
Abstract
Abstract
Introduction
Osteochondromas are usually found in the long bones of patients with hereditary multiple exostoses (HME). The spine is reported to be involved in over 50% of cases, but few of these patients are symptomatic as the result of an existing spinal exostosis.
Methods
We reviewed the current literature in order to find the right approach to patients with HME-complicated spinal exostosis and describe three paediatric patients that were diagnosed late with spinal cord compression due to cervical exostosis.
Results
Our three cases were all late presentations with neurology and unfortunately had minimal improvement of neurology after the lesion was surgically removed. There is general agreement that late presentation of spinal cord injury due to osteochondromas involving the cervical spine may cause severe and irreversible neurological sequelae. Our literature review revealed that there are no clear-cut guidelines to develop more comprehensive screening measures for these patients.
Conclusions
A high index of suspicion is the most important factor for correct diagnosis and appropriate management. Physicians who treat HME should bear in mind that thorough history taking and a neurological examination at follow up are essential for these patients. Clearer guidelines for the development of more comprehensive screening programmes are essential.
Level of evidence
IV
Introduction
Osteochondromas (exostoses) are the most common benign bone lesions, constituting 20–50% of all benign bone tumours and 10–15% of all bone tumours. 1 These osseous lesions have a cartilage cap and usually involve the metaphysis or diametaphyseal regions of the long bones. They are frequently encountered among young adolescents.2,3 Their clinical presentation is usually a solitary sporadic lesion, but they may also be multiple when they are associated with hereditary multiple osteochondromas. 4 Hereditary multiple exostoses (HME) is an autosomal dominant inherited musculoskeletal disease that occurs in the general population at a rate of 0.9 to 2.0 per 100,000.5,6 Patients with this disease have symptoms due to stiff and protruding superficial lesions, limb deformities and pressure on neurovascular bundles.7–9
Fewer than 5% of solitary osteochondromas originate in the spine.5,10,11,12,13 Spinal osteochondromas in patients with HME had traditionally been considered an uncommon phenomenon, ranging from less than 1% to 9% of all exostoses,14,15 but recent reports have shown an incidence reaching as high as 68%. 6 Most of the spinal lesions have special predilection for the posterior elements of the cervical or thoracic spine. 16 Diagnosis is invariably a challenge due to the gradual evolution, the wide variety of clinical presentations, and the poor demonstration on imaging studies.5,17 While most symptomatic spinal exostoses evolve slowly, several reports have shown that neurological deterioration might be rapid.6,18 The presenting symptoms of spinal osteochondromas are usually due to nerve root or cord compression with radicular pain, weakness, sensory dysfunction, and myelopathy.6,14,18 Rare cases, such as torticollis and hemiparesis due to vertebral artery occlusion, have also been described. 19 Bess et al recommended that the tumour should be excised surgically when it causes pain or neurological complications or when the diagnosis is unclear. 14
We report three paediatric cases of HME with cervical spine involvement, comprising what we believe to be the largest case series of paediatric cervical spine osteochondromas causing cord compression. We provide a review of the literature to clarify the clinical characteristics of spinal HME in the paediatric population.
Case reports
Case 1
A nine-year-old girl with HME and a strong family history presented with a limping gait and right drop foot. Plain radiography demonstrated exostosis in the right proximal tibia. The exostosis was excised, mostly from the posterior medial aspect of proximal tibia, and the peroneal nerve was explored one year later. There was no postoperative clinical recovery of the peroneal nerve. Nerve conduction studies performed one year later showed no evidence of sensory or motor abnormality within the right peroneal nerve. At the age of 12 years, the patient was referred to the senior author's clinic and the clinical examination revealed a hemiplegic gait and brisk reflexes on the right side. The neurological examination revealed numbness below the neck, in both hands, and in both legs, which worsened when the neck was flexed or extended. The findings of examinations of the central nervous system and higher mental functions were normal, as was cranial nerve function. Examination of the motor system revealed spasticity and wasting on the right side, which was more proximal than distal. Muscle power was +4/5 in the right upper limb and +4/5 in the right lower limb with the exception of dorsiflexion of her ankle. Strength on the left side was normal.
C-spine radiography did not show any obvious bony deformity. The MRI showed C1 exostosis arising from the left lamina causing cord compression. She underwent a C1 laminectomy and complete removal of the exostosis under general anaesthesia. There were no complications and no adverse events. The results of the neurology examination at discharge were the same as before surgery. The final pathologic diagnosis revealed a 2.5 cm exostosis.
At the 10-year postoperative follow up, her physical examination revealed a stable residual right hemiparesis, recurrent intermittent anisocoria, exaggerated reflexes, and clonus on the right side. Cervical magnetic resonance imaging (MRI) follow-up studies showed no recurrence of the lesion. The last MRI at age 19 years demonstrated an attenuated upper cervical cord with associated myelomalacia (Fig. 1).
