
Abstract
Abstract
Purpose
The goal of this retrospective study was to compare the gradual lengthening of the ulna in children with multiple hereditary exostoses with and without an elastic intramedullary nail.
Methods
Between 1998 to 2018, the ulna was lengthened in 28 forearms in 21 patients (aged 7.1 to 16.6 years) using a monolateral external fixator when relative ulnar shortening exceeded 15 mm. In total, 16 forearms were lengthened with the external fixator (group I) and 12 forearms with the addition of an intramedullary elastic nail (group II). Subjective assessment of function, range of movement (ROM) of the wrist and elbow and complications were compared. Ulnar shortening, radial head dislocation, radial articular angle (RAA) and percentage of carpal slip and radial bowing were followed radiographically. The difference between the groups has been evaluated statistically.
Results
The function of the extremity improved partially in 81% of patients in group I and in 83% of patients in group II. ROM was not improved except for radial deviation. Radial head position did not change. The values in group II in comparison with group I are higher for gain of length and lower for bone lengthening index and for bone healing index. Carpal slip decreased insignificantly. The RAA and radial bowing decreased, the comparison of values between groups and age under and over ten years were not statistically significant. Complications were more common in group I. No permanent complications were noted.
Conclusion
The addition of an intramedullary nail during the gradual ulnar lengthening improves the gain, bone healing index and rate of complications.
Level of Evidence
III.
Introduction
The ulna and radius are involved in 30% to 60% of the patients with multiple hereditary exostoses (MHE) at pre-school age.1,2 Typical deformities include, relative shortening of the ulna; bowing of the radius and/or ulna; increased ulnar tilt of the distal radial epiphysis; ulnar deviation of the hand; ulnar-ward translation of the carpus; and a possible dislocation of the radial head. 1 In addition to the cosmetic deformity, these deformities produce limited forearm rotation and wrist movement, and pain and limited movement of the elbow by the radial head dislocation. Under normal conditions, 20% of the load of the forearm is transferred through the ulnar side of the wrist. 3 Relative shortening of the ulna contributes to overloading of the radiocarpal joint. The treatment strategy of forearm deformities remains controversial and varies from non-treatment to early radical complex treatment.1,4–6 In our department, the treatment strategy consists of early excision of exostoses of both bones as a first step followed by a gradual ulnar lengthening by callotasis as the second step, when relative shortening of the ulna exceeds 15 mm. In our experience, shortening of the ulna of < 1 cm does not require the correction; shortening between 1 cm to 1.5 cm could be treated with a single step lengthening with bone graft. Timing for gradual ulnar lengthening depends on cortical restitution after excision of the exostosis, in order to achieve adequate stability for the screws of the external fixator. Generally, the goals of ulnar lengthening are: 1) to improve the discrepancy in the length of the forearm bones reducing overload on the radiocarpal joint; 2) to avoid/improve radial head dislocation; 3) to improve function of the wrist and elbow joints4–7 and finally improve cosmesis. Ulnar lengthening using the callotasis technique is difficult and has a longer bone healing index due to the small diameter of the ulna in comparison with other bones.7,8 Literature reports have described significant improvement of forearm bone lengthening combined with intramedullary nailing,7,9 namely the shortening of the bone healing index. According to these reports and our own positive experiences in the lengthening of other long bones, we attempted to improve the results of gradual ulnar lengthening by the addition of an intramedullary nail to enhance the stability of bone ends to accelerate the ossification of regenerate bone and to shorten external fixation time. The final decision for lengthening with or without intramedullary nail, however, depended on the surgeon's preference.
The aim of this study was to compare ulnar lengthening by callotasis in MHE with and without an intramedullary nail. We hypothesized that lengthening of the ulna in combination with the nail would reduce: 1) bone lengthening index; 2) bone healing index (external fixation time); and 3) the complication rate.
