
Abstract
Purpose
In myelomeningocele, several classifications have been used. The present manuscript proposes a new functional classification to better assess the prognosis and management of these patients.
Methods
The manual muscle test is what defines the actual group in which the patient should be included. Furthermore, this new classification brings information about the bracing and external supports recommended to each functional level. We also recommend that the patient's Functional Mobility Scale should always be mentioned together with their functional level.
Results
The four levels in this classification are MMFC1, MMFC2, MMFC3 and MMFC4. The MMFC1 group includes patients with significant muscle weakness. They need to use high braces crossing the hip joint with a walker to achieve some ambulation. The MMFC2 group includes patients who have functional hip flexors, knee extensors and knee flexors. However, the hip abductors are quite weak. These patients usually need to use a walker - or crutches - and Ankle-Foot Orthosis (AFOs). The MMFC3 group includes patients with functional hip flexors, knee extensors, knee flexors and hip abductors. However, the ankle plantar flexion function is absent. Most of them are able to walk independently, only using AFOs without any external support. The MMFC4 group includes patients who have preserved function in the entire lower limb musculature. These patients don't need any assistive devices to achieve an adequate ambulation pattern.
Conclusions
We hope that this new classification is a system that is simple to understand, serves as a gait prognosis guide and facilitates communication among healthcare professionals.
Level of evidence
V
Introduction
In orthopaedic surgery, several classifications have been created to facilitate the understanding of diseases and the communication among surgeons and healthcare professionals. An effective classification system must be easy to understand, have a good inter- and intraobserver reliability, predict prognosis and be able to guide treatments.1–6
In paediatric orthopaedics, several classification systems have been used successfully. For example, for Legg-Calvé-Perthes, the lateral pillar classification by Herring et al7,8 has four easy-to-reproduce groups that efficiently assist communication between surgeons and predict prognosis. For proximal femoral focal deficiency, Aitken 9 proposed a classification into four groups, which is easy to interpret and also helps the surgeon in terms of prognosis and choice of treatment.
Within the neuromuscular population, two important functional classification scales have been introduced: the Gross Motor Function Classification System 10 and the Functional Mobility Scale (FMS) 11 (Fig. 1). These classifications are simple to interpret, have great prognostic value and are helpful in the formulation of the treatment plan.
