
Abstract
Abstract
Purpose
Comparison of two hexapod frame systems in paediatric tibial deformity correction; the Taylor Spatial Frame (TSF) and Orthex Hexapod System.
Methods
Paediatric patients with congenital and acquired tibial deformities treated with either TSF (between 2014 and 2016) or Orthex (between 2017 and 2019) frames were included in a retrospective comparative study. Outcome measures were healing index, pin infection rate, regenerate quality and density, software residual rate, deformity correction accuracy, strut exchanges and quality of life (QoL).
Results
The TSF group had 17 patients (18 frames) and the Orthex group had 21 patients (25 frames). The most common indications for tibial deformity correction were fibular hemimelia (14) and septic or traumatic growth arrest (8). The median time in frame was 230 days (TSF) versus 203 days (Orthex) (p= 0.06). The mean lengthening achieved was 54 mm (TSF) and 51 mm (Orthex) (p = 0.41). The healing index was 41 days/cm (TSF) versus 43 days/cm (Orthex) (p = 0.70). Pin site infections occurred more in the TSF cohort (40%) than in the Orthex cohort (18%) (p < 0.001). The regenerate in the Orthex group showed higher density at three months (p = 0.029) and was more homogenous (p = 0.023) at six months after frame application. Strut exchanges were less frequent with the Orthex system (p < 0.0001). QoL measures were similar in both cohorts (p = 0.92).
Conclusions
This is the first study to compare two hexapod designs in paediatric orthopaedics. The Orthex system showed superiority in regenerate quality and a significant reduction in pin site infection rates. Both systems delivered predictable and accurate limb deformity correction.
Level of evidence
III
Keywords
Introduction
The introduction of the Taylor Spatial Frame (TSF; Smith & Nephew, Memphis, Tennessee) in 1995 revolutionized the treatment of limb deformities in paediatric orthopaedics. 1 The possibility to correct deformities in all three planes simultaneously without the need for sequential hinge constructs with the Ilizarov apparatus has proven to be more precise, efficient and user friendly.2–5
The TSF has been successfully used for a wide range of acquired and congenital conditions 5 and acute paediatric fractures. 6 The expiry of its patent has allowed new design and software concepts to enter the market, e.g. TrueLok-Hex (Orthofix, Lewisville, Texas), Orthex (OrthoPediatrics, Warsaw, Indiana), Hoffman-LRF (Stryker, Kalamazoo, Michigan) and Ortho-SUV (OrthoSUV Ltd, St Petersburg, Russia). Only one study has directly compared the Ilizarov frame with TrueLok-Hex 2 and, to our knowledge, no study has directly compared different hexapod systems in the clinical context.
Our single-centre single-surgeon study aims to compare the Orthex Hexapod System with the TSF. We hypothesize that differences in hardware and software design might affect clinical and radiological outcomes in terms of healing index, time in frame, pin site infection rate, regenerate characteristics and quality of life measures post treatment. We also assess the reliability in deformity correction. For patient safety reasons we compared preoperative set-up times, operating times and radiation exposure intraoperatively.
Patients and methods
This study represents a review of prospectively collected data from our institutional database. Ethics approval was obtained from the local institutional review board (H15-00185; H15-03353).
All patients requiring tibial deformity correction between 30 September 2014 and 26 September 2019 were included in the study if a minimum of six months of clinical follow-up was achieved following frame removal. Exclusion criteria were; different frame system (e.g. TrueLok-Hex) or deformity correction in the femur with TSF or monolateral systems.
Eligible participants were recruited from the limb reconstruction outpatient clinic. All clinical and radiographic data collected as part of their routine clinical care was recorded in a REDCap electronic database (Vanderbilt, Nashville, Tennessee) hosted at the senior author's (AC) institution. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies.
Data was collected based on radiographic appearance of regenerate, 7 on regenerate density (pixel value ratio, PVR), 8 pin site status (Checkett's grading) 9 and quality of life measures (PedsQL) 10 after frame removal (minimum six months). An infection episode was defined as a finite period of antibiotic treatment for a pin site infection (Checkett's grade 2 and above) resulting in clinical resolution. All pin sites were topographically labelled and documented with photographs. Mechanical axis deviation, medial proximal tibial angle (MPTA), lateral distal tibial angle, posterior proximal tibial angle (PPTA) and anterior distal tibial angle were collected pre- and post-correction via picture archiving and communication system software (Philips, Amsterdam, Netherlands).
