
Abstract
Abstract
Purpose
This study was performed to evaluate a modified method of reconstructing the thumb abduction function in children undergoing surgical treatment of thumb duplication.
Methods
This retrospective study included 33 children (38 thumbs) with Wassel type III to VII thumb duplication who underwent excision of the polydactylism and osteotomy of the preserved thumb. Among them, 16 children (19 thumbs) underwent reconstruction of the attachment of the articular capsule and collateral ligament of the metacarpophalangeal joint, abductor pollicis brevis and flexor pollicis brevis by the anchor technique (Group A), while 17 children (19 thumbs) underwent suturing the attachment of the above-mentioned soft tissues to the periosteum (Group B). All children were followed up for six years after surgery. The appearance, function and joint stability of the preserved thumb were compared between the two groups; the bone alignment and development were observed.
Results
The deformity rate of preserved thumbs and the positive rate of lateral stress test were significantly lower in Group A than B (p < 0.05). The modified Tada score and the distance of first web were significantly higher in Group A than B (p < 0.05). Flexion, extension, adduction, abduction and palmar movement of the thumbs were good; bone alignment and development were good and no osteophyte or anchor shadow was left in the preserved thumbs in Group A.
Conclusion
Reconstruction of the abduction function using the anchor technique is effective in children undergoing surgical treatment for Wassel type III to VII thumb duplication and it may be superior to the conventional technique.
Level of evidence
III
Keywords
Introduction
Thumb duplication is a common congenital hand deformity with an incidence of 0.1%1,2 and is usually treated by surgery. Surgical treatment of thumb duplication should not simply involve excision of the polydactylism but bone alignment, joint stability, function and the appearance of the preserved thumb should be ensured to as great extent as possible.3–5 Therefore, the metacarpal, phalange, articular capsule, collateral ligament, muscle and tendon of the thumb should be carefully reconstructed during surgery. Improper treatment of these tissues may lead to secondary deformities of the thumb, such as poor alignment, first web contracture, a residual in the preserved thumb and nail deformity. 6
However, surgical treatment of Wassel type III to VII thumb duplication in particular results in complications such as deflection deformity, poor joint stability and poor abduction function of the thumb 7 (Fig. 1). This may be related to scar contracture, deformity of bone development, improper reconstruction of soft tissues and tissue imbalance after reconstruction. 8 Especially, if the reconstruction of the joint capsule is not reasonable, collateral ligament, muscle and tendon may affect the appearance and abduction function of the preserved thumb. Research has shown that the reason for needing a second surgery for Wassel type III to VII thumb duplication was to loosen the soft-tissue sutures or because of failure to reconstruct the original attachment in the first surgery. 9 Therefore, it is of particular importance to firmly fix the articular capsule, collateral ligament, abductor pollicis brevis (APB) and flexor pollicis brevis (FPB) to ensure successful reconstruction of the abduction function in children undergoing surgical treatment of Wassel type III to VII thumb duplication.
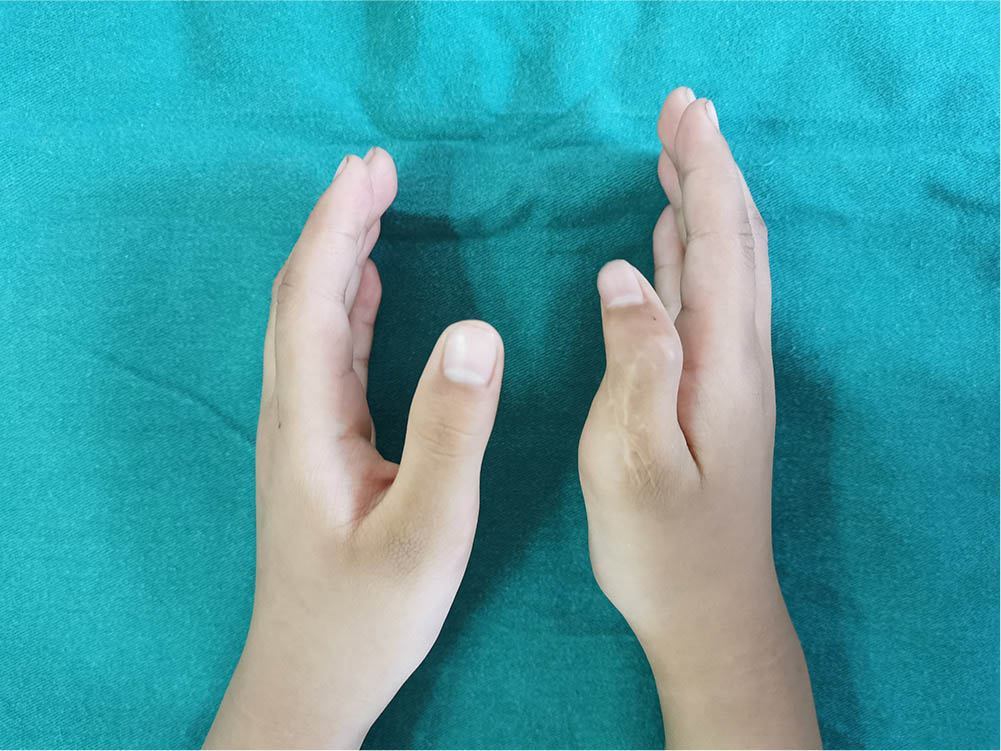
Deformity after traditional surgery.
