (95% CI 0.88 to 1.00; p < 0.01), with moderate heterogeneity (chi-squared = 55%). Treatment was successful in 106/114 type-III hips, with failure in 8/114 (Fig. 2c and Table 2). The success rate for type-IV hips was lower at 32% (95% CI 0.18 to 0.47; p = 0.14), with low heterogeneity (chi-squared = 40%). Treatment was successful in 25/70 type-IV hips and failed in 45/70 (Fig. 2d and Table 2). The treatment success rate for type-IV hips was significantly lower than for type-II and type-III hips (p < 0.01).
Summary of meta-analysis results

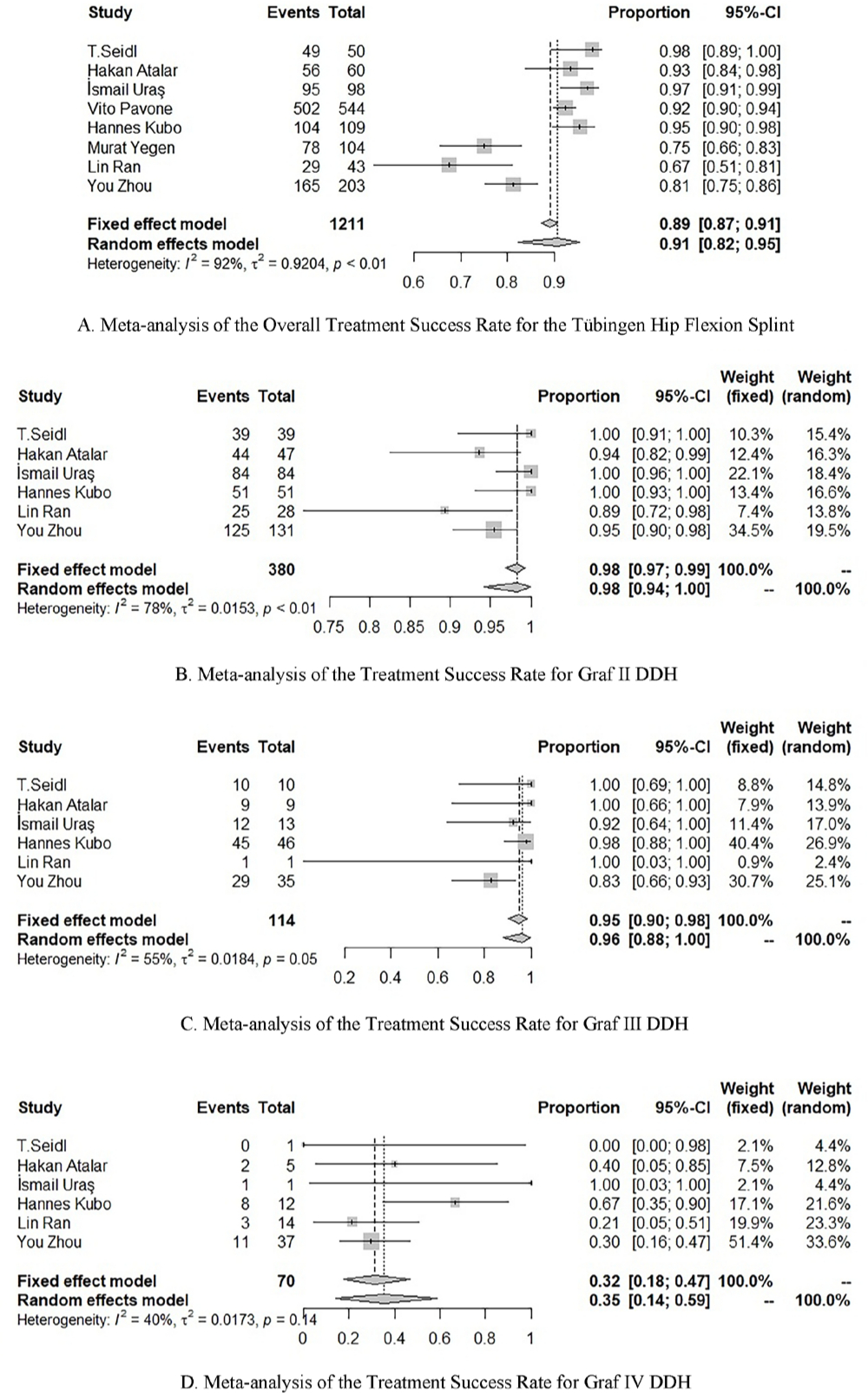
Meta-analysis of the treatment success rate for the Tübingen hip flexion splint.
