
Abstract
Abstract
Purpose
Developmental dysplasia of the hip (DDH) encompasses a wide pathological spectrum, from mild acetabular dysplasia to complete congenital hip dislocation at birth. Screening policies have been implemented in an effort to effectively identify and treat patients with DDH. Since 2009 there has been a national DDH programme in Chile. The current study evaluates the results of the programme in patients born between 2010 and 2015.
Methods
Records of patients hospitalized from 1st January 2010 to 31st December 2019 were retrieved from national databases. Those born from 1st January 2010 to 31st December 2015 who underwent a procedure for DDH under general anaesthesia during their first five years of life were selected. Sex, first surgical procedure and age at first surgical procedure were analyzed. The incidence of DDH that required major surgical treatment was calculated.
Results
A total of 961 children born from 1st January 2010 to 31st December 2015 underwent a procedure for DDH during their first five years of life. The number of major procedures was significantly lower than the number of minor procedures (269 vs 692). The incidence of major procedures was 0.18 per 1000 live births. Girls underwent a higher number of procedures than boys (831 vs 130), whereas 39.2% of the boys and 26.2% of the girls had major procedures. The mean age at the time of the first procedure was 15.35 months (sd 10.09; range 0.03 to 55.92 months).
Conclusion
The present study suggests that the Chilean National DDH Screening Program is an appropriate programme with substantial benefits with respect to public health.
Level of evidence
II
Introduction
Developmental dysplasia of the hip (DDH) encompasses a wide pathological spectrum, from mild acetabular dysplasia to complete congenital hip dislocation at birth. 1 It can affect all components of the hip of mesodermal origin (muscle, bone and blood vessels), with ossification delay of the femur and iliac, cartilage alteration and soft-tissue secondary contracture. 2 Reports indicate a global DDH rate of up to 4% of the population, rendering it one of the most common orthopaedic diseases. 3 The incidence of DDH in newborns in the Chilean population is approximately 3.9%. 4 The most severe form of DDH is congenital hip dislocation, which has an incidence ranging between 0.1% and 0.2% of the population. 1 If a child with congenital hip dislocation is not properly treated, substantial physical impairment during adulthood can be expected. DDH is evidently the most common cause of total hip arthroplasty in young adults (approximately 21% to 29% of cases). 5 Acetabular dysplasia is the most common cause of hip arthroplasty in women aged < 50 years6,7 and it may be associated with infantile DDH.
The maturation curve of the newborn hip peaks during the first four months of life. 8 For this reason, early conservative treatments such as reduction of a dislocated hip or the maintenance of a reduced but dysplastic hip have the highest success rate with respect to restoring normal anatomy in over 90% of cases, with the best results ensuing when treatments are initiated before the age of six weeks. 9 Treatments incorporating a Pavlik harness for stable dysplastic hip and reduced but dislocatable hips result in satisfactory clinical and radiological outcomes in such infants. 10 The success rate of conservative early Pavlik harness treatment for dislocated but reducible hips is approximately 70% to 80%.11,12 Conversely, late conservative treatments performed after the age of six months tend to be unsuccessful and result in anatomical alterations associated with early degenerative changes of the hip. Thus, current evidence suggests that DDH must be treated before the age of six months. 13
Numerous screening policies have been implemented and evaluated around the world in efforts to ensure that children are identified and treated for DDH in a timely manner, including clinical instability detection in newborns, ultrasound screening at four to six weeks of age, and radiographic evaluation of the pelvis at three to four months of age. Policy to implement screening programmes depends on the outcomes expected and the resources and budget available, 14 and it is broadly acknowledged that late detection increases treatment complexity and costs.15,16 Because of the high incidence of DDH in the Chilean population, radiographic evaluation at three months of age has been common practice since the late 1970s. The age of three months was chosen to obtain the screening radiograph for hip dysplasia as it is the earliest moment that allows for assessment of mild dysplasia or unstable hips with this method, given the acetabular ossification process.17–19 A national DDH programme that includes diagnosis and access to treatment for every child was developed and instituted by the National Health Ministry, 20 and it has been in operation since 2009. The programme's protocol promotes early diagnosis via ultrasound when accessible, mandatory specialist evaluation in the presence of high-risk factors and standardized radiographic imaging at the age of three months. The mandatory screening programme requires that every child born in Chile undergo an anteroposterior pelvic radiograph projection at three months of age or a Graf technique ultrasound at six weeks of age, in medical centres where appropriate facilities are available. According to the national programme registry, 7968 newborns were treated with a Pavlik harness during 2019, which is consistent with the previously described incidence of DDH in Chile.