The TSF system consists of aluminium rings connected by single-telescoping struts. The rings were fixed to the tibia with smooth stainless-steel wires (1.8 mm) and partially hydroxyapatite (HA)-coated (thread only) half-pins. Mounting parameters (relation of the proximal reference ring to the point of origin) were measured intraoperatively and then entered into the web-based software application. 11
The Orthex system has aluminium rings connected by double-telescoping struts, fixed to the tibia with extended HA-coated (thread and shank) half-pins and fully HA-coated wires (1.8 mm). Intraoperative radiographs were uploaded onto the web-based software application 12 for semi-automated mounting and deformity analysis.
Structures at risk and patient characteristics determine the rate of correction. The patient and their family are instructed to perform adjustments three times per day. Weekly pin site care is performed in clinic following our institute's protocol. 13
Statistical analysis
This was undertaken using NCSS 2019 (v19.0.1) (NCSS, LLC, Kaysville, Utah). Normally distributed data were analyzed with two-sided t-test (or analysis of variance for multiple group testing), Mann-Whitney-U test for non-parametric ordinal and crosstab tests for categorical data. Multiple regression analysis (Poisson) was performed with pin infection rate as the non-continuous responder variable. Age, time in frame, length of regenerate, number of rings, half-pins and wires, presence of foot ring and extended HA coating were included as potential predictor variables. Results were considered significant if p < 0.05.
Results
Demographics
The inclusion criteria were met by 38 patients treated at our institution from 2014 until 2019 (Table 1). A total of 17 patients (18 frames) were included in the TSF group. The mean age in this group was 12 years (5 to 18). The sex distribution was 14 boys and three girls. The mean weight was 51 kg (37 to 82). A total of 21 patients (25 frames) were treated with the Orthex system. The mean age in this group was 13 years (3 to 20). The mean weight was 53 kg (23 to 90). The sexes were more equally distributed with 11 boys and ten girls.
Patient demographics, indications and details of hexapod constructs
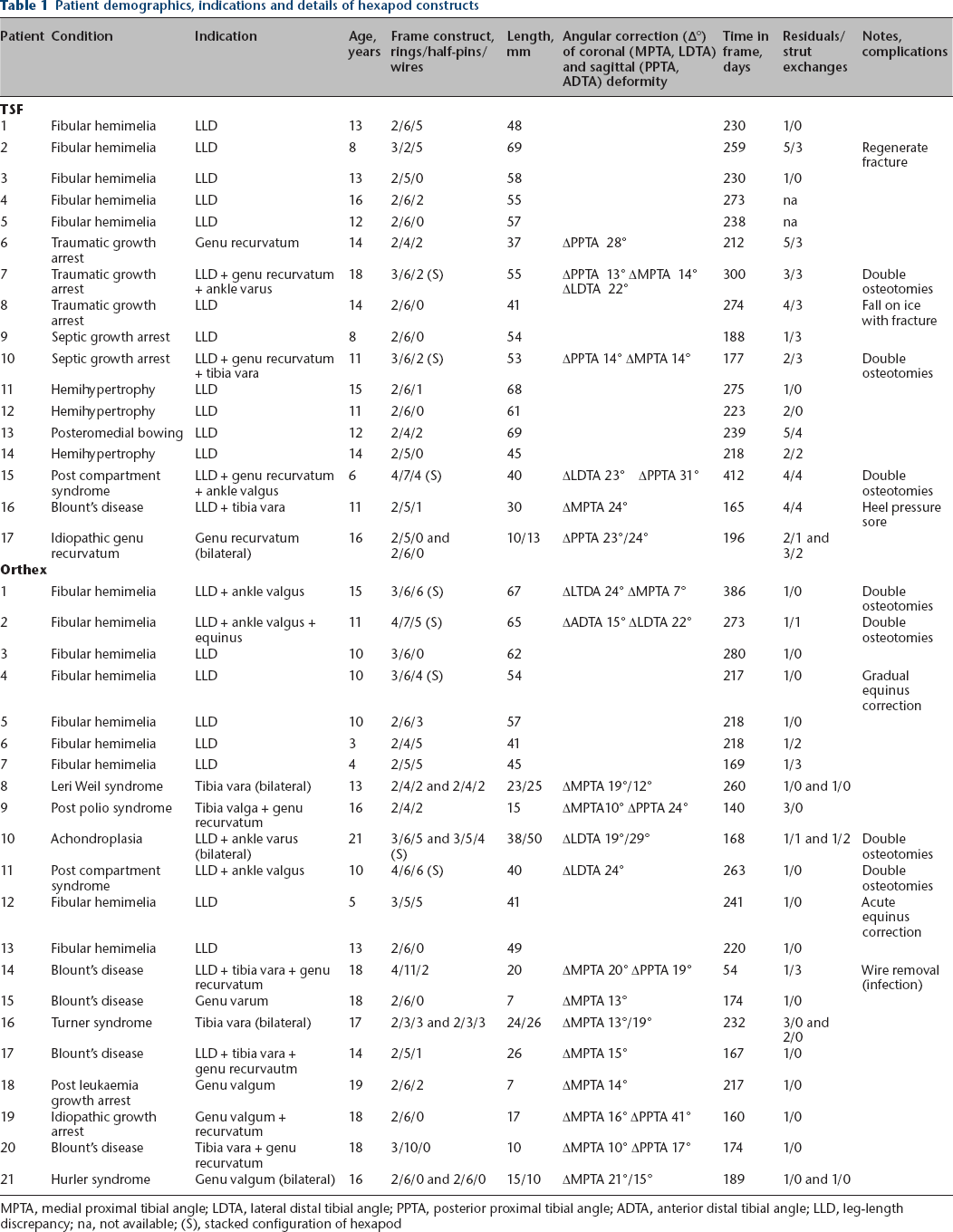
MPTA, medial proximal tibial angle; LDTA, lateral distal tibial angle; PPTA, posterior proximal tibial angle; ADTA, anterior distal tibial angle; LLD, leg-length discrepancy; na, not available; (S), stacked configuration of hexapod
In a total of 43 frames (Table 1), lengthening was the primary correction goal in 18 cases, 16 tibiae required simultaneous 3D corrections. Angular corrections in the coronal and sagittal plane with only minimal axial distraction was performed in nine cases. Correction was achieved through either a proximal osteotomy (standard) or with an additional distal osteotomy for angular correction. In cases with double osteotomies (n = 8) a stacked hexapod configuration was used. In the Orthex group, two patients in addition to lengthening had concomitant ankle equinus correction, one patient with gradual hexapod correction and one patient with acute soft-tissue correction and foot ring stabilization.
