
Abstract
Objective
To evaluate the clinical and functional results of the surgical treatment of bifid thumb type IV in children.
Materials and methods
A retrospective study was undertaken from January 1995 to December 2006. Clinical and radiographic evaluations were made according to Wassel's classification. The patients were performed by transferring an epiphyseal segment of the proximal phalanx with insertion of the abductor pollicis brevis tendon into the radial side of the epiphyseal proximal phalanx of the ulnar thumb. All patients were operated using one of five surgical procedures for bicephalous metacarpus, cartilaginous connection between the radial and ulnar proximal phalanges, the angular deformity of the metacarpophalangeal joint (MPJ) is >20°, and zigzag deformities. The postoperative results of the patients were evaluated for both function and cosmesis according to Tien's modified Tada scoring system.
Results
One hundred and sixty-four patients (102 females, 62 males) were included in this study. The MPJ was stable in 170 thumbs, 15 thumbs had 10° of radial instability, and new collateral ligaments were augmented in 27 thumbs. The alignment was normal in 75 thumbs, with alignment of the interphalangeal joint (IPJ) in 101 thumbs and alignment of the MPJ in 75 thumbs. Postoperatively, there were zigzag deformities in four thumbs (developed zigzag in two thumbs, recurrent zigzag in two thumbs); there was no first web space in those hands. There were four of 185 thumbs with thumb stiffness. The abductor function of 185 thumbs was as follows: >70° in 158 thumbs (85.4%), 50°–70° in 21 thumbs (11.4%), and <50° in six thumbs (3.2%). At the latest follow-up evaluation, no evidence of physeal growth injury or growth arrest was observed in any patient. Overall, we attained good results in 140 thumbs (75.7%), fair results in 36 thumbs (19.4%), and poor results in nine thumbs (4.9%).
Conclusion
We recommend the use of an epiphyseal segment of the proximal phalanx with insertion of the abductor pollicis brevis tendon into the radial side of the epiphyseal proximal phalanx of the ulnar thumb and to restore anatomical insertion of the abductor pollicis brevis muscle. The technique is simple, safe, and effective for thumb abductor function in the treatment of bifid thumb type IV in children.
Introduction
Duplication of the thumb is the most common anomaly of the hand [1–3]. The appearance of the duplicated thumb depends on the changes in the skeletal and soft-tissue structures, which vary with the level of the bifurcation and the extent of the duplication. A precise understanding of the anatomical abnormalities is a prerequisite for successful reconstruction of the thumb in such hands.
Thumb duplication is usually unilateral and sporadic, and with a higher occurrence in Asian populations [4–11]. In China, thumb polydactyly is the most common congenital hand anomaly. Duplication at the metacarpophalangeal joint (MPJ) level (Wassel type IV) is the most common type of duplicated thumbs [3, 5, 9, 10, 12–16].
In the treatment of thumb polydactyly, the simple ablation of one digit has not produced satisfactory results, and doing so frequently results in retained deviation or ligamentous instability of the remaining thumb [9, 12, 13, 17, 18]. Moreover, the reconstructed thumb often later develops complications of physeal growth disturbance and joint stiffness. Therefore, modern reconstructive strategies involving the combining of elements from both thumbs are indicated to achieve a functionally and cosmetically desirable result.
This article describes the results of a series of reconstructive operations done to correct bifid thumbs in children, using the procedure of transferring the epiphyseal segment of the proximal phalanx with insertion of the abductor pollicis brevis tendon for duplication at the MPJ level (Wassel type IV) between 1995 and 2006.
Materials and methods
A retrospective study was undertaken to evaluate the results of a specific surgical technique: transferring the epiphyseal segment of the proximal radial phalanx with insertion of the abductor pollicis brevis tendon. From January 1995 to December 2006, this operation was performed on 173 patients (195 hands) with pre-axial duplication; the Wassel type IV thumb was the most frequent type. Nine patients (10 hands) were excluded from the study because they were lost to follow-up. The remaining 164 patients (185 hands) formed the basis of this study. The main outcome measures were: success of the operation, in terms of function and cosmesis, parental satisfaction with the outcome, and children satisfaction with the outcome.
The 164 patients included 62 boys and 102 girls. The mean age at the time of the surgery was 12 months (range, 6 months to 3 years, 7 months). All patients had a type IV bifid thumb deformity. The duplication was bilateral in 21 patients, on the right side in 86 patients, and on the left side in 57 patients. In 16 patients (9.8%), there was a family history of these same anomalies: two in twins, seven in brothers and sisters, four in parents, and three in other family members.
All surgical procedures were performed by one surgeon (the author of this paper). In the type IV thumbs (bifurcation at the MPJ), the most common deformity, five surgical procedures were used according to the extent of duplication. These are described in detail below. The surgical procedures that were done most frequently (for all patients) included resection of the supernumerary thumb and transferring the radial epiphyseal segment, with insertion of the abductor pollicis brevis tendon into the radial side of the epiphyseal ulnar thumb, after which a collateral ligament was reattached (see Figs. 1a–c, 2, and 3).