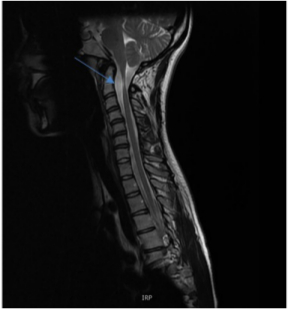
The last follow-up MRI at the age of 19 years demonstrated attenuated upper cervical cord with associated myelomalacia.
Case 2
A 12-year-old girl was diagnosed at the age of 18 months as having a spontaneous mutation HME. She had undergone multiple orthopaedic surgeries, including the removal of exostoses from bilateral proximal humeri and the left proximal ulna, as well as screw epiphysiodesis of bilateral distal medial tibias. She was referred to our clinic due to a limp that had appeared six months earlier and was getting worse, together with recurrent episodes of collapsing. Clinically, she had a type 1 hemiplegic gait on the right side, with lack of flexion in the swing phase. She is left-hand dominant, the right arm was internally rotated, the right elbow was flexed, and the right shoulder was slightly abducted and held in flexion. The neurological examination revealed normal sensation and motor function in both upper and lower limbs, brisk reflexes (particularly on the right side), a positive Hoffmann's sign and clonus (more than three beats) on the right side. The plantar reflexes were equivocal, and the Romberg test was negative. An X-ray of the cervical spine confirmed exostoses both at C3, which was intra-spinal, and at C2, which was extra-spinal. An urgent computerized tomographic (CT) scan demonstrated a significant exostosis coming off the C3 lamina, indenting the spinal cord slightly more to the right side, and comprising more than 50% of the cavity (Fig. 2).
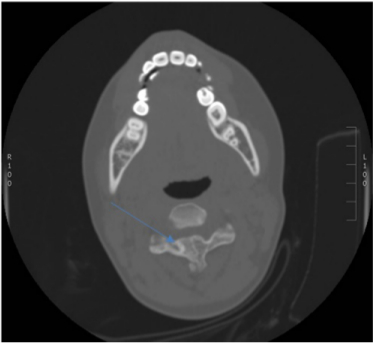
Exostosis coming off the C3 lamina, indenting the spinal cord and compromising more than 50% of the cavity.
An MRI scan confirmed a large posterior exostosis at levels C3/4 that was causing anterior displacement of the cervical cord with severe cervical cord compression and cord a T2 signal abnormality (Fig. 3). There was a small right anterior exostosis just touching the anterior and right side of the cord without cord compression or signal abnormality at T6/7. There was a small right exostosis at L3/4 that extended from the disc space into the right lateral recess, which just touched the traversing right L4 root. There was no evidence of compression of the cauda equina at this level.

MRI scan: C3/4 levels large posterior exostosis causing anterior displacement of the cervical cord with severe cervical cord compression and cord T2 signal abnormality.
The patient underwent a C3 laminectomy and excision of the C3/4 exostosis under general anaesthesia. There were no postoperative complications and no adverse events. At the two-year postoperative follow up, her gait and arm position had improved, but she was still walking with a short leg gait. She had no problems with coordination or altered sensation in her arms or legs, and the reflexes of her upper and lower limbs were brisk and symmetrical. Hoffman's sign was negative, clonus of the right foot was positive (three beats), there was no clonus of the left foot, the plantar reflexes continued to be equivocal, and Romberg's test was negative.
Case 3
A 13-year-old boy, who had been diagnosed with HME had undergone multiple excision surgeries for exostoses from his left scapula, right tibia, right ulna, left radius, and right distal femur. He was admitted to our department with complaints of progressive weakness, dizziness, and recurrent syncopial episodes during the last three years. He also had difficulties and significant pain while climbing stairs, walking, and self-care activities, such as washing his hair and personal hygiene, which were related to his multiple exostoses of the upper and lower limbs. He developed difficulties in bowel and bladder control, which were diagnosed as behavioural problems during the last few months before admission to our department. On physical examination, he had a good range of cervical motion, with a positive Lhermitte's sign. He had mild dizziness and became sweaty when standing up, both of which improved when he sat down. He had normal sensation and normal motor power, and all reflexes were present and symmetrical. Hoffman's sign and clonus tests were negative. A spine MRI showed two exostoses posteriorly at the level of C2 and C4, indenting the thecal sac, and causing cord compression and cord signal change, particularly at the C2 level.