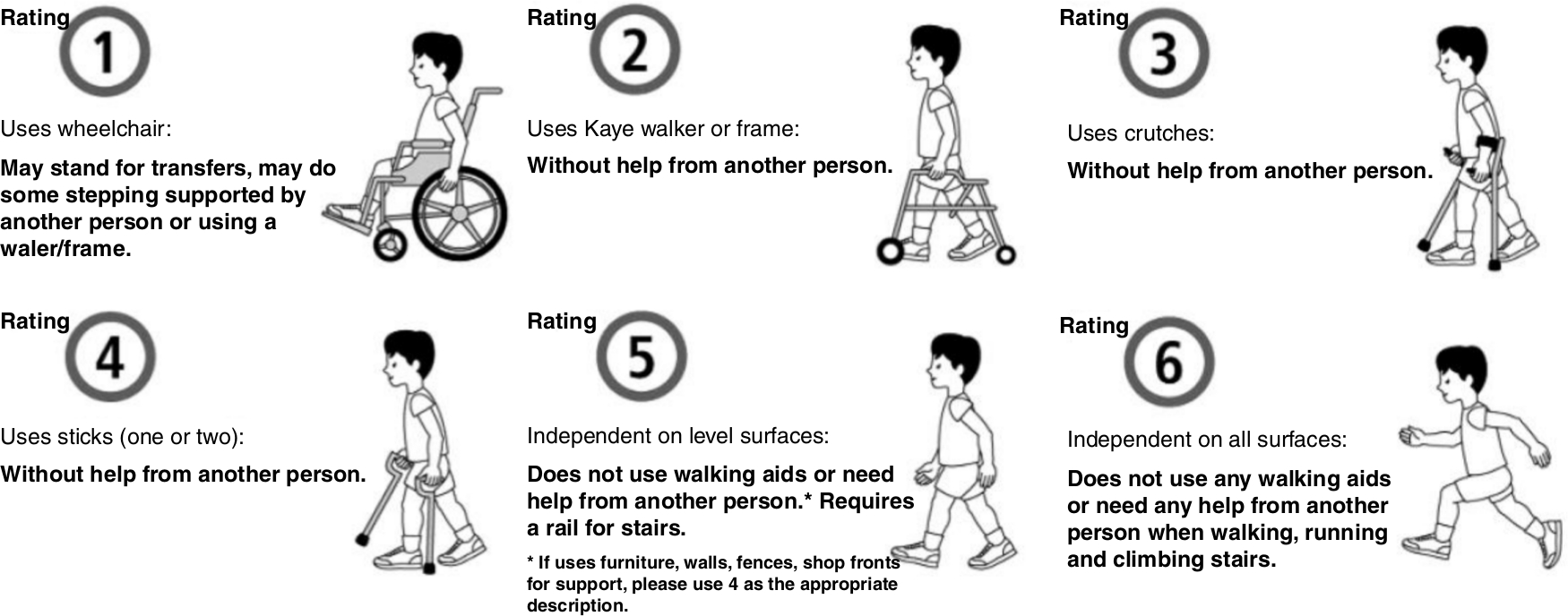
Functional Mobility Scale (FMS) classification patients rated at 5 m (e.g. home), 50 m (e.g. school) and 500 m (e.g. shopping mall). A rating of 1, 2, 3, 4, 5 or 6 is given for each distance (reproduced with permission from Kerr Graham) 21
For the diagnosis of myelomeningocele (spina bifida), several classification systems have been created in an attempt to classify the different clinical and anatomical aspects of the disease.12–18 Sharrard, 12 Lindseth, 17 Ferrari et al 18 and Broughton et al 14 have all developed classification systems dividing patients into seven to nine subgroups, using the anatomical terms thoracic, lumbar and sacral. Hoffer et al 13 proposed a division of patients with myelomeningocele into four functional categories: community ambulator, household ambulator, nonfuctional ambulator and nonambulator. McDonald et al 15 proposed a classification system to predict patients’ ability to walk from the assessment of muscle strength. Bartonek et al 19 published a review of these classification systems and concluded that there was incompatibility between the anatomically based and the functional ambulation-based classifications. In other words, the same lesion levels described in the different classifications do not correlate to the actual ambulatory function of the patients. It is important to mention that Bartonek et al 19 did not include the classifications proposed by Schafer and Dias 20 in 1983 and Swank and Dias 16 in 1994 in the analysis.
In 2009, our group proposed the use of a functional classification combined with the FMS (Table 1).11,21 This system is inclusive of the muscles that are strong, the types of external support and braces that are indicated for each functional level, as well as the distance that the patient might be able to walk. The inclusion of the FMS scale within a myelomeningocele classification system allows for the quantification of the patient's functionality, which helps the healthcare team communication and understanding of the disease evolution in every single patient.
Swaroop and Dias Spina Bifida classification (2009) 22 (adapted with permission from L. S. Dias)
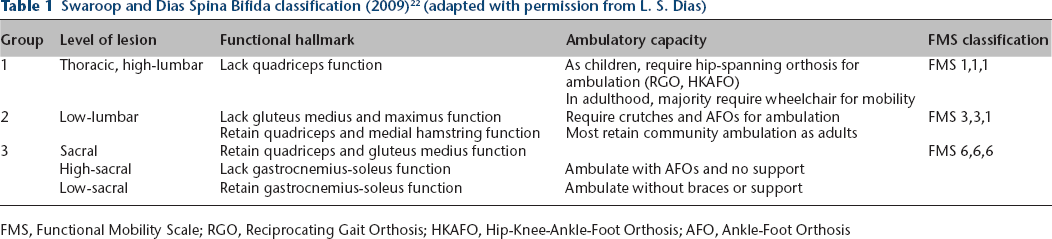
FMS, Functional Mobility Scale; RGO, Reciprocating Gait Orthosis; HKAFO, Hip-Knee-Ankle-Foot Orthosis; AFO, Ankle-Foot Orthosis
While there are many published classifications for myelomeningocele, there is not one unifying or universal system that integrates qualitative and quantitative information about the functionality level of each patient. Based on an adaptation of our last classification system, 22 which Rethlefsen et al 23 has shown to have excellent correlation with the patient's ambulatory function, we propose a new classification that can provide the gait prognosis, facilitates patient care decision-making process and enhances communication among healthcare professionals.