The absorbable anchor is an extraordinarily small implant which can be firmly fixed in the bone. Thus, the soft tissues can be effectively reconnected by the suture of the anchor and the attachment can be firmly fixed in the original anatomical position, which is in line with the biomechanical requirements. This technique has achieved good results in the reconstruction of different tendons and ligaments of hand in adult.10,11 Therefore, for the children undergoing surgical treatment of thumb duplication, we also used the anchor technique to reconstruct the attachment of the collateral ligament and joint capsule of the metacarpophalangeal (MCP) joint, APB and FPB in order to restore the abduction function of the preserved thumb. In this study, we compared this technique with the traditional method of suturing the attachment on the periosteum to evaluate whether the modified method can effectively reconstruct the thumb abduction function.
Materials and methods
The inclusion criteria were: age one to four years; Wassel type III to VII thumb duplication; thumb duplication with ulnar dominance; need to reconstruct the thumb abduction function; and need for metacarpal or phalangeal osteotomy.
The exclusion criteria were: age less than one or more than four years; Wassel type I or II thumb duplication; thumb duplication with radial dominance; and no requirement for osteotomy.
Between 01st January 2013 and 31st December 2014, 38 children (45 thumbs) with Wassel type III to VII thumb duplication in this retrospective study underwent excision of the polydactylism, osteotomy and abduction function reconstruction of the preserved thumb. Among them, 18 children (22 thumbs) underwent reconstruction of the attachment of the articular capsule and collateral ligament of the MCP joint, APB and FPB by the anchor technique (Group A) between 01st January 2014 and 31st December 2014, while 20 children (23 thumbs) underwent suturing of the attachment of the above-mentioned soft tissues to the periosteum (Group B) from 01st January 2013 to 31st December 2013.
Two children (three thumbs) were lost to follow-up in Group A, while three children (four thumbs) were lost to follow-up in Group B; the remaining were followed up for six years.
Group A
This group included 16 children (19 thumbs) aged 2.23 years (sd 0.71) (1 to 4 years). There were 11 male and five female patients; eight right hands, five left hands and three bilateral hands. In terms of Wassel classification, 12 two thumbs were type III, ten thumbs were type IV, four thumbs were type V, two thumbs were type VI and one thumb was type VII; all were ulnar-dominant thumbs and required reconstruction of thumb abduction function.
Group B
This group included 17 children (19 thumbs) aged 2.19 years (sd 0.70) (1 to 4 years). There were ten male and seven female patients; nine right hands, six left hands and two bilateral hands. In terms of Wassel classification, one thumb was type III, 11 thumbs were type IV, four thumbs were type V, two thumbs were type VI and one thumb was type VII; all were ulnar-dominant thumbs and required reconstruction of thumb abduction function.
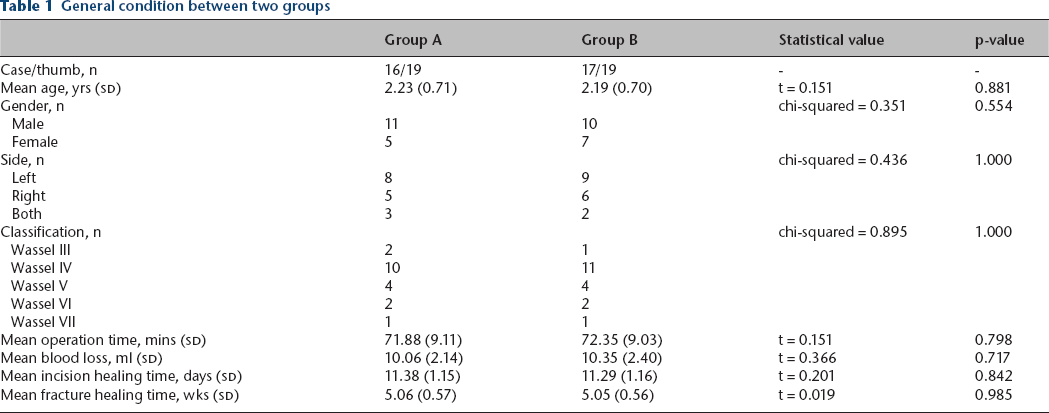
Physical and radiographic examinations were performed before surgery to confirm that the dominant thumb was on the ulnar side and the radial thumb required excision (Figs 2 and 3). All the surgeries were performed by YY and there was no significant difference in general information between the two groups (p > 0.05) (Table 1).