In the current study the results of the DDH screening programme in Chile were evaluated in patients born between 2010 and 2015, during their first five years of life. The numbers of major procedures (open reduction, pelvic osteotomy, femoral osteotomy) and the numbers of minor procedures (closed reduction, hip spica casting, adductor tenotomy) during the study period were compared, and ages at the first procedure and patient sex distributions were analyzed.
Materials and methods
The medical records of patients hospitalized from 1st January 2010 to 31st December 2019 were retrieved from the Chilean Department of Statistics and Health Information database, 21 which is a freely accessible data repository maintained by the Chilean Health Ministry that includes all patients discharged from all public and private hospitals in the country. Among other data, the registry includes patient demographics, diagnoses codified in accordance with the International Classification of Diseases (ICD) 10th revision 22 (obligatory in the registry since 2008) and all procedures performed during hospitalization.
Patients born between 1st January 2010 and 31st December 2015 diagnosed with the code ICD-10 Q65 (Congenital Deformities of the Hip) from 1st January 2010 to 31st December 2019 on their record were identified. From these, those who underwent a procedure for DDH under general anaesthesia were selected. Patients who underwent more than one surgery were logged by the first procedure performed. Sex, first surgical procedure and age at first surgical procedure were recorded and analyzed. Surgical procedures were categorized as major (open reduction, pelvic osteotomy, femoral osteotomy) or minor (closed reduction, hip spica casting, adductor tenotomy).
The incidence of DDH requiring major surgical treatment was calculated using the accumulated numbers of major procedures during the first five years of life in those children who were born in one birth cohort year, divided by the number of total live births in that birth cohort year according to the Statistics National Institute, 23 an autonomous administrative agency that compiles official statistics data in Chile. Incidence of DDH requiring major surgical treatment was then divided in ‘open reduction without osteotomy’ procedure and ‘open reduction associated with osteotomy (acetabular and/or femoral)’ procedure.
Statistical analysis
A generalized linear model was used to compare the numbers of major and minor procedures over the years, between sexes and between age groups. All analyses were performed in R (R Core Team 2020, R Foundation for Statistical Computing, Vienna, Austria).
Results
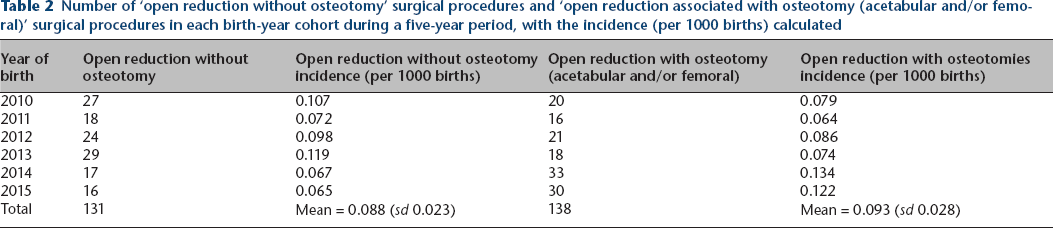
From 1st January 2010 to 31st December 2019, a total of 961 children born between 1st January 2010 and 31st December 2015 underwent a procedure for DDH under general anaesthesia during the first five years of life. The total number of procedures changed significantly over the years (chi square = 11.22; p = 0.047), likely due to a high number of procedures performed in 2010 (Fig. 1). The number of major procedures was significantly lower than the number of minor procedures (269 vs 692; chi square = 192.7; p < 0.0001; Fig. 1) but the difference between procedures did not change from 2010 to 2015 (chi square = 7.03; p = 0.22; Fig. 1). The mean incidence of major procedures in all patients was 0.18 per 1000 live births (sd 0.021; range 0.14 to to 0.20), and that incidence was stable over the years (Table 1). Incidence for ‘open reduction without osteotomy’ procedures was 0.088 per 1000 live birth (sd 0.023; range 0.065 to 0.119), 131 cases in total from 1st January 2010 to 31st December 2019; and incidence for ‘open reduction associated with osteotomy (acetabular and/or femoral)’ procedures was 0.093 per 1000 live birth (sd 0.028; range 0.064 to 0.134), 138 cases in total from 1st January 2010 to 31st December 2019 (Table 2).