We operated on 347 bifid thumbs (bilateral deformity was present in 42 patients): type I, 15 thumbs (4.3%); type II, 45 thumbs (13%); type III, 23 thumbs (6.6%); type IV, 195 thumbs, (56%); type V, 39 thumbs (11%); type VI, nine thumbs (2.6%); and type VII, 21 thumbs (6.1%). In this study, we evaluated the clinical and functional results of the surgical treatment of bifid thumbs, specifically type IV in children only.
The Wassel classification is the most commonly employed classification [4–6, 8, 13, 14, 19–27]. Depending on the level of duplication and bony architecture, seven types are distinguished: (1) bifid distal phalanx, (2) duplicated distal phalanx, (3) bifid proximal phalanx, (4) duplicated proximal phalanx, (5) bifid metacarpal, (6) duplicated metacarpal, and (7) duplicated metacarpal associated with a triphalangeal thumb.
The joint was assessed as being unstable if there was >10° of varus or valgus angulation with stress. Bone healing and any growth-plate changes were evaluated radiographically. We measured the length and the circumference of the thumb. We measured the grip strength and two-point pinch. We also measured the active and passive mobility of the MPJs and interphalangeal joints (IPJs), the stability, and the alignment.
The overall satisfaction of the parents was determined by their selection of one of three responses: “satisfied,” “satisfied, but with some reservation,” or “dissatisfied.” The parents were asked whether they would have their child undergo the same operation again. The overall satisfaction of the children was determined by their response to the question: “Is your thumb pretty?” or “Do you like it?” At the final follow-up evaluation, the mean age of the children was 6 years, 3 months (range, 4 years, 7 months to 10 years, 4 months).
Surgical procedure
After the administration of general anesthesia, the patient was placed supine on the operating table. The upper extremity was prepared with standard antiseptic solutions and draped. The other hand needed to be readily available for comparison when necessary during the operation. We used loupe magnification, and placed a pneumatic tourniquet around the arm. We had a surgical microscope available in case it became necessary to separate the digital nerves of the two thumbs. We planned incisions to avoid a longitudinal incision along the radial border of the reconstructed thumb. A racket-shaped incision was made around the base of the radial duplicated thumb, and the surgeons explored the thumbs for tendon abnormalities. We detached the extensor tendon from the smaller thumb. For the Wassel type IV thumb, the incision had to allow careful exposure of the extensor and flexor surfaces, so that the tendon bifurcations and digital neurovascular structures could be well visualized. Exposure usually entailed a racquet-shaped incision of some type with extension proximally and distally.
Variant 1 (V1)
The racquet-shaped incision was made over the most hypoplastic thumb (usually the most radial digit). Through the incision, we exposed the abductor pollicis brevis tendon as it was inserted into the proximal phalanx of the most radial thumb, and carefully preserved this tendon. If the radial thumb was to be excised, then we identified the adductor pollicis; cut off and carefully preserved an epiphyseal segment, with insertion of the abduction pollicis brevis; and excised an epiphyseal segment of the radial side of the ulnar thumb (Fig. 1a, b). The radial thumb was then shelled out of the wound. We detached the collateral ligament distally from the phalanx that was to be excised (Figs. 1a and 2). We stripped the collateral ligament proximally to the metacarpal or phalanx, using a strip of periosteum to allow adequate exposure of the joint. We then reattached the epiphyseal segment, with insertion of the abduction pollicis brevis tendon attached to the radial side of the epiphyseal ulnar thumb by Dexon 4-0 suturing (Figs. 1c and 3). We centralized the remaining digit over the remaining articular surface, and sutured the collateral ligament and intrinsic tendon securely to the phalanx. We checked the alignment of the extensor and flexor tendons to ensure that they tracked centrally along the digit. Partial resection or transfer of the tendons was sometimes required to achieve a central line of pull. We closed the skin with simple interrupted sutures.