Material and methods
This is a retrospective study of a cohort of 21 patients (28 forearms), where gradual ulnar lengthening was performed between 1998 and 2018. Inclusion criteria were: patients with MHE who were over six years of age with a relative ulnar shortening exceeding 15 mm (Fig 1a). The monolateral Orthofix LRS system for children (Orthofix S.r.I, Verona, Italy) was used in 24 forearms, while the Pediatric Wagner system (Mathys, Betlach, Switzerland) was used in four forearms. The surgery was carried out by four different surgeons (JC,MO,MF,PD). The patients were divided into two groups. Group I consisted of 16 ulnas (12 patients, Table 1) which were lengthened with only the external fixator (between 19th June 1998 and 7th January 2015) and in group II, 12 ulnas (nine patients, Table 2) were lengthened by combining the external fixator and a single elastic titanium nail (diameter 2 mm) (between 29th October 2009 and 25th April 2018). The nail was introduced into the ulna through the olecranon distal to the physis, prior to the application of the fixator and was buried below the skin. Two cortical screws (diameters 3.2 mm to 3.5 mm) were inserted into each fragment in both groups. The age of patients was similar in both groups: six to 17 years (mean 10.7 years) in group I and six to 15 years (mean 11.2 years) in group II (Table 1, 2). Corticotomy of the ulna was performed between its proximal and middle quarters by predrilling of the cortex, with subsequent completion of the fracture with an osteotome. Distraction started after seven days at the rate of 1 mm/day. This rate was reduced to 0.5 mm/day if there was attenuated regenerate formation or other complication, i.e. deviation of bone ends. The patients were followed up clinically and radiographically at two-week intervals during the lengthening (Fig. 1b), and thereafter regularly every four weeks until