Preoperative appearance.

Preoperative radiograph.
General condition between two groups
Surgical procedure
All the children had basic anaesthesia combined with brachial plexus anaesthesia.
A U-shaped incision was made on the radial side of the polydactylism. Then a proximally-based U-shaped flap was taken to be the longest and as much fascia as possible was retained. After the flap was raised, the articular capsule and collateral ligament of the MCP joint, APB and FPB were dissociated from distal to proximal, then a wide rectangular fascia flap was formed. The radiographs of both hands were compared to calculate the osteotomy angle of the preserved thumb. After removing the polydactylism, the inclined metacarpal was corrected by a V-shaped osteotomy in the metacarpal neck in order to get it in alignment and the hypertrophic metacarpal head was partially excised at the same time. 13 The fracture was fixed with one or two Kirschner-wires (1.0 mm2) (Fig. 4). The reconstruction method of abduction function of thumb was as follows in Group A. An absorbable anchor (Microfix, 1.6 mm; Depuy Mitek, Raynham, MA, USA) was fixed 0.2 cm away from the radial epiphysis of the proximal phalanx basement. The direction was perpendicular to the phalanx, which was just the attachment of the articular capsule and collateral ligament of the MCP joint, APB and FPB. The soft tissues mentioned above were adjusted to ensure that the thumb was in the abduction and opposition position. The joint capsule and collateral ligament were sutured with one thread-end in the deep layer, while the APB and FPB were sutured in the superficial layer with the other thread-end. A lateral stress test of the MCP joint was then performed in order to check whether the soft tissues were firmed (Figs 4 to 6).

Intraoperative reconstruction of the articular capsule and collateral ligament of metacarpophalangeal joint, abductor pollicis brevis and flexor pollicis brevis by anchor technique.
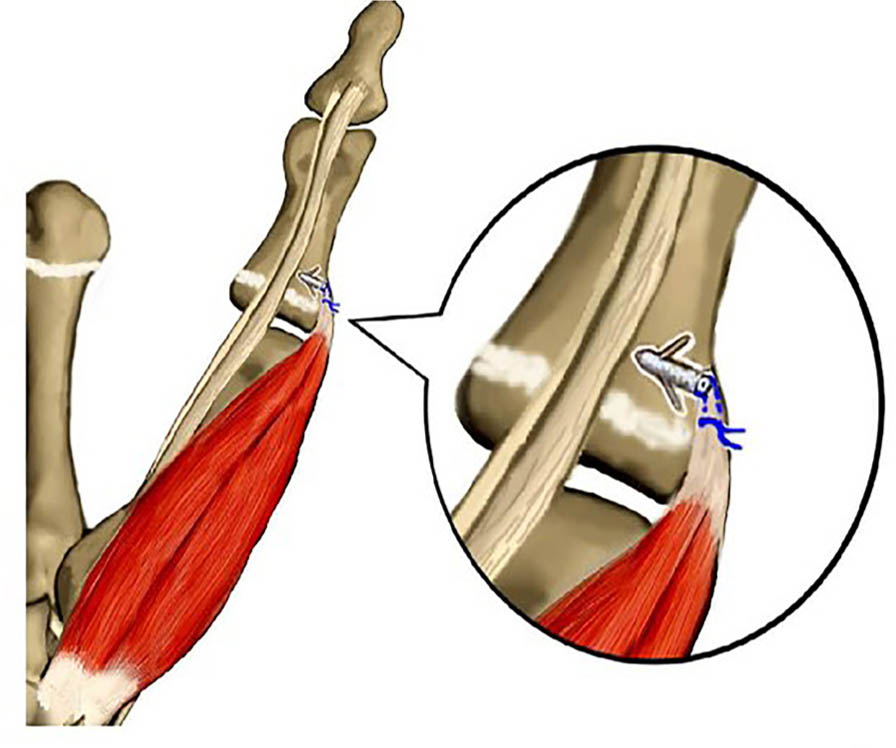
Schematic diagram of anchor technique.