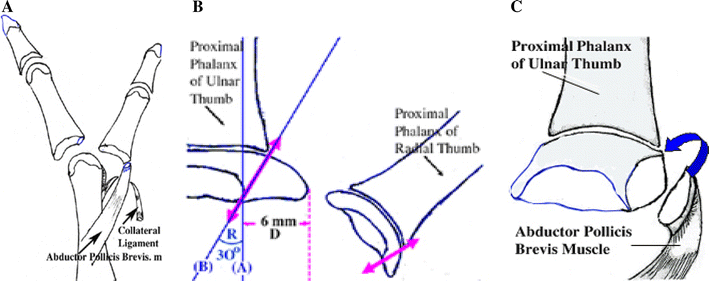
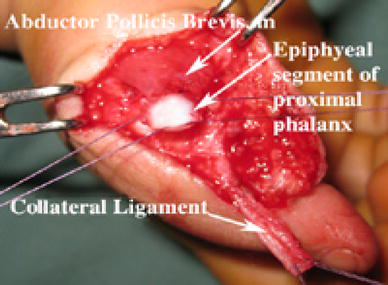
Creating the epiphyseal segment of the proximal phalanx and the collateral ligament
Attach the radial epiphyseal segment with insertion of the abductor pollicis brevis muscle and the radial side of the ulnar epiphysis
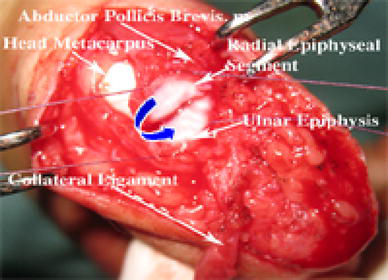
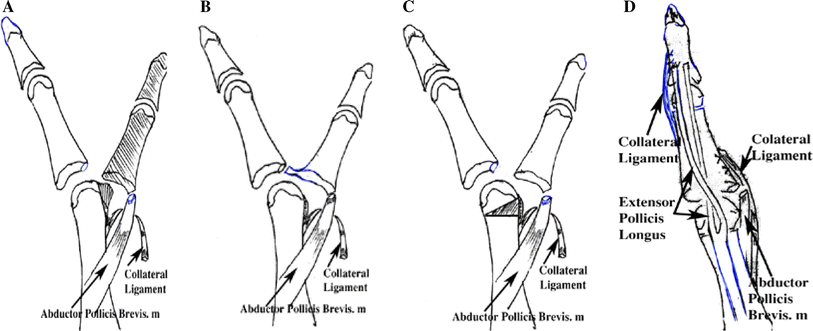
Variant 2 (V2): The metacarpal and its two facets
Using the surgical procedure outlined in V1, the radial thumb was then shelled out of the wound and the metacarpal head needed to be identified. The metacarpal head usually has two facets, one for the excised thumb and one for the remaining thumb. Using a #15 blade as an osteotome, the surgeon removed the radial facet with a triangular portion of the radial shaft. In older children, with more ossification of the metacarpal, a rongeur or bone biter was sometimes required (Fig. 4a); the bone was shaved down to correct the malalignment and to produce congruent joint surfaces. Then, we sutured the epiphyseal segment with insertion of the abduction pollicis brevis tendon attached into the radial side of the epiphyseal ulnar thumb, and reattached the collateral ligament.
Surgical procedures:
Variant 3 (V3): Cartilaginous connection between the radial and ulnar proximal phalanges
Using the surgical procedure outlined in V1, the cartilaginous connection between the radial and ulnar proximal phalanges was identified and we then separated the connected cartilage (Fig. 4b). Care was taken not to excise too much cartilage, in order to avoid postoperative malalignment of the MPJ, due to incongruency of the joint surfaces. Then, we sutured the epiphyseal segment with insertion of the abduction pollicis brevis tendon attached to the radial side of epiphyseal ulnar thumb, and reattached the collateral ligament.
Variant 4 (V4)
This procedure was performed in cases in which the angular deformity of the MPJ was >20°. Performing a corrective closing-wedge osteotomy at the metacarpal neck was required (Fig. 4c). The epiphysis was usually not included in the wedge, for fear of growth-plate injury. The additional Kirschner wire crossed the metacarpal neck to stabilize it. Then, we sutured the epiphyseal segment with insertion of the abduction pollicis brevis tendon attached to the radial side of the epiphyseal ulnar thumb, and reattached the collateral ligament.
Variant 5 (V5): Surgery for zigzag deformity
In these thumbs, where the radial component was removed, there was ulnar deviation at the MPJ and radial deviation at the IPJ. The aim of the reconstructive surgery was to provide good alignment and stable joints. We performed a closing-wedge osteotomy of the metacarpus and proximal phalanx to correct malalignment. The additional Kirschner wire was then inserted from the tip of the thumb across the IPJ and MPJ into the metacarpus to stabilize it. The Kirschner wire was left outside the skin for easy removal later (Fig. 5). The extensor pollicis longus tendon was reinserted toward the ulnar side of the distal phalanx (Fig. 4d). The surgeon then performed simple capsulorrhaphy of the ulnar side of the IPJ, including tightening of the ulnar collateral ligament. Then, we sutured the epiphyseal segment with insertion of the abduction pollicis brevis tendon attached to the radial side of the epiphyseal ulnar thumb, and reattached the collateral ligament.

Closing-wedge osteotomy and fixed Kirschner wire
Aftercare
Depending on the age of the patient, a short- or long-arm thumb spica cast was applied (Fig. 6). Younger children (under 3 years of age) required a long-arm cast. We removed the cast 4–6 weeks postoperatively, and checked the radiographs. We removed buttons and pullout sutures, and removed Kirschner wires after checking for bony union on the radiographs (usually 6–8 weeks). During therapy and gentle activities, the children were allowed to use the thumb freely. In cases in which the IPJ or MPJ radial collateral ligament had been reconstructed, we provided a custom-made splint for the child to wear at night until 3 months after surgery.