consolidation of the regenerate was achieved. The lengthening was discontinued when the distal physis of ulna reached the level of the ulnar margin of the radiocarpal surface but overlengthening of ulna was performed in the majority of patients (Table 1 and 2) in order to prevent the necessity of repeated lengthening due to the loss of the ulnar length during the growth. The amount of overlengthening depended on the subjective assessment of surgeon comfort/discomfort after achievement of above-mentioned length of the ulna. The external fixator was removed when consolidation was complete or corticalization of the regenerate was visible on radiographs (Fig. 1c). The intramedullary nail was removed after three to six months. The global follow-up ranged from two to 11 years (mean 4.5 years) in group I and from two to eight years (mean 4.7 years) in group II.

a) Radiograph of left forearm, boy #19, age ten years. Exostoses of the ulna and radius (arrows). Radiological parametres according Burges and Gates: linear axis of the forearm (a); radial articular angle (RAA); ulnar variance 17 mm – shortening of the ulna relative to the radius (b); double arrow – carpal slip (%); b) radiograph six months after exosostes removal. Ulnar lengthening of 24 mm using Orhofix exernal fixator and intramedular elastic nail, boy #19; c) consolidation of the bone regenerate after ulnar lengthening and external fixator removal. Healing index 45, 8, boy #19.
Patients treated for ulna shortening with external fixator (group I)
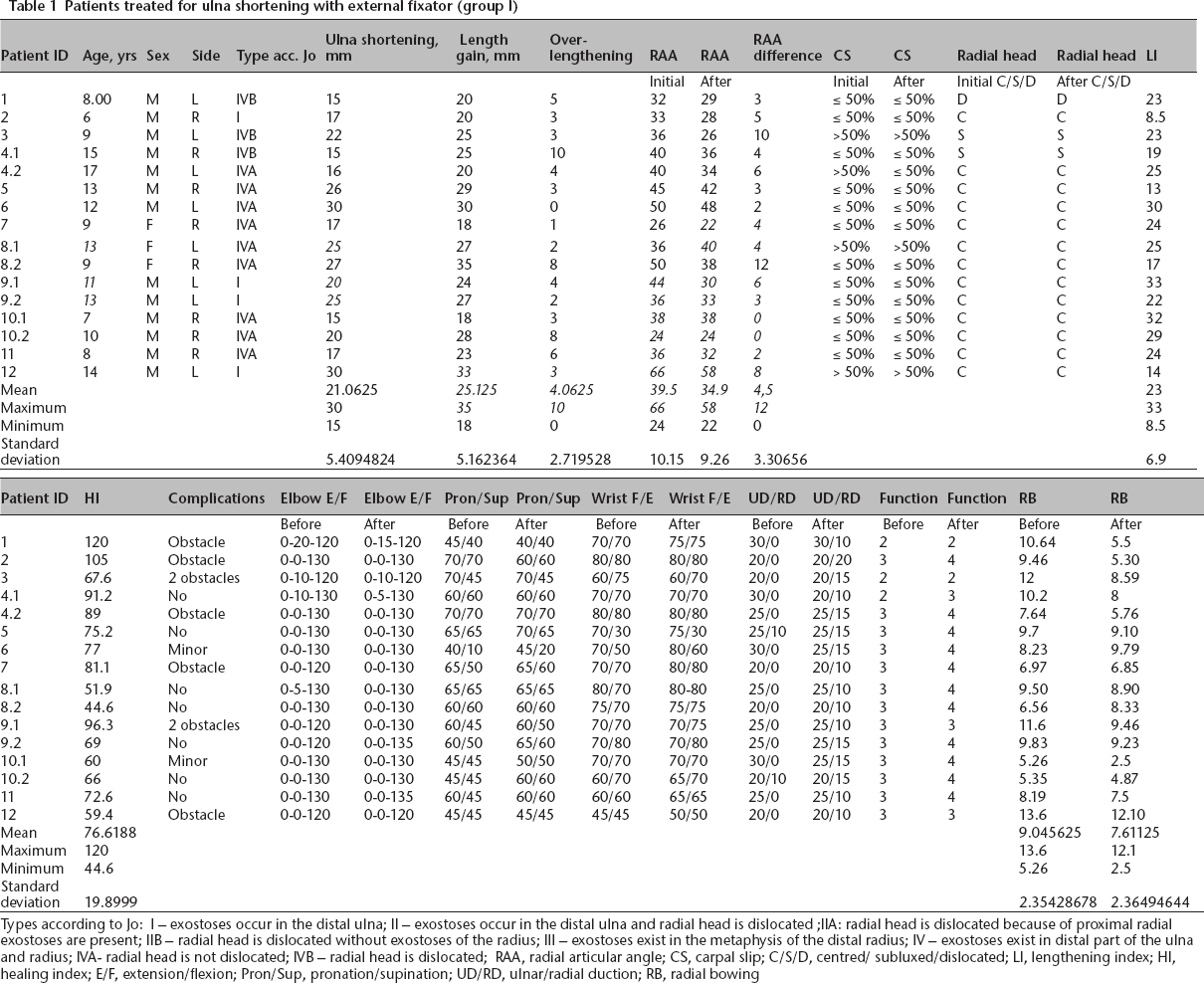
Types according to Jo: I – exostoses occur in the distal ulna; II – exostoses occur in the distal ulna and radial head is dislocated; IIA: radial head is dislocated because of proximal radial exostoses are present; IIB – radial head is dislocated without exostoses of the radius; III – exostoses exist in the metaphysis of the distal