Materials and methods
Our clinical experience of over 45 years suggests that an ideal classification system for myelomeningocele should:
reflect the functional capacity of the patient;
have few classification levels;
avoid anatomical nomenclature.
We propose the inclusion of the assessment of muscle strength based on the manual muscle test 24 (MMT), ideally done by a physiotherapist. This evaluation is what defines the actual level in which the patient should be included. Based in our experience in gait analysis in the last 30 years, the muscle evaluated is considered functional if its strength is greater than or equal to 3, except for the medial hamstrings and the gluteus medius, which are considered functional if muscle strength is greater than or equal to 2. Thus, the muscle is considered functional if it is able to assist in some way in the patient's gait. Furthermore, this new classification brings information about the bracing and external supports recommended to each functional level.
To facilitate communication, we suggest some changes in how to express the patient's functional level. Instead of using the anatomical level of the spinal cord lesion, as has been done before by several authors,12,15,16,22 we propose the use of a numerical graduation from 1 to 4. Because healthcare professionals tend to abbreviate the term myelomeningocele using the acronym ‘MM’, the four levels in this classification are MMFC1, MMFC2, MMFC3 and MMFC4 (i.e. Myelomeningocele Functional Classification). We also recommend that the patient's FMS 11 should always be mentioned together with their functional level.
It is relevant to mention that this classification system is dynamic. It may change due to tethered cord complications, shunt malfunction followed by infection and severe orthopaedic deformities that prevent the use of braces.21,23,25,26
Therefore, the classification should be as follows (Table 2).
The Myelomeningocele Functional Classification (MMFC)
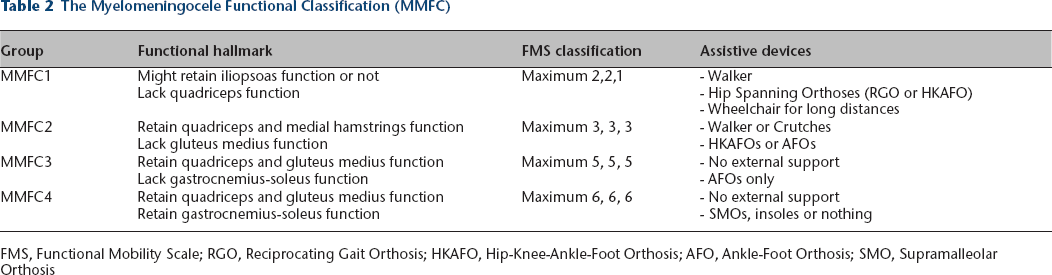
FMS, Functional Mobility Scale; RGO, Reciprocating Gait Orthosis; HKAFO, Hip-Knee-Ankle-Foot Orthosis; AFO, Ankle-Foot Orthosis; SMO, Supramalleolar Orthosis
Results
MMFC1
This group includes patients with significant muscle weakness. The hip flexor strength, represented by the iliopsoas muscle, may be present, but these patients do not have significant quadriceps strength. They need to use a Reciprocating Gait Orthosis or a Hip-Knee-Ankle-Foot Orthosis to achieve some ambulation. Most of them will need a walker as an external support, and some might be able to use even crutches depending on their level of coordination and balance. 27 However, some may be unable to walk due to a poor sitting balance. 20
Regarding the FMS, most of them will be 2/2/1 when young, i.e. under the age of 11 years old. As they gain weight and get older, which results in high energy cost for ambulation, they might become 2/1/1 and, invariably, by the age of 11 to 13 years old, they will become 1/1/1. Few exceptions are seen. For example, the senior author (LD) knows at least three MMFC1 patients that are FMS 3/3/1.
Our clinical experience suggests that patients can be classified within this level as early as birth when the newborn child shows no active movement of the entire lower limbs.
MMFC2
This group includes patients who have preserved hip flexor and knee extensor strength. The medial hamstrings present, at least, a muscle strength grade 2, which prevents excessive anterior pelvic tilt. 27 However, the function of the hip abductors, represented by the gluteal muscles, is not significant, i.e. less than grade 2 on MMT. These patients need to use a walker and Ankle-Foot Orthosis (AFOs) usually before the age of four, and crutches and AFOs thereafter. As the hip abductors strength is not present, it is very unusual for these patients to achieve a good ambulation pattern without using an external support. 27 For these children, the effectiveness of the ambulation pattern could be best determined by an instrumented gait analysis evaluation.