Hand spica cast
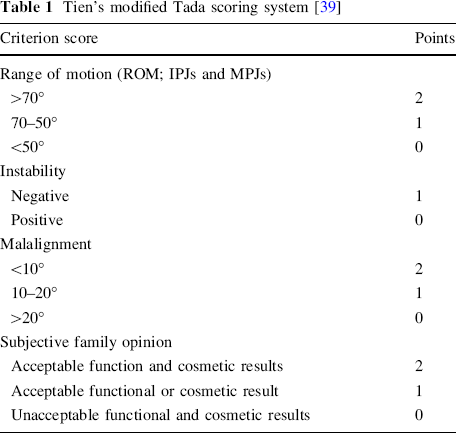
We used Tien's modified Tada scoring system to evaluate both function and cosmesis (Table 1). The patients’ parents were asked to score the functional and the aesthetic results. An overall score of 6 points or more was rated as a good result; 3–5 points, fair; 2 points or less, poor.
Tien's modified Tada scoring system [39]
Results
The results after each of these five procedures varied, as shown in Table 1. We discuss the results for the varying procedures below.
Variant 1 (V1)
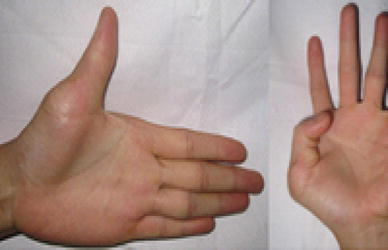
There were 117 thumbs operated on with V1. In seven of these 117 cases, we created a new collateral ligament, and this composite was reattached to restore joint stability. The thumb abductor function was >70° in 102 thumbs and 50°–70° in 15 thumbs (Fig. 7). Adequate skeletal correction and stability was achieved, with no disturbance of growth noted, and function was satisfactory.

Postoperatively, functional abductor and adductor thumb
Both parents and patients rated the surgery as having acceptable functional and cosmetic results in 109 thumbs, acceptable functional or acceptable cosmetic result (but not both) in four thumbs, and unacceptable functional and cosmetic results in four thumbs.
Variant 2 (V2)
There were 29 thumbs operated on with V2; children who had arthroplasty of the MPJ (shaving of the head of the metacarpus) which caused bicephalous metacarpus (Fig. 8). In four of 29 thumbs, we created a new collateral ligament. The thumb abductor function was >70° in 25 thumbs, 50°–70° in two thumbs, and <50° in two thumbs. After follow-up ranging from 4 to 9 years (on average, 6 years, 5 months), 15 of 29 thumbs were rated as good, and none of the 29 thumbs showed evidence of disturbed growth of the shaved metacarpus. Enlargement of the metacarpal head was seen on the roentgenograms of two hands (two patients). In the remaining 27 thumbs (93.1% of 23 patients), all of which were reconstructed in patients less than 3 years old, cartilaginous enlargement was identified during the reconstruction. There was one thumb that developed a zigzag deformity, and one thumb that developed joint stiffness. Both parents and patients rated the result as having acceptable function and cosmesis in 15 thumbs, acceptable functional or cosmetic result in 12 thumbs, and unacceptable functional and cosmetic results in two thumbs.
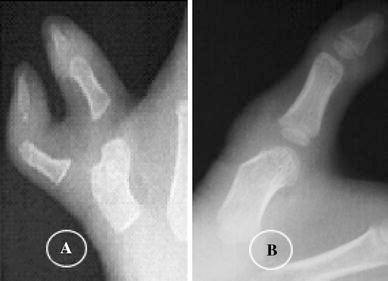
X-ray:
Variant 3 (V3)
There were 13 thumbs operated on with procedure V3; children who had a cartilaginous connection between the radial and ulnar proximal phalanges. In three thumbs, we created a new collateral ligament. At the latest follow-up, the thumb abductor functions were >70° in 12 thumbs and 50°–70° in one thumb. Both parents and patients rated the results as having acceptable function and cosmesis in six thumbs, and acceptable functional or cosmetic result in seven thumbs.
Variant 4 (V4)
There were 11 thumbs operated on with V4; children who had a closing-wedge osteotomy of the metacarpal head; all thumbs were divided >20° at the MPJ. In five thumbs, we created a new collateral ligament. At the latest follow-up, adequate skeletal correction and stability had been achieved, no disturbance of growth had been noted, and the thumb abductor function was >70° in eight thumbs, 50°–70° in one thumb, and <50° in two thumbs. There was one thumb that had developed a zigzag deformity, and one that had joint stiffness. Both parents and patients rated the results as having acceptable function and cosmesis in seven thumbs, acceptable functional or cosmetic result in three thumbs, and unacceptable functional and cosmetic results in one thumb.