radius; IV – exostoses exist in distal part of the ulna and radius; IVA- radial head is not dislocated; IVB – radial head is dislocated; RAA, radial articular angle; CS, carpal slip; C/S/D, centred/ subluxed/dislocated; LI, lengthening index; HI, healing index; E/F, extension/flexion; Pron/Sup, pronation/supination; UD/RD, ulnar/radial duction; RB, radial bowing
Patients treated for ulna shortening by external fixator and intramedullary nail (group II)
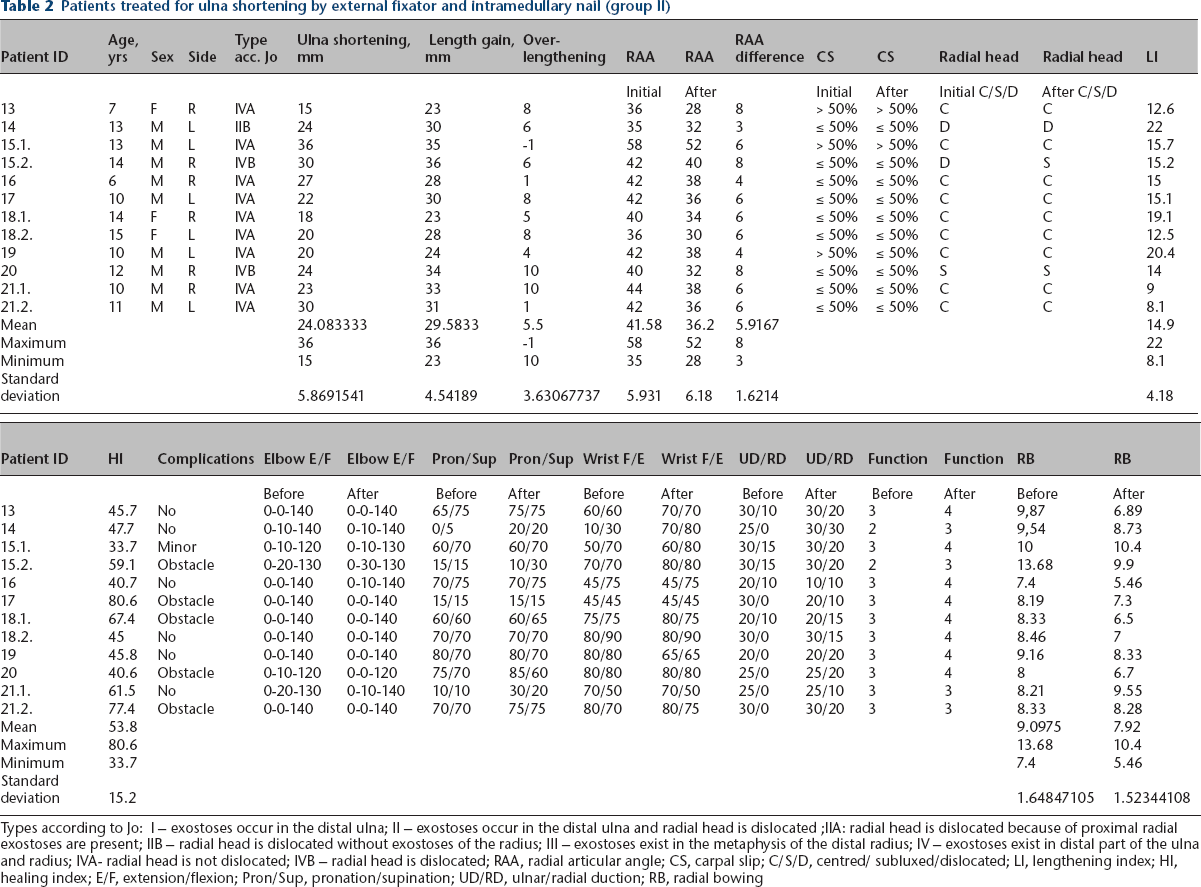
Types according to Jo: I – exostoses occur in the distal ulna; II – exostoses occur in the distal ulna and radial head is dislocated; IIA: radial head is dislocated because of proximal radial exostoses are present; IIB – radial head is dislocated without exostoses of the radius; III – exostoses exist in the metaphysis of the distal radius; IV – exostoses exist in distal part of the ulna and radius; IVA- radial head is not dislocated; IVB – radial head is dislocated; RAA, radial articular angle; CS, carpal slip; C/S/D, centred/ subluxed/dislocated; LI, lengthening index; HI, healing index; E/F, extension/flexion; Pron/Sup, pronation/supination; UD/RD, ulnar/radial duction; RB, radial bowing
Within the clinical assessment, subjective satisfaction (cosmetic concerns) and upper extremity function of MHE patients were evaluated according to Stanton and Hansen 10 , and range of movement (ROM) of the wrist and the elbow was compared preoperatively and after a minimum of three months following removal of the external fixator and physical therapy. Static ROM was measured using the goniometer in resting posture of the joints. Complications were recorded and classified according to Paley 11 as minor, obstacles or major. They were correlated according to the age of start of treatment using Spearman's correlation coefficient. The p-value 0.05 was chosen at the level of 95% significance.