Appearance immediately after surgery.
In Group B the dissociative articular capsule, collateral ligament, APB and FPB were adjusted to ensure that the thumb was in the abduction and opposition position. The broken ends of the soft tissues above were sutured with 5-0 Prolene (Ethicon, San Lorenzo, Puerto Rico, USA) in an 8-character pattern to the periosteum of the attachment, which was 0.2 cm far away from the radial epiphysis of the proximal phalanx basement. A lateral stress test of the MCP joint was then performed in order to check whether the soft tissues were firmed.
For the Wassel IV-D type thumb duplication, when the soft tissues were treated, we extended the incision to the distal end of the preserved thumb and explored whether the attachments of the flexor pollicis longus (FPL) and extensor pollicis longus (EPL) were in the centre of the distal phalanx basement. Usually the FPL and EPL were divided into two bundles to the polydactylism and preserved thumb, respectively, and the attachments of the preserved thumb deviated from the centre. So it was also necessary to translocate the FPL and EPL of the polydactylism to the preserved thumb to reconstruct the attachments in order to strengthen the force. 14 In our study, all thumbs were ulnar dominance and the attachments of the FPL and EPL were located on the radial side of the distal phalanx basement in the preserved thumb. Then the bundles of the FPL and EPL from the polydactylism were pulled to the ulnar of the distal phalanx basement in the preserved thumb through a subcutaneous tunnel. In Group A, an absorbable anchor was fixed on the palmar/dorsal of the ulnar base of the distal phalanx, which was 0.2 cm away from the epiphysis (the direction was perpendicular to the distal phalanx). The FPL was sutured by one thread-end and the EPL was sutured by the other thread-end. In Group B, the broken ends of the FPL and EPL were sutured with 5-0 Prolene in an 8-character-pattern to the ulnar periosteum of the attachments, respectively, which was 0.2 cm away from the epiphysis. Next, a fusiform incision was made on the ulnar of the interphalangeal (IP) joint in the preserved thumb. Then the redundant skin was excised and the joint capsule and collateral ligament of the IP joint were tightened so as to correct the radial deviation of the distal digit. When we treated the bone and joint, the multiple osteotomies of the metacarpal and phalanx were necessary to maintain the alignment. 15
For the Wassel VI to VII type thumb duplication, the radial capsule of the carpometacarpal joint was sutured routinely.
Post-surgery management and follow-up
The thumb was fixed in abduction by a forearm brace. Anti-inflammatories were given and dressing change was performed routinely after surgery. The stitches were removed two weeks postoperatively. Radiographs were taken four weeks after surgery. If the fracture had not healed in four weeks, radiographs were taken again two weeks later. After fracture healing, the Kirschner-wires and brace were removed. Active and passive functional exercises were then performed during the day and the thumb was fixed by a brace at night for one month. Finally, the brace was removed completely and the functional exercises continued for one year.
All the children underwent a six-year follow-up (once a month in the first year and then every six months until the last review). The following indexes were evaluated: parents’ satisfaction with the thumb aesthetics; abduction, flexion and extension function of the thumb; joint stability (lateral stress test); fracture healing; bone development; and anchor absorption on radiograph.
Evaluation methods
The modified Tada evaluation form for thumb duplication 16 was used to evaluate the affected thumb. The thumb was evaluated according to the range of joint movement, joint stability, angular deformity and aesthetics (Table 2).
Modified Tada evaluation form
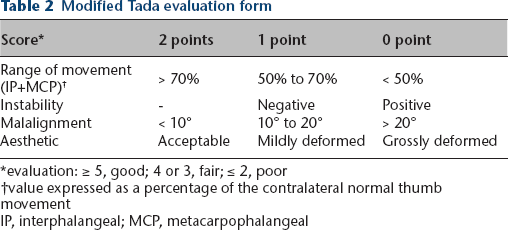
evaluation: ≥ 5, good; 4 or 3, fair; ≤ 2, poor
value expressed as a percentage of the contralateral normal thumb movement
IP, interphalangeal; MCP, metacarpophalangeal
The distance of first web was measured by the Cambridge–Keeling method 17 to evaluate the abduction function of the thumb. This measurement was performed as follows: when the thumb was fully abducent, the distance from the ulnar edge of the IP crease of the thumb to the radial edge of the MCP crease of the index finger was measured.