Variant 5 (V5)
There were 15 thumbs operated on with V5; children in which the radial thumb was resected and who had MPJ deformities. The MPJ deformity in all patients was >20° [average 24.6° (range 21.2–30.0)] and the proximal phalanx joint was >20° in all patients [average 22.9° (range 22.2–28.5)]. A closing-wedge osteotomy of the proximal phalanx and the metacarpus was used to correct these deformites (Fig. 5). There were eight thumbs for which the surgeon created a new collateral ligament. At the latest follow-up, the thumb abductor function was >70° in 11 thumbs, 50°–70° in two thumbs, and <50° in two thumbs. There were two thumbs that experienced recurrent zigzag deformity. Three patients lost the power of tip-pinch and had a decreased power of pinch. Frequently, an abnormal pattern of pinch developed, yet, the patient did not complain about a decreased ability to pinch. Both parents and patients rated the results as having acceptable function and cosmesis in nine thumbs, acceptable functional or cosmetic result in four thumbs, and unacceptable functional and cosmetic results in two thumbs. There were two thumbs that had joint stiffness. The time to solid osseous union of the distal phalanx and metacarpal neck osteosynthesis radiographically ranged from 4 to 6 weeks; however, after removal of the Kirschner wire at 4–6 weeks postoperatively, osseus healing was adequate for stability without pain. The radial component and radial long extensor were usually hypoplastic compared with the ulnar component.
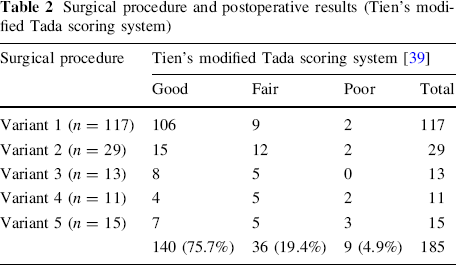
The average follow-up was 4 years and 6 months (range, 3 years, 6 months to 9 years, 10 months). Malalignment of the longitudinal axis of the thumb and lack of motion were the main causes of the 36 fair and nine poor results in these thumbs (Table 2).
Surgical procedure and postoperative results (Tien's modified Tada scoring system)
Remodeling of the distal phalanx occurred with time. At the latest follow-up evaluation, no evidence of physeal injury or growth arrest was observed in any patient (Fig. 9). The average length of the thumb was 3.9 cm on the operated side and 4.1 cm on the normal side. The average circumference was 5.0 cm on the operated side and 4.8 cm on the normal side. At the latest follow-up evaluation, the average grip strength measured 3.2 kg (1.4–6.8 kg) on the operated side (Fig. 10a) and 3.5 kg (1.8–7.4 kg) on the normal side. The two-point pinch strength measured an average of 2.1 kg (range, 1–6.4 kg) on the operated side (Fig. 10b) and an average of 2.5 kg (range, 1–7 kg) on the normal side.

None of the patients showed evidence of disturbed epiphyseal growth with attached insertion of the abductor brevis muscle

Postoperatively, the functional extensor and flexor interphalangeal joint (IPJ) and metacarpophalangeal joint (MPJ)
Postoperatively:
There were 158 of 185 thumbs with the collateral ligament from the deleted component elevated with an osteoperiosteal sleeve and attached via periosteal suture to the ulnar thumb. We augmented a new collateral ligament in the 27 remaining thumbs (V1 in seven thumbs, V2 in four thumbs, V3 in three thumbs, V4 in five thumbs, and V5 in eight thumbs). At the latest follow-up evaluation, the MPJ was stable in 170 thumbs and 15 thumbs (V1, five thumbs; V2, three thumbs; V3, two thumbs; V4, two thumbs; V5, three thumbs) had >10° of radial instability, with an average of 14° and a range of 12°–18°.
Overall, the alignment at the time of follow-up was normal in 75 of 185 thumbs:
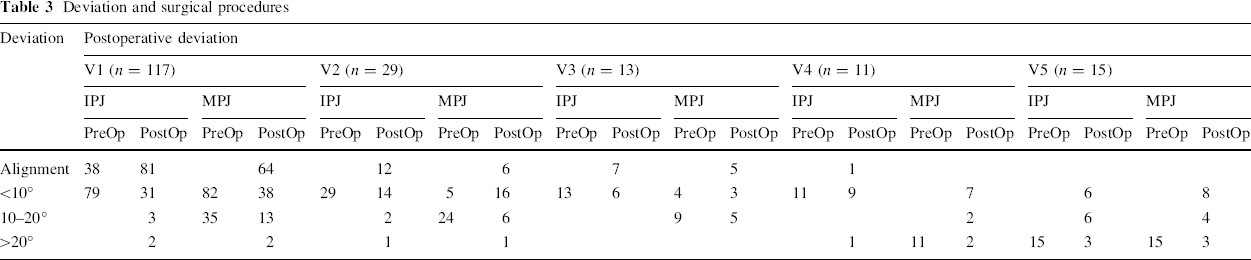
Alignment of the IPJ in 101 thumbs Deviation at the IPJ <10° in 66 thumbs, 10–20° in 11 thumbs, >20° in seven thumbs (V1 in two thumbs, V2 in one thumb, V4 in one thumb, V5 in three thumbs) Alignment of the MPJ in 75 thumbs Deviation at the MPJ <10° in 72 thumbs, 10–20° in 30 thumbs, >20° in eight thumbs (V1 in two thumbs, V2 in one thumb, V4 in two thumbs, V5 in three thumbs)
Postoperatively, there were zigzag deformities in four thumbs (developed zigzag in two thumbs: V2 in one thumb, V4 in one thumb; recurrent zigzag: V5 in two thumbs):
IPJ improvement in preoperative ROM 50°–70° in nine thumbs, <50° in six thumbs Postoperative ROM >70° in two thumbs, 50°–70° in 11 thumbs, and <50° in two thumbs MPJ improvement in preoperative ROM 50°–70° in seven thumbs, <50° in eight thumbs Postoperative ROM >70° in two thumbs, 50°–70° in nine thumbs and <50° in four thumbs
There were four of 185 thumbs (2.2%) with thumb stiffness (V2 in one thumb, V4 in one thumb, and V5 in two thumbs).