Within the radiological assessment, standardized anteroposterior (AP) and lateral radiographs of the wrists, forearm and elbow were evaluated according to Burgess and Cates 12 prior to lengthening and after full consolidation of the regenerate. The parameters included (Fig. 1a): radial articular angle (RAA; the angle between the inclination of articular surface of the distal aspect of radius to a line perpendicular to the linear axis of the forearm in AP view), carpal slip (percentage of the lunate that is to the ulnar side of the continuation of the linear axis of forearm), ulnar shortening as the distance of the perpendicular drawn from the distal end of ulna to the linear axis and medial border of the radial epiphysis), radial bowing was calculated as the percentage of the maximal distance that the radial diaphysis deviates from the long axis of the forearm divided by the radial length and position of the radial head relative to the capitulum humeri (centred, subluxated, dislocated). The position of the radial head was evaluated according to the congruency of the foveola radii to the capitulum humeri. Classification of forearm deformities with MHE according to Jo et al 13 was used preoperatively in both groups (Table 1 and 2). The radiological parameters were measured by three authors (JC, MO, MF) and finally checked and corrected by the first author.
Statistical analysis
The difference between ulnar lengthening in group I (external fixator) and group II (external fixator and intrameduallry nail) was evaluated using a linear model with the generalized least squares method. The value 0.05 was chosen as the significance level. The following differences were compared: gain of ulnar length; bone lengthening index (days of lengthening for 1-cm gain); bone healing index (days of external fixation for 1-cm gain); RAA; and radial bowing. The results were obtained using the R statistical software with nlme package (Manufacturer: R Core Team, R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/).
Results
The data are presented in Tables 1 and 2. Preoperatively, shortening of the ulna ranged between 15 mm and 30 mm (mean 21 mm) in group I and 15 mm and 36 mm (mean 24 mm) in group II. The mean RAA did not differ between the two groups (39.6°, range 24-66° versus 41.5°, range 35-58°). Carpal slips over 50% were more common in group I (four forearms) than in group II (one forearm). In group I there was one dislocation and two subluxations of the radial head noted, while in group II there were two dislocations and one subluxation.
Postoperative clinical evaluation showed that cosmetic appearance improved in all patients. The overall satisfaction of the patients was negatively influenced by complications (see below) and radial head dislocation. The ROM of the wrist and elbow decreased during lengthening in all patients; but except for radial deviation, the difference between preoperative values and the values after full consolidation and physiotherapy was not significant in either group. Only radial deviation improved (mean 12° (0° to 30°; Standard Deviation 6.4°)). Subjective assessment of the upper extremity function improved in 13 forearms (81%) of group I and in ten forearms (83%) of group II. The improvement exceeded 1° of scale but no patients obtained full unrestricted function (grade V). The results did not differ between the two groups.
In terms of radiological parameters, the differences between the groups in length gain (p = 0.0319; Fig. 2), lengthening index (p = 0.0073; Fig. 3) and healing index (p = 0.0021; Fig. 4) were found statistically significant. Probability density plot for length gain, lengthening index and healing index are shown in Figures 2, 3 and 4, respectively. Continuous line represents group I and dashed line represents group II (external fixator and intramedullary nail). The mean amount of lengthening was 25.1 mm (18 to 35) in group I and 29.6 mm (23 to 36) in group II. The values in group II as compared with group I increased for length gain and decreased for bone lengthening and bone healing indexes. The difference of the bone lengthening and healing indexes was independent of the age of the patients.
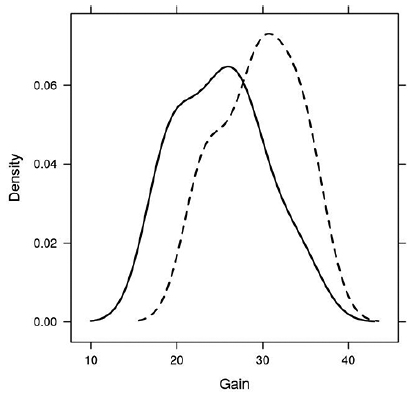
Probability density plot for gain: ulna lengthening external fixator group I (continuous) and ulna lengthening external fixator and intramedually nail group II (dashed).