Statistical analysis
Categorical parameters are expressed as frequency and percentage. Quantitative data are expressed as mean and sd. Statistical analyses of age, healing time of bone, range of movement (IP + MCP), modified Tada score and distance of first web were performed using the two-independent-samples t-test. The threshold for statistical significance was set at p < 0.05. Statistical analyses of the sex, hand side, classification, rate of deformity of the preserved thumbs and rate of a positive lateral stress test were performed using the chi-squared test. The threshold for statistical significance was set at p < 0.05. Statistical analyses were performed with IBM SPSS 21.0 software (IBM Corp., Armonk, New York).
Results
Post-surgery incision and bone recovery
All incisions in this study underwent primary healing. The phalanx and metacarpal reached clinical healing in 5.06 weeks (sd 0.56) (4 to 6 weeks). No anchor shadow or epiphyseal injury was seen on radiographs and the bones developed normally (Figs 7 and 8).

Radiograph six years after surgery (positive).

Radiograph six years after surgery (lateral).
Recovery of thumb appearance
Soft and lightly coloured linear scars were present with no eminence. The skin flap at the incision was slightly bloated in two thumbs. The circumference of the preserved thumb was about 0.36 cm (sd 0.08) (0.3 to 0.5 cm). smaller than that of the contralateral normal thumb. The appearance of the thumbs was satisfactory according to parents in 28 digits. Appearance was slightly bloated in two thumbs, however, it was judged acceptable. The parents considered that eight thumbs had a deviation deformity that affected the function and required a secondary surgery (Figs 9 to 11).
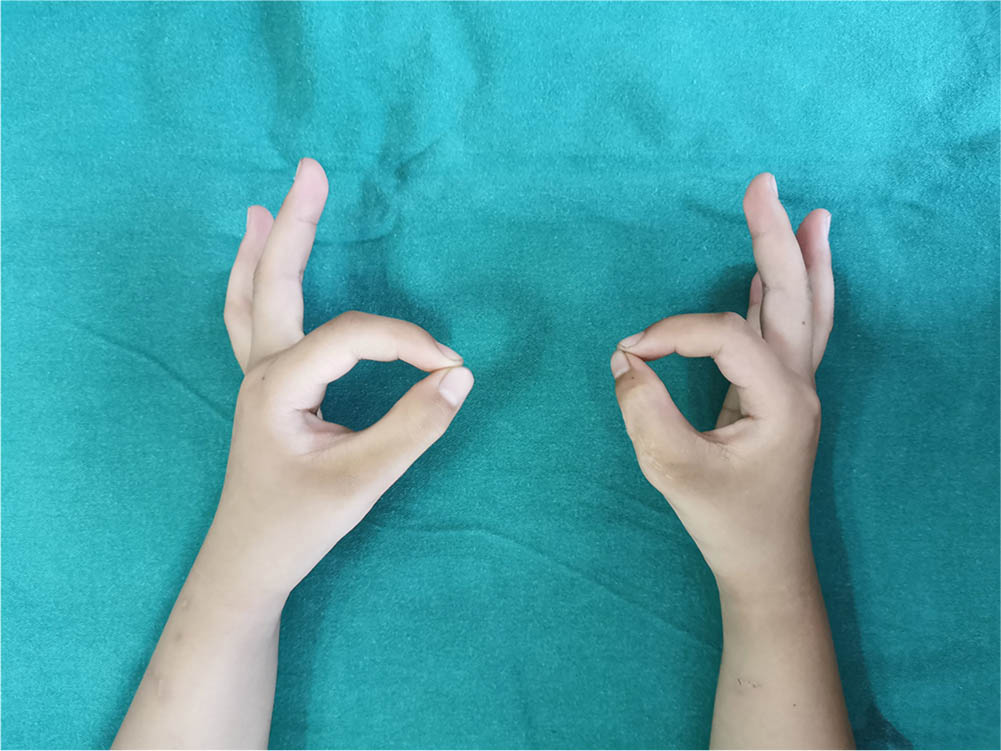
Function of the thumb six years after surgery one.