The patient underwent surgery by our spinal surgical team for excision of osteochondromas from the anterior aspect of the C2 lamina on the right and the C4 lamina on the left. There were no complications and no adverse events after the surgical procedure. At the four-month postoperative follow up, the pain symptoms and weakness had improved significantly, with no change throughout a six-year follow up during which he had left leg mechanical axis correction by means of a Taylor spatial frame.
Literature review and discussion
Osteochondromas may develop as solitary or multiple lesions when associated with hereditary autosomal dominant multiple exostosis. These benign bony neoplasms derive from abnormal cartilaginous epiphyseal growth plate tissue, which proliferates independently from the normal growth plate. As growth progresses, this aberrant tissue flourishes as an early outgrowth of subperiosteal osseous with a cartilage cap that projects from the bone surface. 20 Osteochondromas that affect the spinal cord had been thought to be rare, even in patients with HME.9,21 The literature contains multiple case reports and small case series on spinal involvement, with an incidence of about 7–9% in the HME population,14,15 and about 1–4% in solitary osteochondromas.5,10,11,12,13 The lesions usually have a sessile appearance 2 and the posterior arch, lamina, pedicles, spinous or transverse processes are the most commonly affected sites, even though any part of the vertebrae can be involved. There are also reports of sporadic cases of osteochondromas arising from a lumbar facet joint.11,17
In a recent review of the English literature, Lotfinia et al reported that the male-to-female ratio in solitary cervical osteochondromas was 1.5:1.0, 21 and it is generally accepted that both multiple and solitary osteochondromas are more common in males than in females.22–25 Kamiya et al reviewed nine cases of cervical cord compression in paediatric patients with HME, among whom there were only two females. 26 Contrarily, Zaijun et al observed that female patients with solitary osteochondromas of the spine presented symptoms more often than male patients, 27 while Thompson et al 28 reported no gender differences. In our case series female patients were more affected than male patients. It is possible that different genetic aetiologies cause different phenotypes in patients with multiple hereditary exostoses, but the number of reported patients is too small to determine a higher morbidity for either sex. These lesions do not grow after skeletal maturity and they usually manifest clinically at a mean age of 20 years in the hereditary variety and 30 years in the solitary subtype.21,29
Spinal osteochondromas can occur at any part of the vertebral column, but they most frequently arise from the cervical vertebra (49%) followed by the thoracic and lumbar vertebra. 16 The most frequent site is the C2 vertebral bone, followed by C3 and C6.5,30 Two of the patients in our case series had additional lesions in the thoracic and lumbar spine, which were asymptomatic throughout the entire follow-up period. The clinical diagnosis of cervical exostosis in the HME paediatric population might pose a challenge to the healthcare provider as well as to the paediatric orthopaedic surgeon. These spinal lesions vary widely in their clinical manifestations, and their unspecific symptoms may lead to a delay between the onset of symptoms and the final diagnosis. 31 The most frequent presenting symptom is the palpation of a painless lump that occasionally causes mechanical compression and pain. 32 Albeit very rare, it can be associated with neurological symptoms, 33 and neurological signs can present as radiculopathy or myelopathy when the lesion involves the spinal canal.5,34–36
Most of the clinical presentations are gradual due to slow progress of the lesion in the neural canal 26 and owing to the large space available for the spinal cord at the level of C1–C7. 37 Acute symptoms may develop after a fall, accident, direct or indirect trauma to the cervical spine, with catastrophic results and even death. 38 Han et al described a case of a cervical osteochondroma presenting as Brown-Sequard syndrome after a mild trauma in a seven-year-old child with HME. 39 Less common symptoms due to anterior encroachment include dysphagia, hoarseness, sleep apnoea, cranial nerve palsy, Horner's syndrome, and torticollis.16,40 The only complaint of one of our three patients was dizziness and difficulty in walking and climbing stairs, although the neurological physical examination findings were within normal limits apart from a positive Lhermitte's sign. The presenting signs and symptoms of cord compression and myelopathy could potentially be confounded by the general complexity of the HME patient in whom multiple lesions affecting all the long bones might be interpreted as the cause for the neurological symptoms and signs of weakness and pain.
Kamiya et al recommended careful routine physical examination for all patients diagnosed with HME, especially for patients under the age of seven years who are not sufficiently cooperative to undergo an MRI without general anaesthesia.6,26 Roach et al used MRI scans to look for spinal column involvement in 44 HME patients (26 males and 18 females) who had no neurological symptoms. 6 They reported that 30 (68%) patients had exostoses arising from the spinal column, and 12 (27%) had lesions encroaching into the spinal canal. This suggested that the incidence of lesions within the spinal canal of patients with HME is much higher than commonly believed.