Complications of THFS treatment
The overall complication rate of THFS treatment was 2% (95% CI 0.01 to 0.05; p < 0.01), with high heterogeneity (chi-squared = 76%). The distribution of complications was as follows (Fig. 3): transient femoral nerve palsy (n = 1; 4.2%); AVN (n = 9; 37.5%); and residual acetabular dysplasia (n = 14; 58.3%).
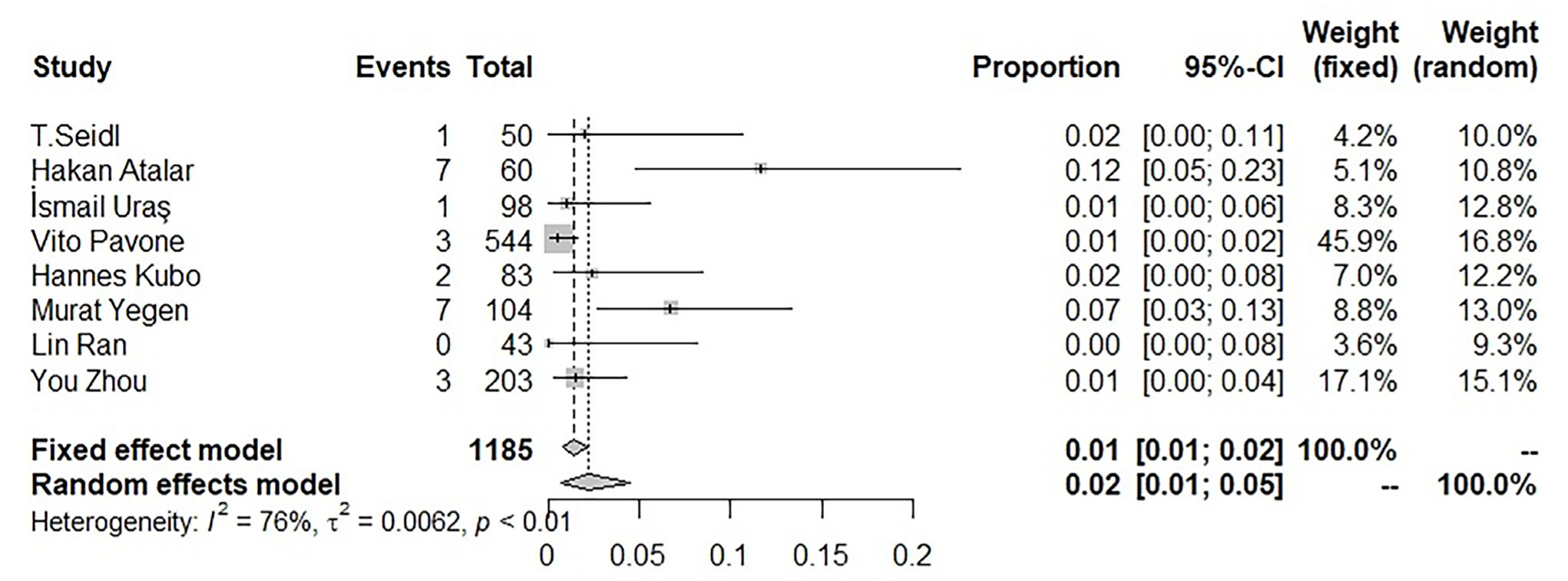
Meta-analysis of the incidence of treatment-associated complications.
Publication bias
According to Egger's regression (intercept 1.46; standard error 2.27; t = 0.77, df = 6; p = 0.47), there was no evidence of publication bias on the measured success rate of THFS treatment (p = 0.47 > 0.05).
Heterogeneity test
Review Manager (version 5.4; Cochrane, London, UK) was used to analyze the date of publication, country of origin, average age of the study group and other factors. Results indicated that the difference in the country of origin was an important factor affecting heterogeneity (p < 0.01).
Discussion
The present study indicates that the overall success rate of THFS treatment for DDH among infants younger than six months of age was 91%. This high rate of treatment success reflects the good tolerance of the splint and its ease of application, and good compliance on the part of parents.