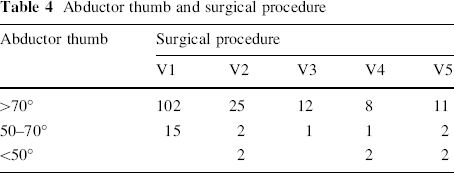
Overall, the abductor function of 185 thumbs was as follows: >70° in 158 thumbs (85.4%) average 72° (range, 71°–76°); 50°–70° in 21 thumbs (11.4%) average 61° (range, 56°–68°); <50° in six thumbs (3.2%) average 38° (range, 32°–45°)]. The abductor functions of thumbs were under 50° with either thumb stiffness or zigzag deformities.
At the latest follow-up, the IPJ had an average active range of motion of 42° (range, 15°–71°), and an average passive range of motion of 68° (range, 39°–74°). On the normal side, the average active and passive range of motion of the IPJ was 72° (range, 62°–80°) (cf. Fig. 11).
The mobility of the MPJ had an average active range of motion of 54° (20°–81°) and a passive range of motion of 74° (39°–84°). On the normal side, the average range of motion of the MPJ was 78° (range, 64°–82°) (cf. Fig. 11).
Deviation and surgical procedures
Abductor thumb and surgical procedure
Range of motion (ROM) and surgical procedures

Subjective family opinion and surgical procedures

The parents who reported unacceptable functional and cosmetic results in nine thumbs are awaiting additional operations for their children.
Complications
All patients had normal sensibility. There was no complications consisting of physeal growth disturbance, hyperplastic scar in 14 thumbs, zigzag deformities in four thumbs (developed zigzag deformity in two thumbs, recurrence of zigzag deformity in two thumbs), and joint stiffness in four thumbs.
Discussion
The timing of the initial surgery
The timing of the initial surgery for the reconstruction of bifid thumb type IV is very important. If it is undertaken too early, the abnormal anatomical findings are difficult to identify, and the reconstructive surgery cannot be accomplished properly, with the result that deformity may develop after the surgery. The timing of the initial surgery should be determined according to the extent of duplication and the experience of the surgeon. Based on the experience in this study, the most suitable time for the initial surgery is about 6 months after birth to 1 year old for type IV. In a survey of the literature, most surgeons who have operated on bifid thumb type IV in children suggested the same timing of the initial surgery [16, 18, 28]. In our own study, 122 of 164 patients (74.4%) were operated on when they were under 12 months of age.
It has generally been accepted that simple resection of a supernumerary thumb frequently leads to a deformity of the remaining thumb [11]. Even after a seemingly adequate initial operation, a deformity may occur with growth. Marks and Bayne reported that six of their 25 patients needed additional procedures, and Tuch et al. reported that only 60% of their 22 patients had a satisfactory result after initial operative treatment for duplication of the thumb. This suggests that it may be difficult to achieve a well-planned reconstruction if duplication of the thumb is treated too early, and a deformity may develop.
Function of the hand, including grip and pinch, develops rapidly during the first 6 months of life and is established, albeit at a primitive level, by the 12th postnatal month. Therefore, from the age of 6 months, we believe that the earlier the hand is reconstructed, the more satisfactory will be the functional result. If the articular cartilage is shaved to establish more congruent joint surfaces in the affected thumb, remodeling of the joint can be expected only in children who are less than 1 year old, as described by Riordan [29] in the reconstruction of the radial ray deficiency. Marks and Bayne considered the preferable age for reconstruction of the thumb to be 3 years, but we prefer 6 months to 1 year, based on the 185 thumbs that we treated initially in this study. James and some authors had proposed the optimal timing of initial surgery to be roughly 6 months of age, when general anesthesia is safe. Surgery performed before the child starts school may reduce teasing by other children and prevent school absences. Parents and the older child should share the surgeon's goals, and understand the risks and likely outcomes of the surgery [30].
Transferring the abductor pollicis brevis muscle and relative factors of thumb abduction
Having a functional abductor pollicis depends on several factors, including power and direction of the abductor pollicis muscle, congruent joint surfaces at the MPJ, and a stable collateral ligament. In our study, the abductor pollicis brevis muscle was always attached to the radial component, regardless of the extent of the duplication, and had to be transferred to the preserved ulnar thumb component. In thumbs with this level of bifurcation, no other intrinsic muscle was attached to the radial thumb component. If only resection of the radial thumb is to be carried out, the remaining thumb will deviate at the MPJ toward the ulnar side because of the lack of abduction force.