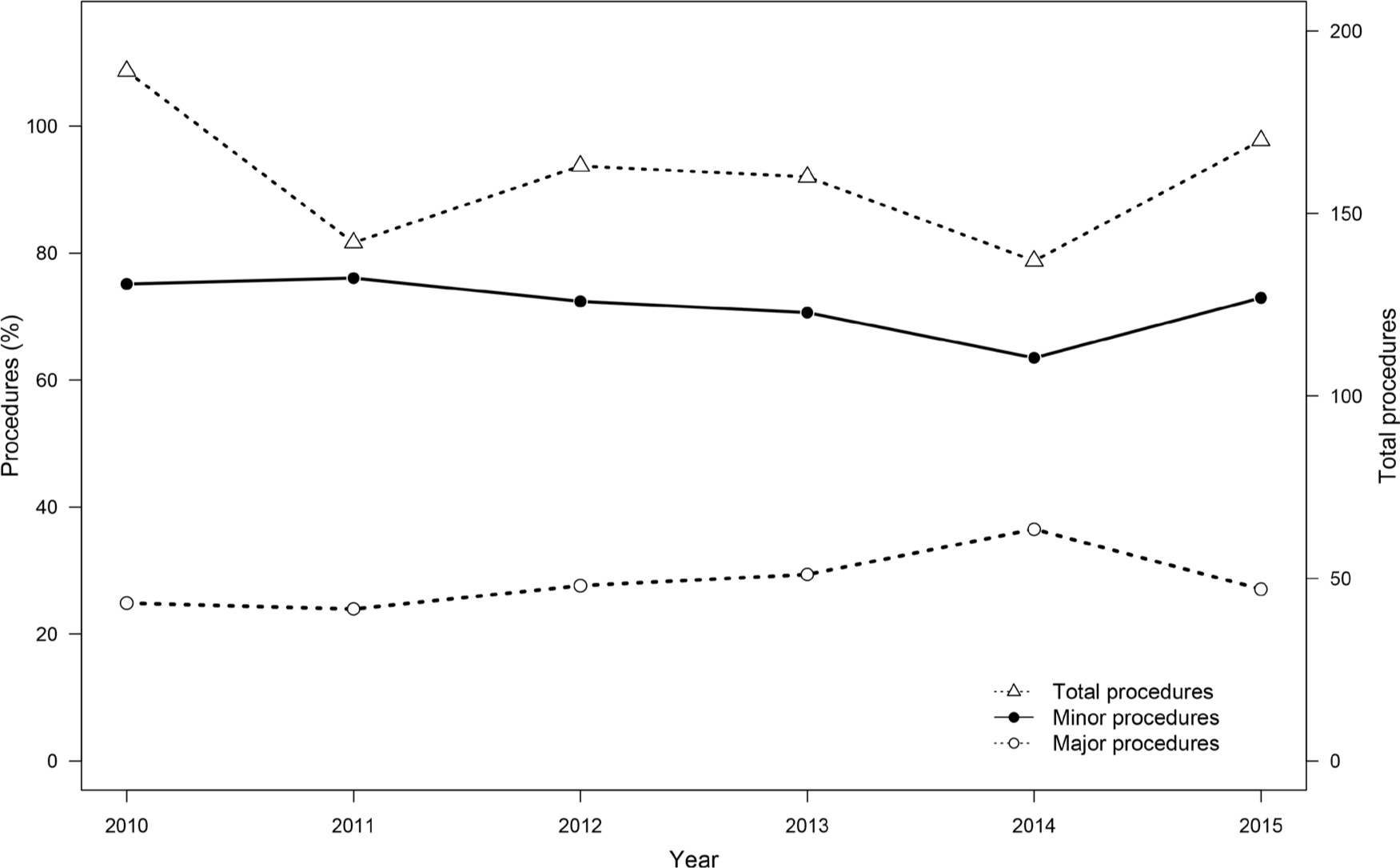
Percentages of minor and major procedures during the first five years of life in each birth-year cohort.