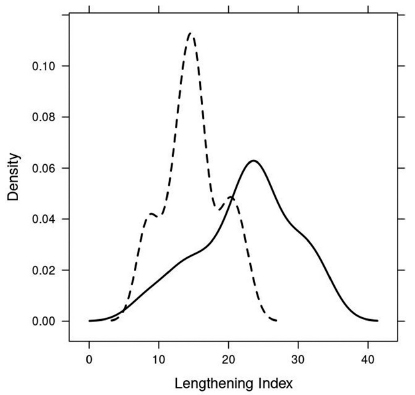
Probability density plot for lengthening index, ulna lengthening external fixator group I (continuous) and ulna lengthening external fixator and intramedually nail group II (dashed).
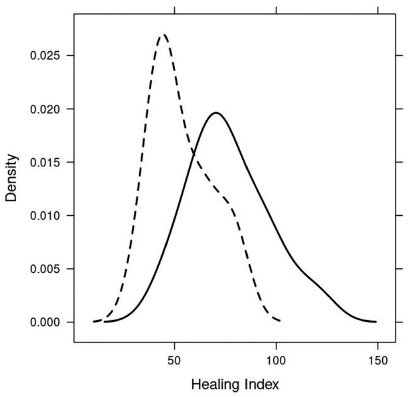
Probability density plot for healing index, ulna lengthening external fixator group I (continuous) and ulna lengthening external fixator and intramedually nail group II (dashed).
With regards to the other measured radiological parameters, the RAA decreased in both groups, namely 4.5° on average (0° to 12°) in group I and 5.9° on average (3° to 8°) in group II. There was no statistical significance between group I and group II to the achieved RAA (p = 0.39 > 0.05, which corresponds to the selected level of significance of 95%).
The RAA decreased by 5.2° on average (0° to 12°) in age under ten years and 4.9° on average (2° to 9°) in age over ten years. The statistical significance of belonging to a particular age group for the achieved value of RAA differences has not been proven (p = 0.75 > 0.05, which corresponds to the selected level of significance of 95%).
The mean radial bowing in group I decreased from 9.04 (5.26 to 13.6) to 7.6 (2.5 to 12.1) after surgery. The mean radial bowing in group II decreased from 9.10 (7.4 to 13.7) to 7.92 (5.5 to 10.4) after surgery. No statistical significance of belonging to group I or group II to the achieved radial bowing differences value has been demonstrated. (p-value = 0.61 > 0.05, which corresponds to the selected level of significance of 95%).
With regards to age, mean radial bowing decreased from 8.4 (5.3 to 12) to 6.8 (2.5 to 9.6) in the group under ten years and from 9.8 (7.7 to 13.7) to 8.7 (5.8 to 12.1) in the group over ten years. The statistical significance of belonging to a particular age group for the achieved value of radial bowing differences has not been proven (p = 0.4 > 0.05, which corresponds to the selected level of significance of 95%).
The carpal slip did not significantly decrease in either group (Tables 1 and 2). Overlengthening of the ulna was achieved in all but one forearm of both groups and varied between 1 mm to 10 mm (means 4 mm (group I) and 5 mm (group II), Tables 1 and 2). Position of the radial head did not change after lengthening, i.e. the radial head did not reduce to the humeroradial joint in cases of dislocations and it did not dislocate during or after lengthening in cases without preoperative radial head dislocation. There were no other attempts of reducing of radial head dislocations during the treatment.