As many authors have mentioned, it is not the simple presence of excess tissue, but, rather, the anatomical abnormality, malalignment, and hypoplasia that cause problems [9, 11, 13, 31–34]. The range of motion is restricted by hypoplasia or deformity of the joint, hypoplasia or abnormal insertion of a tendon, and/or scarring. Instability is caused by hyperlaxity or hypoplasia of supportive tissues of the joint, and by abnormal insertion of a tendon. Angulation is the result of an incorrect axis of a bone, an excessively large cartilaginous head, imbalance and abnormal insertion of a tendon, an interposed delta phalanx, and/or scarring [25].
In the thumbs that had been treated by simple resection of the supernumerary digit at the level of the MPJ, the procedure was commonly complicated by deviation of the digit at the MPJ, while the alignment and stability of the IPJ were maintained satisfactorily [30] (see Table 3). In these thumbs, abduction was deficient due to the lack of function of the abductor pollicis brevis muscle. Radial angulation of the IPJ and ulnar angulation of the MPJ developed after the radial thumb had been resected. The imbalance of the power of the tendons caused both the secondary deformity at the MPJ and also a narrowing of the first web space [9, 25].
Abductor pollicis brevis is a thin, subcutaneous muscle in the proximolateral part of the thenar eminence. It arises mainly from flexor retinaculum: a few fibers spring from the tubercles of the scaphoid bone and trapezium, and from the tendon of the abductor pollicis longus. Its medial fibers are attached by a thin, flat tendon to the radial side of the base of the proximal phalanx of the thumb [23]. We transferred the radial epiphyseal segment with insertion of the abductor pollicis brevis tendon attached to the radial side of the ulnar epiphysis to restore power and direction of the abductor pollicis muscle (see Table 4).
We used Dexon suture attachment of the segment of epiphyseal radial thumb with insertion of the abductor brevis tendon, which was sutured into the epiphyseal ulnar thumb. Postoperatively, the thumb was immobilized by a hand spica cast. We removed the cast at 4–6 weeks, and provided a custom-made splint for the child to wear at night until 3 months after surgery. At the latest follow-up, there was no evidence of disturbed growth of the metacarpal or distance between the epiphyseal ulnar thumb and the segment of epiphyseal radial thumb with insertion of the abductor brevis tendon.
However, we agree that should suture attachment of the abductor pollicis brevis directly onto the epiphysis of the proximal phalanx by nonabsorbable sutures (Silk, Ethibond) to protect the segment of the epiphyseal radial thumb with insertion of the abductor pollicis brevis tendon and length of time quite possibly limited the rotation of that epiphyseal fragment.
The first web space might have been a secondary change after insufficient active abduction, but there was no relationship between the extent of abduction and the age of the patient. In this study, functional abductor thumbs were normal (>70°) in 158 thumbs (85.4%) and 50°–70° in 21 thumbs (11.4%), so we did not identify this complication.
The objective of the surgical procedure that we performed was to gain good alignment of the MPJ. The enlargement of the metacarpal head was seen on the roentgenograms of two patients who were more than 3 years old (see Fig. 5). In 27 of 29 remaining thumbs [93.1% (23 patients)], all of whom were less than 3 years old, cartilaginous enlargement was identified during the reconstruction. So, we decided to expose the MPJ to examine the head of the metacarpus in all patients. If the metacarpal had a dicephalous head, this was shaved down to correct the malalignment and to produce congruent joint surfaces, and the capsule of the MPJ was reconstructed. After follow-up ranging from 4 to 9 years (average, 5 years, 8 months), 15 of the 29 (51.7%) remaining thumbs were rated as good, and none of these 29 thumbs showed evidence of disturbed growth of the shaved metacarpal.
One of the 29 thumbs (3.4%) in V2 and two of the 11 thumbs (18.2%) in V4 had radial deviation at MPJ >20°, perhaps because we had shaved down too much cartilage to produce incongruent joint surfaces at the MPJ, and when the collateral ligament was reattached, distal insertion of the collateral ligament was unstable. Care was also taken not to excise too much cartilage when there was a cartilaginous connection between the radial and ulnar proximal phalanges, in order to avoid postoperative malalignment of the MPJ due to incongruency of the joint surfaces.
There were 158 of 185 thumbs with the collateral ligament from the deleted component elevated with an osteoperiosteal sleeve and attached via periosteal suture to the ulnar thumb (see Fig. 2). In the 27 remaining thumbs, we created a new ligament by using part of the ablated tendon. Care had to be taken to preserve a slip of the subperiosteal tissue for reattachment, together with the distal insertion of the collateral ligament. These recurrences of thumb malalignment were mainly caused by a persistent imbalance of the intrinsic and extrinsic muscle forces. In these hands, tendon reinsertion and arthroplasty were more effective than osteotomy in producing good alignment and stability of the affected thumb [25]. In our study, at the latest follow-up evaluation, the MPJ was stable in 170 thumbs (91.9%) and 15 thumbs had >10° of radial instability (average 14°, range 12°–18°).