Number of minor and major procedures in each birth-year cohort during a five-year period, with the incidence of major procedures calculated

Number of ‘open reduction without osteotomy’ surgical procedures and ‘open reduction associated with osteotomy (acetabular and/or femoral)’ surgical procedures in each birth-year cohort during a five-year period, with the incidence (per 1000 births) calculated
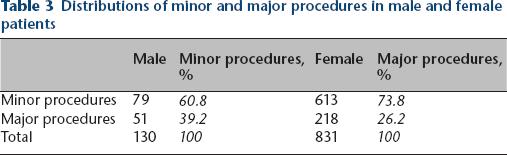
In analyses of relationships between procedure type and patient sex, girls underwent a higher number of procedures than boys (831 vs 130; chi square = 570.6; p < 0.0001; Table 3). There was also a significant interaction between sex and procedure type, with 51/130 (39.2%) of the boys having a major procedure compared with 218/831 (26.2%) of the girls (chi square = 8.91; p = 0.003). The mean age at the time of the first procedure was 15.35 months (sd 10.09; range 0.03 to 55.92 months), the mean age for major procedures was 20.46 months (sd 12.51; range 5.30 to 55.92 months), and the mean age for minor procedures was 13.37 months (sd 8.17; 0.03 to 55.49 months). There was a significant interaction between age group and procedure type (chi square = 97.82; p < 0.0001), with the number of minor procedures decreasing with age (Fig. 2). Between 0 and 5.9 months 97.1% of the procedures were classified as minor, whereas only 36.7% of the procedures performed between 36 and 60 months were minor (Fig. 2).