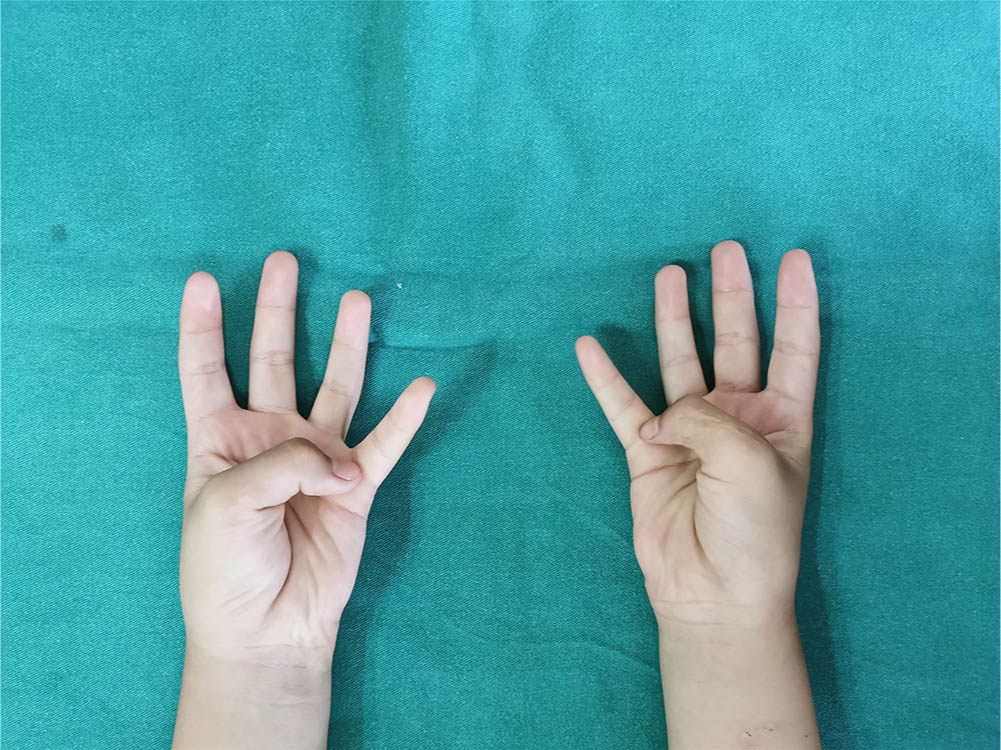
Function of the thumb six years after surgery two.
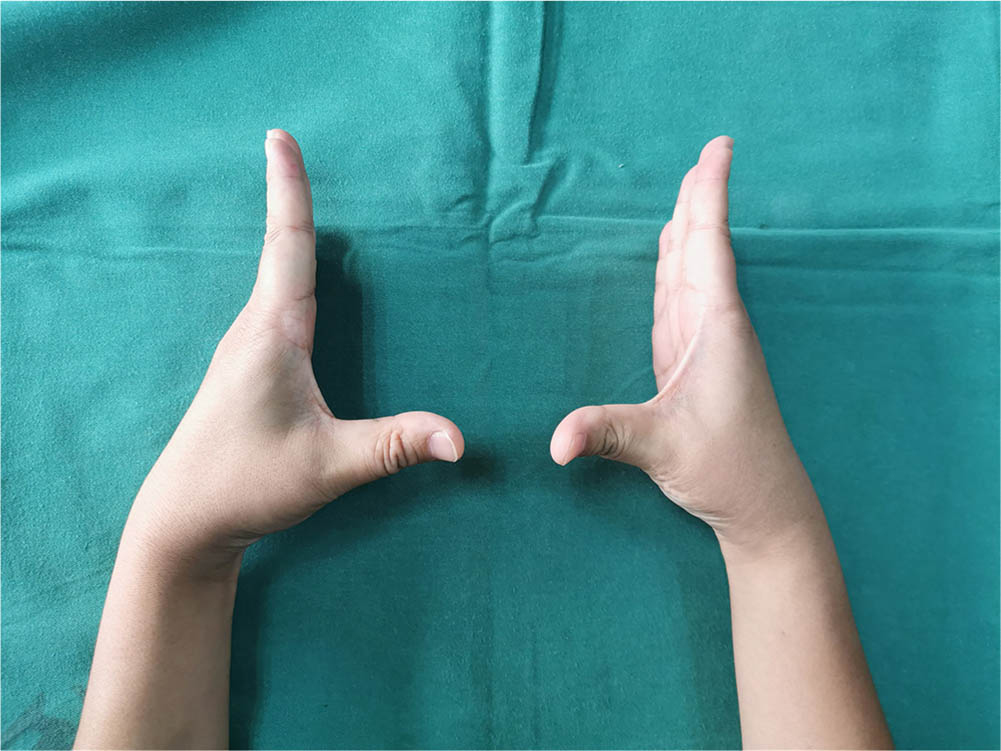
Function of the thumb six years after surgery three.