Complications are shown in Tables 1 and 2. No major (permanent) complication was recorded. The incidence of minor complications (pin tract infection) was similar in the two groups, occurring in two forearms (13%) in group I and in one forearm in group II (8%). The frequency of obstacles differed between the two groups, with eight cases in group I (50%) and three cases in group II (25%). In group I, the obstacles included mostly nonunion of the regenerate that required additional internal fixation (three forearms, 19%); delayed consolidation of the regenerate in two forearms that were treated with cast immobilization; one severe pin tract infection necessitating removal of the external fixator; one axial deviation treated by surgical correction and internal fixation; and one fracture of the bone at the screw insertion. These complications resulted in loss of length of the regenerate. In group II, the obstacles included four cases of delayed consolidation of the regenerate (33%) treated with cast immobilization; one nonunion (8%) requiring reconstruction and internal fixation; and one elastic nail perforation with poor regenerate formation after its removal. Repeat lengthening had to be performed in two patients in group I 2.5 and three years after the first lengthening. The age of start of lengthening was 11 years and seven years in these patients (Table 1, patients 9.1 and 10.1). The complication rate did not correlate with the patient's age at the start of lengthening in both groups. The value of Spearman's correlation coefficient was 0.042, which is very weak. The hypothesis that this coefficient is zero has not been rejected (p = 0.84 > 0.05, which corresponds to the selected level of significance 95%) and, therefore, we consider the variables to be uncorrelated.
Discussion
The hypotheses of our study have been confirmed, i.e. combining the intramedullary fixation with the ulna lengthening significantly reduced the bone lengthening and healing indexes, as well as reduce the complication rate. These findings are in agreement with the study by Jager et al, 9 using the circular frame for lengthening.
Treatment of forearm deformities in MHE patients remains controversial. According to the literature reports, the main reason is limited experience due to relatively small groups of patients, and the use of different treatment methods. 5 Our results and complication rate are similar to those in the recently published studies14–17 based on the same treatment philosophy.
Criteria for ulnar lengthening and the optimal age for its performance have not been fully defined. We empirically use the following criteria: relative shortening of the ulna > 10 mm and the minimum patient's age six years, with or without functional impairment. Single-step lengthening using iliac bone graft and osteosynthesis with the plate is performed if ulnar shortening is between 10 mm and 15 mm and gradual ulnar lengthening when relative shortening of the ulna exceeds 15 mm. Unlike Abe et al, 18 we do not postpone the lengthening procedure until ten years of age. We accept the fact that then could be recurrence of the ulna shortening 0.25 cm/year before adolescence 19 possibly necessitating a second lengthening.
With regards to our clinical assessment, we have not shown any significant improvement in the ROM of the elbow, forearm or wrist after ulnar lengthening, except for radial deviation. This is in contrast to findings of some authors,14,15,20 but in agreement with Peterson 1 and others.2,16,21,22 We have found improvement in the cosmetic appearance, associated with the achievement of the proper length of the ulna and some improvement of upper extremity function on the Stanton's scale 10 in the majority of patients. The improvement exceeded 1° on the scale but full unrestricted function was never achieved. These results are comparable in both groups. In patients who had no improvement in function, lengthening was associated with some obstacle or with a pre-existing radial head dislocation or subluxation.
Lengthening and reduction of the ulna to the distal radio-ulnar joint can preserve function of the wrist as it prevents progression of the carpal slip. This fact was proved by a previous study using arthroscopy of the wrist. 23 Ulnar lengthening did not significantly correct the carpal slip, which contradicts the findings reported by some authors,14,20,24 but is in agreement with studies by other authors.1,2,18,25
With regards to the RAA, we observed some remodelling effects on the radius after ulnar lengthening, similar to previous authors.14,18,25 Reduction of the RAA of > 5° was seen in only seven cases (25%), and it did not depend on the age. We agree with Fogel et al 21 and others1,2 that a significant remodelling effect on the distal radial epiphysis did not occur. We cannot confirm the RAA improvement correlated directly to improvement in ROM. We confirmed radial bowing corrections in both groups, but differences between groups I and II were not statistically significant. We did not confirm the radial bowing correction in correlation to the age, but it is known from literature reports, spontaneous improvement of radial bowing is possible in patients in age under ten years. 17
As for the radio-humeral joint, we can confirm that removal of the distal ulnar exostoses and ulnar lengthening prevent radial head dislocation, because distal ulnar lesions and ulnar shortening are early identifiable risk factors for radial head dislocation. 26 The radial head remained located during ulnar lengthening. This correlates with the findings reported by Refsland et al 16 and Huang et al 15 but contradicts the study by Hill et al, 27 describing two dislocations of the radial head during the lengthening. We have not confirmed a stable reduction of the radial head during and after ulnar lengthening, which is in contrast to D'Ambrosi et al 14 but in agreement with the study by Hill et al. 27 According to our results, adequate lengthening or even overlengthening of the ulna alone cannot lead to reduction in radio-humeral joint. According to Huang et al, 15 reduction of the radial head is feasible if the initial ulnar lengthening starts with external fixation of the distal ulna and radius. We do not attempt to reduce the radial head dislocation using another surgical method because the patients/parents denied it due to relative satisfaction after ulnar lengthening and due to other problems with MHE in further anatomical locations and necessary surgical treatment.