Regarding the FMS, most of them will be 3/3/3, 3/3/2 or 3/3/1 when young, usually before the age of 13. As they get older and gain some weight, they might become 3/2/1, 2/2/1 or 2/1/1.
Based on our experience, we cannot predict with certainty this functional level until the patient is at least four years old.
MMFC3
This group includes patients with preserved hip flexor strength, knee extensor and flexor strength and hip abductors strength, represented mainly by the gluteus medius function. However, the ankle plantar flexion function, represented by the gastrocnemius and soleus muscles, is absent. Most of them are able to walk independently, only using AFOs without any external support. However, depending on the degree of their gluteus lurch, a few might benefit from the use of crutches for long distances. 27
Regarding the FMS, most of them are 5/5/5, 5/5/3 or 5/3/3. As adults, they might become 5/5/1 or 5/3/1.
Similar to the MMFC2, this level cannot be predicted until the age of four. An instrumented gait analysis should be recommended to evaluate their ambulatory status.
MMFC4
This group includes patients who have preserved function in the entire lower limb musculature, including the ankle plantar flexors. These patients don't need any assistive devices to achieve an adequate ambulation pattern. However, some might benefit from the use of a Supramalleolar Orthosis or insoles to maintain a good foot alignment.
Regarding the FMS, they are 6/6/6.
Similar to the MMFC1, this level can be predicted in the newborn period.
Discussion
Several classifications for myelomeningocele have been developed in the past but there is no clear agreement among the anatomical levels proposed by these different classification systems. 19 It should also be noted that many of these classifications do not take into account the patient's functional capacity as the main factor.4,19,23,28,29 When referring to a patient with lumbar myelomeningocele, for example, the reader may not understand exactly which of the numerous lumbar levels already proposed the author refers to.12,15,16 Also, the patients’ grouping by anatomical level can generate misunderstandings, since, for example, several lumbar level patients may have different functional levels. Thus, within the same anatomical group, we can include patients who have no gait prognosis and patients who can walk without assistive devices.
As previously mentioned, Rethlefsen et al 23 demonstrated that the anatomical classifications, like the International Myelodysplasia Study Group's functional neurological level and lesion level on radiograph findings, were less descriptive of ambulatory mobility than our functional classification, 22 which is based on muscle function, braces and assistive devices used.
Furthermore, in 2015, Bisaro et al 30 showed that there are at least 19 measures that have been used to examine walking in children with myelomeningocele, and that there is still no system that is universally used to categorize the ability to walk in these patients. This hinders communication among healthcare professionals, prevents the formulation of standard treatment guidelines and undermines the performance of systematic reviews to assess the results of treatments performed in this population.
We believe that the functional classification, using a numerical scale in conjunction with the FMS, is efficient in predicting gait prognosis, assisting in management decisions and facilitating communication among healthcare professionals. For example, when referring to a six-year-old boy that has a grade 3 gluteus medius strength but does not have strength in the plantar flexors, and can walk independently at home and school using only AFOs, but needs crutches for long distances, we would classify him as an MMFC3 - FMS 5/5/3.
In addition, information about the maximum level expected in the FMS and the recommendations about the assistive devices provide practical guidelines for less experienced professionals. This can improve the understanding of the gait prognosis of each functional level and the counselling of family members regarding the ability to walk expected for each child.
Our clinical experience suggests that this scaling approach is dynamic in nature. The functional level can change with time, as mentioned before, due to several factors like tethered cord syndrome, shunt malfunction and severe orthopaedic deformities.21,25,26 One should always be aware that classification level changes may be a sign of a complication, which should require additional investigation.
In conclusion, as demonstrated earlier,16,19,22,23,30 the best classification systems rely on a functional grouping. This is even more essential in myelomeningocele, since what guides the patient's treatment is their functional capacity and not the anatomical level of their spinal cord lesion. We hope that this new functional classification brings a system that is simple to understand, easy to apply in clinical practice, serve as a gait prognosis guide and facilitates communication among healthcare professionals, generating a positive impact in patients’ care.
Footnotes
OA licence text
VTS: Study design, Manuscript preparation, Manuscript review.
LRAdA: Manuscript preparation, Manuscript review.
JEL: Manuscript preparation.
A-MR: Manuscript preparation.
TK: Manuscript preparation, Manuscript review.