The THFS maintains the hip joint at 90° of flexion and 40° of abduction, which is sufficient to achieve a concentric reduction of the hip.3,13 A previous study reported that insufficient hip abduction and flexion can lead to an unstable reduction, preventing the hip from developing normally. 26 The THFS has a similar success rate than the PH (84% to 99%)27,28 but with a lower incidence of AVN.5,14 Treatment failure with the PH may be due to the fact that it can only maintain the hip in 80° to 90° of abduction by gravity. 8 Moreover, clinical outcomes will be influenced by the use of the PH, namely if it is worn appropriately and sufficiently. 28 However, the PH is relatively complex to use and the reduced compliance of families with the use of the PH increases the rate of treatment failure.24,29 Compared with the PH, the THFS is easier to use and families are more compliant with its use, which helps to explain the high rate of good clinical outcomes. 3 This is why the THFS has gained popularity among paediatric orthopaedic surgeons. However, the success rate of THFS treatment was significantly lower for type-IV (32%) than either type-II (96%) or type-III (98%) DDH. This difference may be due to the severity of the dysplasia in type-IV hip, compared with type-II and –III hips, with the normal anatomy of the hip being difficult to restore regardless of the type of hip abduction orthosis used.26,30,31 Nevertheless, the success rate of THFS for the treatment of Graf type-IV hips appears to be higher than the rate for PH treatment, as previously reported, although we did not compare the THFS with the PH specifically in our study. By comparison, not all type-IV hips treated using the THFS have poor outcomes. According to Uraş et al 24 and Ardila et al, 32 patients with a reducible hip, as demonstrated by a positive Ortolani sign, can benefit from treatment using a THFS. Ömeroglu 33 showed the Ortolani manoeuvre to be a useful clinical diagnostic tool to assess the reducibility of hip dislocation and, thus, can be used in treatment decision algorithms.
The overall complication rate of THFS treatment was 2%. This low rate of complications may be related to the relatively stable structure of the splint. The THFS is a rigid splint that can maintain the hip in flexion, while limiting excessive hip abduction, through adjustment of the rigid bar between the hips. In this position, the hip joint can be flexed and extended through part of the range of movement, with the pressure distributed more evenly with less tension on the vessels, which can potentially reduce the risk of AVN associated with the treatment of DDH.3,14 Besides, a combination of tight adductors and rigid immobilization in extreme abduction can lead to compression of retinacular vessels leading to AVN. 34 AVN of the femoral head is the most serious complication of DDH treatment, with an average incidence rate around 8% (0% to 22%) for the PH.1,9,10,34 The incidence of femoral nerve palsy with PH treatment is 2.5%. 35 As with the THFS, the PH keeps the hips in flexion and abduction, while allowing some movement of the hip. 36 However, Zhou et al 14 indicated that the relatively high incidence of AVN with PH treatment could be attributed to an over-abduction of the hip due to the non-rigid design of the splint. Moreover, Novais et al 30 reported a non-negligible rate of acetabular dysplasia over a one-year period of follow-up in infants with type-IV DDH who had achieved a successful treatment using the PH. In particular, the incidence of residual dysplasia at the six- and 12-month follow-up was 11.7% and 11.8%, respectively. To reduce the incidence of complications, Pavone et al 21 suggested a close follow-up by US, while Kubo et al 20 suggested regular radiographic assessment of acetabular development, as per the Tönnis classification, until skeletal maturity. Ashoor et al 37 evaluated the outcomes across six studies using the THFS (713 children; 1001 hips), reporting a pooled failure rate of 7.79% (0% to 25%), AVN rate of 0.5% (0% to 2.4%) and residual dysplasia rate of 6.7%.13,19–21,23,25,38 However, they did not stratify the results according to the Graf subtype. 37 Failure of the PH is commonly reported in patients with high or fixed dislocation and subsequent AVN. According to Tiruveedhula et al, 34 if the hip reduction is not achieved within six weeks, PH treatment should be abandoned and surgical options such as open/closed reduction should be considered. However, if treatment is completed when achieving a Graf type-I hip, the presence of residual acetabular dysplasia within the following months/years may more be related to natural history of the disease than to the treatment device or to a treatment device which is wrongly used with a forced abduction thus potentially altering the cartilaginous growth plate of the acetabulum.
We encountered some limitations in the analysis of our results. Since the use of THFS has not yet been generalized, the clinical findings are relatively limited and it is possible that genetic susceptibility within different ethnic groups may have an impact on the success rate of using the THFS for the treatment of DDH. 28 Further research, such as large-scale multi-regional clinical trials, is needed to collect more clinical data to support our findings.
In conclusion, the success rate of THFS in the treatment of Graf type-II and type-III hips is high at 98% and 96%, respectively, but is significantly lower for of type-IV hips (32%; p < 0.01). In addition, the rate of complication was low (2%). Therefore, the use of a THFS appears to be an effective treatment option for DDH among infants, requiring careful monitoring for those with type-IV DDH.
Footnotes
XTX: Study design, Read and approved final manuscript.
YWW: Study design, Read and approved final manuscript.
PW: Study design, Read and approved final manuscript.
FC: Study design, Manuscript preparation, Data analysis, Manuscript revision, Read and approved final manuscript.
HWX: Study design, Surgical operation, Supervision of the research group, Read and approved final manuscript.