Zigzag deformity
The zigzag deformities are reported to be more severe and complex [18, 25]. In our study, 15 thumbs were angulated radially at the IPJ and ulnarward at the MPJ. An osteotomy of the proximal phalanx and the metacarpus was used to correct this deformity, and the extensor indicis proprius tendon was transferred to the ulnar side of the base of the distal phalanx, in an attempt to provide dynamic augmentation of the lateral stability of the IPJ. Four patients are awaiting surgery at a later stage. Those patients had an axis deviation of 22°–27°.
The surgical procedure is very complicated in hands with the zigzag deformity; the flexor tendon(s) are treated in a similar fashion [6, 8, 9, 35]. All of the intrinsic and extrinsic muscles that had been inserted on the radial thumb could be transferred to their normal insertions on the preserved ulnar component; however, their exposure and transfer should be limited [33]. But eccentric insertions of the flexor pollicis longus and/or extensor pollicis longus are common in patients in whom the IPJs are angulated preoperatively [12, 28]. Some authors propose that the flexor and extensor tendon insertions should be carefully examined, and tendon realignment should be performed if necessary [6, 14, 35] to provide the balancing of unbalanced tendons [18, 25]. The imbalance of tendons in these thumbs may have caused the angulation deformity.
To avoid the residual angular deformities in the remaining thumb, numerous refinements in the technique exist, such as adequate collateral ligaments reconstruction, flexor and extensor tendons centralization, alignment of the joint surfaces perpendicular to the long axis by osteotomies, and balancing muscle power by tendon transfer [6, 8, 9, 12, 18, 35, 36].
Criteria for postoperative evaluation
Our patients who had residual deformities were much more concerned with appearance than with function. Similarly, Cheng et al. found that, of 95 patients, only one complained about function, but many patients and parents were unhappy with the appearance of the thumb. Kleinert et al. [37] mentioned that one complaint of their patients was the diminished circumference of the thumb. Therefore, treatment must primarily satisfy cosmetic demands, and, from that point of view, the alignment and size of the thumb and the shape of the nail are important [25].
Although an exceedingly small thumb is obviously undesirable from a cosmetic point of view, it is not possible to augment it at the second operation. Postoperatively, in our study, the average length of the thumb was 3.9 cm on the operated side and 4.1 cm on the normal side. The average circumference was 5.0 cm on the operated side and 4.8 cm on the normal side. Some authors [18, 25, 38] had used criteria for postoperative evaluation as initially defined by Tada et al. The results of surgical treatment were rated by a scoring system that we devised to enable us to assign points for the range of motion (see Table 5) and stability of the joint, and the alignment of the affected thumb, as well as to determine an overall score for each thumb. The cosmetic results, based on the size of the preserved thumb and satisfaction of the patient, were very difficult to assess objectively. The results of surgical treatment, therefore, were evaluated only by the objective assessments. The thumbs with active motions of the IPJ and MPJ, stability, and lateral instability were recorded [8, 18].
In our practice, we preferred to use the modified Tada scoring system proposed by Tien et al. combined with subjective family opinion [i.e., the family rated the surgery as having acceptable functional and cosmetic results in 146 thumbs (78.9%); acceptable functional or cosmetic results in 30 thumbs (16.2%); and unacceptable functional and cosmetic results in nine thumbs (4.9%)] (see Table 6). Overall, considering all 185 type IV thumbs that were followed, the results of the modified Tien system combined with subjective family opinion were as follows: 140 (75.7%) good, 36 (19.4%) fair, and nine (4.9%) poor.
Complications
The reconstructed thumb is always shorter than the normal thumb. In addition, angulation, joint instability, limited motion, and scar contracture are common problems [8, 21]. Reoperation rates between 20 and 25% have been reported [17, 33]. More complicated thumb duplications create more postoperative problems. Any offset in bone axis, persistent joint instability, or tendon malalignment will lead to problems. Joint instability and/or imbalanced tendon action will cause thumb deviation and a “Z” deformity over time. The approach to the malaligned thumb is to consider the potential underlying cause(s) [6, 27]. Treatment requires the restoration of parallel joint surfaces, restitution of joint stability, and realignment of tendon(s) [8].
Poor motion and persistent instability are even more difficult to treat. Joint contracture often results after articular modification, followed by subsequent scarring and arthrofibrosis. Limited treatment is available to restore motion in these cases. The thumb with preservation of passive motion without active motion, however, may benefit from tenolysis. Persistent instability combined with limited motion requires ligament reconstruction or arthrodesis. In general, arthrodesis or chondrodesis is preferred to reliably restore stability in cases in which joint enlargement is also a later problem after surgery. This protuberance is usually secondary to the inadequate removal of an intra-articular facet. Arthrotomy and removal will rectify this problem.
Conclusion
The timing of the initial surgery should be 6 months after birth to 1 year of age for type IV bifid thumb reconstruction. Our technique uses an epiphyseal segment of the proximal phalanx with insertion of the abductor pollicis brevis tendon into the radial side of the epiphyseal proximal phalanx of the ulnar thumb, and restores power and direction of the abductor pollicis muscle. The technique is simple, safe, and effective in the treatment of bifid thumb type IV in children.