Post-surgery functional recovery
The mean range of flexion and extension of the (IP + MCP) joint in Group A and Group B was 164.84° (sd 63.80) and 162.84° (sd 63.80), respectively. No significant difference was detected between the two groups (t = 1.62; p = 0.11 > 0.05), but the value was slightly higher in Group A than Group B. Based on this data, the ranges of flexion and extension of the preserved thumbs after the modified surgery cannot be considered significantly better than those after traditional surgery (Table 3).
Evaluation indexes post-operation between two groups

A positive lateral stress test of the MCP joint occurred in two thumbs in Group A and eight thumbs in Group B. This difference between the two groups was statistically significant (chi-squared = 4.89; p = 0.03 < 0.05), and the value was significantly lower in Group A than Group B. This data indicates that the rate of a positive lateral stress test of the MCP joint of the preserved thumbs is significantly lower after the modified surgery than the traditional surgery (Table 3).
Deformity of the preserved thumbs occurred in one case in Group A and seven cases in Group B. All the deformities were in an ulnar deviation of the MCP joint and a radialis deviation of the IP joint. There was a significant difference between the two groups(chi-squared = 5.70; p = 0.02 < 0.05), and the value was significantly lower in Group A than Group B. That is to say, the rate of deformity of the preserved thumbs is significantly lower after the modified surgery than traditional surgery (Table 3).
The mean modified Tada scores of the preserved thumbs in Group A and Group B were 6.79 (sd 0.42) and 5.47 (sd 2.04), respectively. A significant difference was present between the two groups (t = 2.76; p = 0.01 < 0.05). The data showed that the modified Tada scores were significantly different between the two groups, and the value was significantly higher in Group A than Group B. That is to say, the modified Tada scores of the preserved digit are significantly higher after the modified surgery than the traditional surgery (Table 3).
The mean distance of first web in Group A and Group B was 2.44 cm (sd 0.11) and 2.31 cm (sd 0.08), respectively. A significant difference was present between the two groups (t = 4.37; p = 0.00 < 0.05), The data showed there was a significant difference in the distance of first web between the two groups, and the value was significantly higher in Group A than in Group B. That is to say, the abduction function of the preserved thumb was significantly better after the modified surgery than the traditional surgery (Table 3).
Discussion
We retrospectively reviewed 33 children (38 thumbs) with Wassel type III to VII thumb duplication who underwent modified surgery and traditional surgery. The positive results obtained from the cases revealed a lower rate of deformity and better abduction function in the preserved thumbs after the modified surgery. We also suggest the surgery time, indications and announcements for the modified surgery.
Application of anchor technology
For Wassel type III to VII thumb duplication, not only should the polydactylism be excised but an osteotomy should also be performed to restore the alignment.18–21 Additionally, the joint capsule, collateral ligament, APB and FPB should be reconstructed to the attachment in order to restore the joint stability and abduction function of the thumb.18,22–23 In traditional surgery, the broken ends mentioned above were usually sutured to the aponeurosis around the attachment or the periosteum at the attachment position when the joint capsule, collateral ligament, APB and FPB were reconstructed. However, this could not achieve a strong fixation between the tendon and bone. The soft tissues would easily become imbalanced, eventually leading to thumb deviation and poor abduction function. Therefore, we performed the osteotomy at the metacarpal or phalanx according to the angle of thumb deviation and the anchor technique was used to reconstruct the attachment of the joint capsule, ligament and tendon in order to restore the normal anatomical position of the attachment and achieve a better fixation between the tendon and bone.
In this study, we found that after repair by the anchor technique, the modified Tada score, thumb abduction function and MCP joint stability were significantly better than traditional surgery. The incidence of thumb deformity was significantly lower than traditional surgery. This could be explained by the firm fixation of the anchor technique. The screw of the anchor had a strong holding force when it was drilled into the bone cortex. The suture was a high-strength polyester thread, which could restore and increase the strength of the ligament and tendon. The suture could replace the ligament and tendon to bear tension in the early stage. In addition, the fixation of the anchor was beneficial to ensure a tight connection between the joint capsule, ligament, tendon and bone, which conformed to the biomechanical requirements. Anchor fixation thus allowed the joint capsule, ligament and tendon to more easily achieve balance and increased the lateral stability of the joint. Finally, the anchor could shorten the time of external fixation after surgery and allow the children to perform functional exercises at an early stage. The anchor is 1.6 mm in diameter, which matches the size of the metacarpal and phalanx of the thumb, so it does not readily and accidentally injure the epiphysis or other tissues. The absorbable anchor in this study had good compatibility with the bone and no rejection in the children, reducing injury of the epiphysis. However, there was no significant difference in the ranges of thumb flexion and extension compared with traditional surgery. This was related to application of the anchor technique to reconstruct the abduction function of the thumb and had little effect on flexion and extension function.