Distributions of minor and major procedures in male and female patients
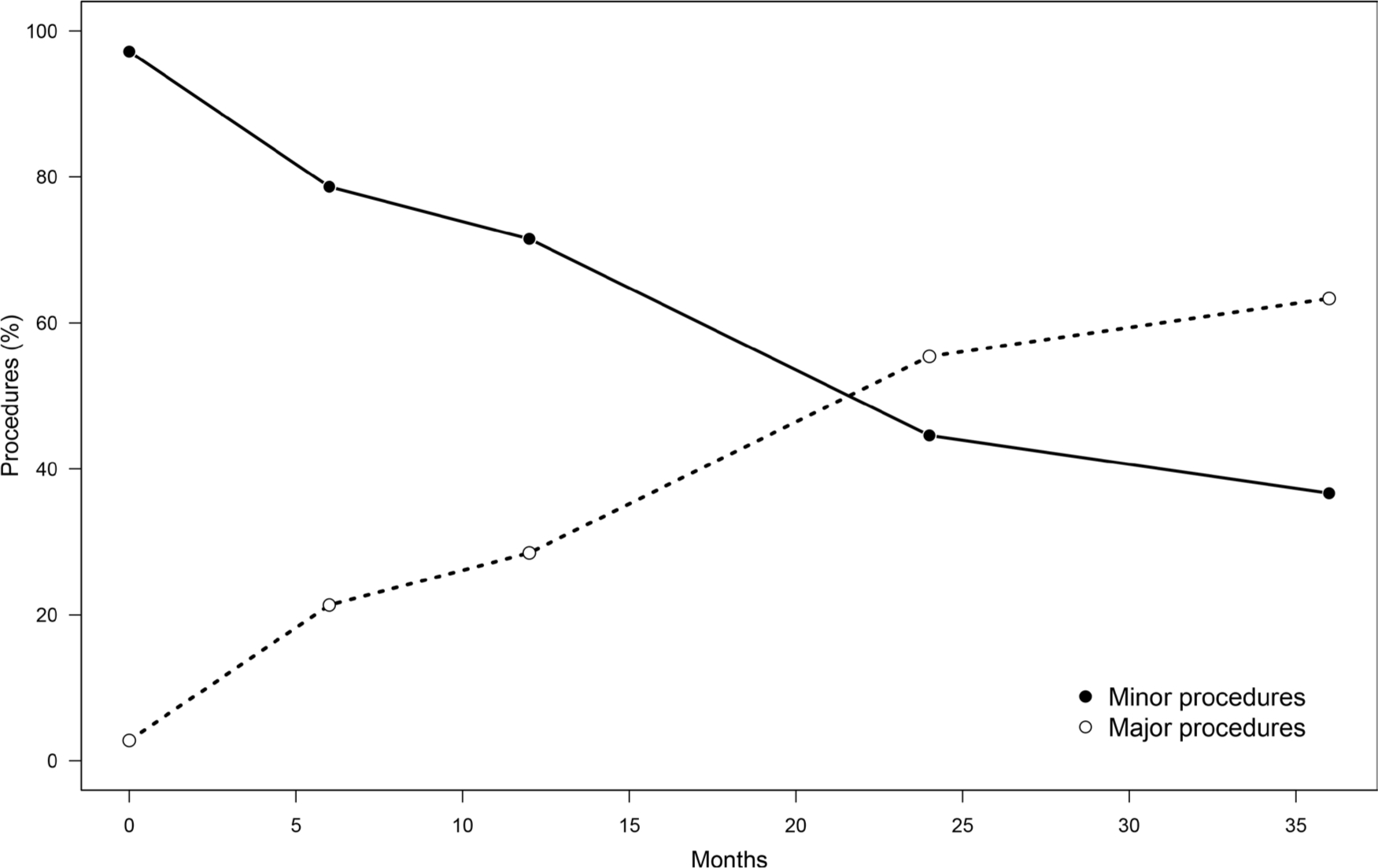
Associations between age at first procedure and type of procedure performed.
Discussion
Given the good results observed in our clinical practice, with the reduced number of major surgeries performed, it is important to acknowledge the apparent success of the Chilean National DDH Screening Program which includes access to diagnosis – usually via anteroposterior pelvic radiograph at three months of age – and treatment of the entire population. As indicated by the present study, the Chilean National DDH Screening Program has resulted in a low number of major surgeries compared with countries that do not screen for DDH or that perform clinical surveillance, and adequate access to timely treatment. We found a low number of ‘open reduction without osteotomy’ procedures (131 cases) and ‘open reduction associated with osteotomy’ procedures (138 cases) during this ten-year period. These results can promote the use of a similar screening programme in countries with limited resources or medical access to specialists. The results also demonstrate an increase in major procedures after walking age, and a higher percentage of major procedures in boys compared with girls, which is concordant with our clinical experience.