The median follow-up time was 52 months (13 to 65) in the TSF (between 2014 and 2016) versus 24 months (8 to 40) in the Orthex group (between 2016 and 2019) (p < 0.0001, Aspin-Welch t-test).
Set-up, operating time and radiation dose
The set-up and operating times did not differ between the groups. Set-up was a mean of 29 mins (14 to 61) in the TSF and 26 minutes (15 to 37) in the Orthex cohort (p = 0.53, equal variance t-test). Frame application including additional operative steps (i.e. tibio-fibular screw fixation (routine), 8-plate application or removal (n = 11) or distal femoral osteotomy (n = 4)) lasted for a median 211 minutes (143 to 336) versus 219 minutes (157 to 378), respectively (p = 0.48, equal variance t-test). The mean radiation dose measured by intraoperative fluoroscopy was 0.361 mG (0.136 to 0.847) in the TSF group versus 0.586 mG (0.108 to 3.390) in the Orthex group (p = 0.37, equal variance t-test). The mean time of radiation exposure was 70 seconds (35 to 102) and 76 seconds (22 to 128), respectively (p = 0.52, equal-variance-t-test).
Time in frame, length achieved and healing index
The median frame time was 230 days (165 to 412) for the TSF group and 203 days (54 to 386) for the Orthex group (p = 0.06, Mann-Whitney U test). Frames were removed when three out of four cortices were in continuity at the regenerate. The mean achieved lengthening was 54 mm (37 to 69) in the TSF group and 51 mm (38 to 67) in the Orthex group (p = 0.41, t-test). A median healing index (or external fixator index) was calculated as follows (for lengthening procedures only): 41 days/cm (33 to 66) versus 43 days/cm (34 to 57) (p = 0.70, Mann-Whitney U test).
Regenerate density and descriptive analysis
The regenerate bone density was measured at one month, three months and six months. The PVR was over 90% (> 0.9) in significantly more patients in the Orthex group at three months than the TSF group (72% versus 38%, p = 0.029, chi-squared test). The regenerate at six months was significantly more homogenous according to the Donnan classification in Orthex patients (73% versus 39%, p = 0.023, chi-squared test).
Strut exchanges and software residuals
In the TSF group strut exchanges were necessary in 11 out of 16 analyzed prescriptions (affecting 33 out of 114 struts). In the Orthex group exchanges were only necessary in six frames out of 25 (12 out of 180 struts). In total, 19 frames did not need any strut changes (p = 0.0008, Pearson's chi-squared test). Reprogramming or residuals were more often needed in TSF patients. In total, 12 out of 16 frames needed further residuals. Only three Orthex patients had residuals, 22 patients were managed within one prescription schedule (p = 0.0005, Pearson's chi-squared test).