Thompson et al's MRI findings for 27 patients with HME showed only six (23.1%) patients with osteochondromas arising from the spinal column, and only three (11.5%) patients with encroachment into the spinal canal. They raised the possibility that there are different genetic aetiologies and different phenotypes of HME in different geographic regions. 28 Both of those groups of authors6,28 concluded that the diagnosis of spinal cord compression by an osteochondroma is picked up late because it is a slow growing lesion and because plain radiographs do not have enough resolution for accurate assessment and may therefore miss them.
Schmale et al 41 reported that multiple hereditary exostoses have a penetrance of 50% by the age of 3.5 years and nearly 100% by the age of 12 years. Accordingly, whole-spine MRI screening of patients diagnosed with HME at around the age of 10 years should detect most lesions.6,28
Many centres have followed the recommendations of Roach et al 6 to use MRI to screen all patients who have HME at least once when the patient is old enough to cooperate without the need for general anaesthesia. However, Jackson et al 42 recently published a large cohort study that evaluated spinal lesions in skeletally immature HME patients. They retrospectively reviewed 227 HME patients and found spinal lesions in only 8 of the 21 patients who were screened (MRI or CT scan) (38.1%, 3.5% overall). From this small group only one patient (4.8%, 0.4% overall) was symptomatic and underwent excision of the spinal lesion. In the conclusion they argued against routine advanced imaging screening (MRI/CT scan) for all patients. They recommended patient education regarding symptoms of spinal cord compression and limiting advanced imaging to patients with highly suspicious neurological symptoms and those with higher tumour burden. Since not all patients are screened and some who are screened with only plain films would likely have lesions that are missed, we do not really know the frequency of spinal lesions nor of lesions in the different regions of the spine. Furthermore, five of the nine paediatric HME patients reviewed by Kamiya et al 26 were seven years old or younger when diagnosed with cervical cord compression. Roach et al 6 had reported that six of the patients with encroaching lesions underwent surgical excision, of them, three were 5.8, 6.5 and 9.5 years of age. Moreover, one of their 12 patients who had a lesion indenting the dural tube was 5.5 years old and another patient was 4.17 years old. CT scans take less time to perform and no anaesthesia is needed, but they involve potential risks of radiation exposure and the cartilaginous cap, which can be quite large in young individuals, would not be outlined. 28 Thompson et al 28 suggested a limited sagittal survey of the entire spine, which takes less time, potentially requires less sedation, and may be a quick screening imaging modality.
One of our patients presented with long-standing dizziness and difficulty in climbing stairs, which were attributed to his other multiple bone lesions and to a behavioural disorder. He was examined by two expert neurologists who found no obvious clinical findings. Only a high index of suspicion led us to perform a spinal MRI under anaesthesia in order to arrive at the correct diagnosis. Although it is a common problem, neck pain in the paediatric population mandates exclusion of a serious underlying pathology and in clinical decision making regarding the extent of the required workup, especially in a high-risk population. 43
Spinal screening with MRI is an excellent imaging modality and should be considered when clinically there is suspicion of any neurological symptomatology, especially before patients undergo surgical excision of other bone tumours under general anaesthesia with an increased risk of traumatic myelopathy. In 2014, Fernandes et al (the senior author) suggested that patients with achondroplasia who were undergoing limb lengthening should be screened for spinal stenosis. Those authors emphasized the importance of a high index of suspicion, a comprehensive neurological examination and a very low threshold for noninvasive imaging, such as a CT scan and an MRI study. 44 When MRI is not feasible, a high index of suspicion, a thorough history taking, and a careful physical examination are irreplaceable. We believe that, equally to the achondroplasia patients, it is imperative that higher level of suspicion and low threshold for obtaining sophisticated imaging should be the core tool for the management of the young patient with HME. Routine spinal MRI is not shown to be mandatory and as demonstrated, if it is carried out after the age of five years many patients are missed and the power of this screening tool is weakened significantly. In contrast to Jackson et al's literature review 44 who reported that 92% of patients with neurological symptoms completely recovered, all three of our cases were late presentations and unfortunately had minimal neurological improvement after the lesions were surgically removed. Therefore it is extremely important that the treating physician focuses on patients with higher burden of disease or with symptoms.
Even though the limitations of our study are obvious due to the small case series and the lack of power to recommend on guidelines, this is an interesting red flag and awareness raising report with a conclusion that late presentation of spinal cord compression due to osteochondromas involving the cervical spine may cause severe and irreversible neurological sequelae. At each visit, physicians who treat HME should carry out a targeted history and clinical examination of neurological symptoms and signs, as an essential clinical screening tool. Clearer guidelines for the development of more comprehensive screening programmes are required, especially regarding whether spinal imaging should be used as a baseline for HME-affected children.
Footnotes
BTK: Collecting data and writing
AC: Writing.
JAF: Review of literature and writing