Neonatal and early childhood screening protocols have been implemented in many countries to achieve early diagnosis of DDH and congenital hip dislocation. It is difficult to compare these different screening programmes directly because they have utilized different screening methods; the wide spectrum of the condition is difficult to standardize with regard to results and the incidence of DDH also differs from region to region. The relative costs of programme implementation and the actual budgets assigned to different programmes also differ between countries. As well as these variables increasing the difficulties associated with comparing DDH and hip dislocation screening programmes, the effectiveness of intervention is not clearly quantifiable. 24 Thus, the evidence available upon which to base recommendations is insufficient. 25
Godward and Dezateux 26 evaluated a surveillance scheme in the United Kingdom and reported an incidence of surgery of 0.78 per 1000 newborns, with a failure to detect 70% of cases. A clinical hip screening programme in Sweden reduced the incidence of late diagnosis of congenital hip dislocation from 0.91 per 1000 to 0.25 per 1000. 27 Chan et al 28 reported an incidence of surgery of 0.46 per 1000 newborn in South Australia after auditing their clinical screening programme. Similarly, in a study investigating clinical screening in Taiwan the incidence reported was 0.48 per 1000 newborns, with 40% of the diagnosed cases requiring surgery, 87% after walking age. 29
Selective ultrasound screening programmes fail to detect more than 88% of cases, because of an absence of risk factors (family history of DDH, born in breech position). It is dependent on neonatal hip examination, which has low successful detection rates and is strongly influenced by the experience of the examiner. It also fails to significantly reduce the need for open surgery. 30 Sink et al 31 reported that 85.3% of patients with symptomatic acetabular dysplasia at skeletal maturity did not meet recommendations for selective ultrasound screening. Despite these reports moderate evidence supports its use, 32 and patients who are presented after an age of three months have fewer traditional risk factors, so a high degree of suspicion should be applied to all children. 33
Universal ultrasound-based screening programmes evidently yield the best results and significantly reduce the need for open reduction and late secondary-related procedures. 34 The incidence of surgery in countries with universal ultrasound screening programmes is reportedly approximately 0.26 per 1000 newborns, 35 with an incidence of open surgery of 0.07 per 1000 36 . One limitation of ultrasound DDH screening programmes is the restricted access to standardized ultrasound in most countries. There is also concern about overtreatment being associated with early ultrasound screening, but classification systems have been devised to differentiate clinically relevant DDH, 37 and there is a preference for standardized ultrasound analysis. 38 With such methods, overtreatment can be avoided.
Varied information has been reported with respect to cost analyses of DDH screening programmes. Economic costs are difficult to assess because they are strongly influenced by local variations in incidence and health access. 39 The costs of treatment also differ between countries. Lastly, quality of life should be included in analyses of DDH screening programmes. 40 For the above-described reasons, recommendations for screening vary from region to region, 24 with some consensus that clinical benefit can overcome the associated costs, 16 but with lack of agreement between orthopaedic surgeons on the best approach for DDH screening. 41
In Chile, with a high incidence of DDH, radiograph evaluation has been routinely performed in all children at three months of age since the late 1970s. This has significatively reduced the number of open surgeries that were performed prior to then. The main advantage of radiograph evaluation is its low cost, high accessibility and standardized reproducible results. The main problem associated with its use is the lack of consensus with regard to the appropriate age at which to perform it, as it has been suggested that three months is not early enough. The degree of patient radiation exposure it entails is not thought to be clinically important 42 because the dose is very low.
The current study had some limitations. There are only a small number of relevant studies available to compare it with, and there is an absence of completely reliable previously recorded national data derived from the time before the national screening plan was implemented in Chile in 2009. The registry also does not specify any underlying conditions, so the numbers presented in the current analysis include patients with concurrent neurological pathology.
The results obtained in the present study indicate that the incidence of major procedures conducted while the Chilean National DDH Screening Program has been operating is 0.18 per 1000 newborns. There were no statistically significant differences between the six cohorts analyzed. This can be considered a low incidence of major procedures for DDH during the first five years of life. Compared with other relatively recent reports, it is almost four-times lower than the incidence associated with clinical surveillance screening programmes but twice as high as the incidence associated with universal ultrasound screening programmes, which is statistically significant. The majority of the procedures performed in the six cohorts in the present study were minor. We consider that the Chilean National DDH Screening Program is appropriate for use in regions with healthcare systems with limited resources, that the screening procedure is reproducible and that it yields substantial public health benefits.
Footnotes
JAP: Acquisition of data, Critical review of manuscript, Approval for publishing, Accountability for the work.
EAS: Acquisition of data, Critical review of manuscript, Approval for publishing, Accountability for the work.
LEC: Analysis and interpretation of data, Drafting and critical review of manuscript, Approval for publishing, Accountability for the work.
DFS: Conception of the study, Drafting and critical review of manuscript, Approval for publishing, Accountability for the work.
EAMB: Conception of the study, Drafting and critical review of manuscript, Approval for publishing, Accountability for the work.