Surgery time
Many factors influence the choice of surgical timing for thumb duplication, such as the bone development of the children, the complexity of the deformity and the surgeon's proficiency and experience. The optimal surgery time is still controversial. Cabrera González et al 7 investigated 99 children who had undergone surgical treatment of thumb duplication and found that there were few complications if the surgery had been performed before one year of age. Considering the high technical skill required if the surgery was performed before the child was six months old, they recommended that an appropriate surgery time was seven to 12 months of age. However, Hassan et al 24 and Engelhardt et al 25 reported that in some children with complex thumb duplication, the articular structure was not clear on the radiograph before one year and the osteotomy and reconstruction of the articular surface, tendon and ligament was often required during surgery. They suggested the first surgery should be performed older than one year. We consider that the development of tissues is not mature at too early an age. If the surgery is performed too early, it is difficult to distinguish the abnormal tissues structure and physiological function, making the reconstruction difficult to be complete. In addition, it is difficult for a child to cooperate with functional exercises after surgery at an early age. Adversely, if the surgery is performed too late, the development and function of the thumb would be abnormal. This may not only cause many inconveniences in daily life but also place great psychological pressure on children and their families. Therefore, we suggest that 1.5 to 3.0 years old is an appropriate time for surgery. The soft tissues gradually mature and can be clearly identified at these ages. More importantly, the size of the anchor matches the metacarpal and phalanx of children at these ages, which results in minimal bone destruction and epiphyseal injury. At this age the children can be more easily encouraged to cooperate with the postoperative functional exercises.
Notes on the anchor technology
Bilateral hand radiograph examination can be performed to determine the level and angle of osteotomy, which is the most important in all preoperative examinations. B-ultrasound examination has a certain diagnostic basis for understanding the dynamic system of the tendons in children with thumb duplication. 26 This imaging technique can help to judge the route of the tendons and reconstruct the tendons during the surgery.
The thumb should be in the maximum abduction position when the tension of the joint capsule, ligament and tendon are adjusted by the anchor. The anchor is fixed in the radial centre about 0.2 cm away from the epiphysis of the proximal phalanx basement. The direction is perpendicular to the phalanx.
The epiphysis can be clearly visualized during surgery and attention should be paid to avoid epiphyseal injury when implanting the anchor.
After anchor fixation and suturing, the broken ends of the tendon and ligament can be strengthened and sutured to the soft tissues at the attachment with 5-0 Prolene to increase the security of the fixation.
Indications
For thumb duplication in children undergoing surgical treatment, it is usually required to reconstruct the thumb abduction function. If there are no primary diseases that cannot tolerate the surgery, all thumb duplications of Wassel type III to VII in children between 1.5 to 3.0 years should be operated on using the traditional or modified surgery.
Limitations
During the analysis of our results, we identified some limitations of this study. We conducted a retrospective evaluation of surgically treated patients only. We neglected the measurement of strength in the preserved thumb such as the force of grip and pinch, and this index could reflect the strength of the reconstructed ligament and tendon. The cases in the study were relatively small and the follow-up time was relatively short. These limitations will be improved in our future research.
In conclusion, thumb alignment is corrected by osteotomy when surgically treating thumb duplication in children. The thumb abduction function can be well reconstructed when the tension of the joint capsule, ligament, APB and FPB are effectively adjusted by the anchor technique and the soft tissues mentioned above are firmly fixed.
Footnotes
Acknowledgements
We would like to thank Jingjing Zhang for her assistance and guidance in this research.
XZ: Researched literature and conceived the study, Reviewed and edited the manuscript, Approved the final version of the manuscript.
XY: Involved in protocol development, gaining ethical approval, patient recruitment and data analysis, Reviewed and edited the manuscript, Approved the final version of the manuscript.
YB: Involved in protocol development, gaining ethical approval, patient recruitment and data analysis, Reviewed and edited the manuscript, Approved the final version of the manuscript.
HC: Involved in protocol development, gaining ethical approval, patient recruitment and data analysis, Reviewed and edited the manuscript, Approved the final version of the manuscript.
JL: Involved in protocol development, gaining ethical approval, patient recruitment and data analysis, Reviewed and edited the manuscript, Approved the final version of the manuscript.
HL: Involved in protocol development, gaining ethical approval, patient recruitment and data analysis, Reviewed and edited the manuscript, Approved the final version of the manuscript.
YY: Researched literature and conceived the study, Reviewed and edited the manuscript, Approved the final version of the manuscript.