The bone healing index was relatively high in group I (76.6 days/cm) and significantly lower in group II (53.8 days/cm). Our results are comparable with some studies8,17,20 but significantly longer in comparison with reports by Jager et al 9 and Tang et al. 24 Jager et al 9 reported the healing index of 22.2 days/cm using a combined external fixator and Elastic Stable Intramedullary Nail (ESIN) technique, and 32.0 days/cm with external fixation alone. We have no explanation for these differences comparing our results, but it is generally known that bone formation and healing index may depend on the patient's age, diameter of osteotomy site and body mass index. 8 Except for age, we did not record those parameters. One reason for longer healing index (longer external fixation time) in our cohort could be explained by a fear of the surgeons to remove the external fixator too early in order to prevent fracture of the bone regenerate. The bone healing index and the lengthening index were significantly lower in group II in comparison with group I. This could be explained by the greater stability of fragments achieved with the intramedullary nail and subsequent reduction of problems during the lengthening, because of less deviation of the fragments. Therefore, elongation was more effective within a shorter time, with lower lengthening index and better regenerate formation and, as a result, lower bone healing index (or external fixator index). The greater stability of fragments after elongation also allows for earlier removal the external fixator.
The complication rate in our study was comparable with studies of a similar design.4,16,26 Minor complications included mostly pin tract infections, while the most common complications were obstacles 11 (poor regenerate formation, nonunion and severe pin tract infection). No major or permanent complication was encountered. Complications were significantly more frequent in group I as compared with group II. We cannot explain the relative high rate of complications, mainly poor regeneration formation and pseudarthrosis. The potential prevention of these complications could be accomplished by reducing of the lengthening rate to 0.5 mm a day.
Regarding overlengthening of the ulna, no clear criteria have been defined. We recommend overlengthening of 0.5 cm to 1 cm in children under the age of 13 years to prevent the necessity of a repeat of lengthening. This corresponds to the recommendation of Abe et al 18 and Pritchett. 19 By contrast, Vogt et al 25 reported one unintended ulnar overlengthening with a subsequent ulnocarpal impaction syndrome and did not recommend this procedure. We did not encounter this complication.
This study has the following limitations. The first limitation is that it is a retrospective study of a relatively small group of patients within a relatively small geographical area with a population of ten million inhabitants. The second limitation is that the surgical procedures were carried out by four surgeons from one institution, so the effects of institutional bias may be possible.
In conclusion, we support ulnar lengthening by distraction osteogenesis if the ulnoradial discrepancy exceeds 15 mm: to prevent radial head dislocation; to stop the carpal slip and to improve the cosmetic impairment as well as to improve some degree of function of the wrist. Limitations of ulnar lengthening include: the impossibility of reduction or improvement of position of the radial head in case of its dislocation; a significant correction of carpal slip and inclination of radial epiphysis; as well as recovery of unrestricted function of wrist and elbow. Finally, we advise the combination of ulnar lengthening with internal fixation using a single intramedullary elastic nail, which provides a significant benefit in terms of the bone lengthening gain, bone healing index and the rate of complications.
Footnotes
MO: Data acquisition.
MF: Data acquisition.
PD: Drafting and revising the work.