Pin infection rate
Overall, the proportion of patients without any infection episodes throughout was 24% in the Orthex group (seven out of 26 frames) and 16% in the TSF group (three out of 18 frames) (p = 0.711, Fisher's exact test).
Orthex extended HA-coated half-pins and fine wires showed a lower infection rate compared with TSF fixation elements (particularly HA-coated half-pins and uncoated wires) (Table 2). We have also mapped the hotspots of half-pin infections for the hexapod ring construct (Fig. 1).
Infection data for both hexapod systems stratified in different hardware components and locations of applications (Pearson chi-squared test applied for contingency tables with odds ratios (OR) and 95% confidence intervals (CI))
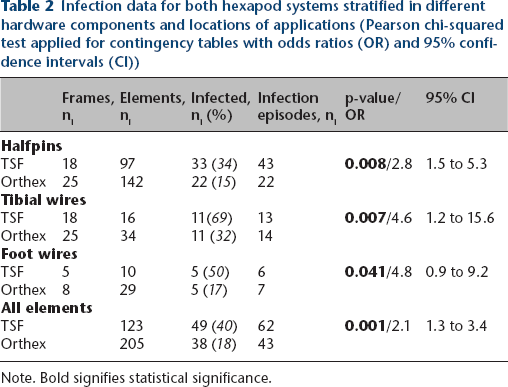
Note. Bold signifies statistical significance.
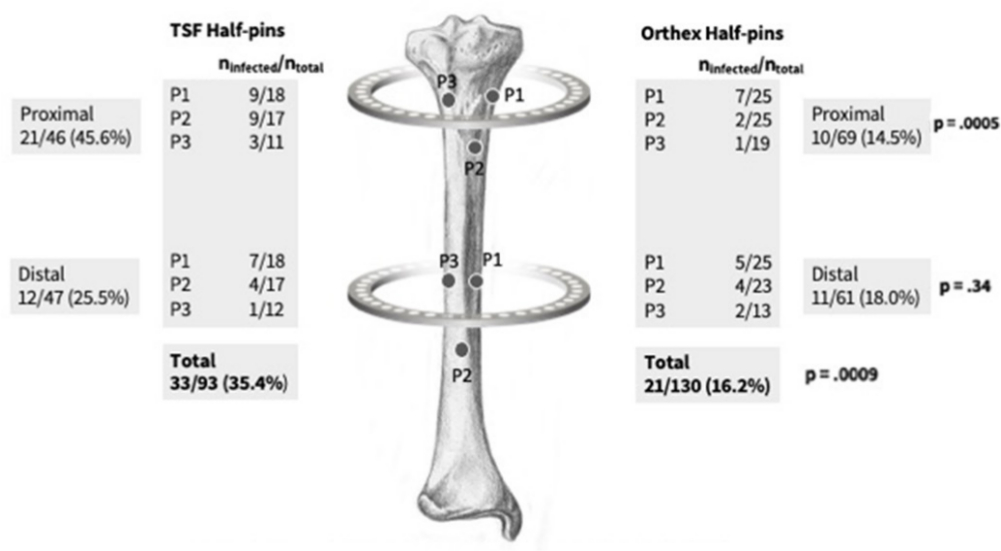
Topographical representation of half-pin placement and distribution (%) of infected pins (Taylor Spatial Frame (TSF) versus Orthex). Medially placed half-pins (P1 in ring 1 and 2) in TSF and Orthex constructs are most prone to infection. Overall infection rate for proximal, distal and total half-pins for both systems given in (ni) and [%] (ninf = number of infected half-pins, Pearson chi-squared test, p and odds ratio (OR)). Medial vs. lateral half-pin position infection risk OR 3.48(CI95% 1.39-8.83)p=.0053.
Infection rates (infection episodes during frame treatment) were analyzed in multiple regression analysis (Poisson) and significant predictors were ‘number of wires’ (estimate 0.217, 95% confidence interval (CI) 0.045 to 0.39; p = 0.013) and ‘extended HA coating’ (estimate -1.25, 95% CI -1.805 to -0.700; p < 0.0001). Age, time in frame, length achieved, presence of foot ring and number of half-pins were not significant predictors of infection in our model (multi-collinearity tested, Pseudo R squared 0.384; excellent McFadden fit: 0.2 to 0.4) (Table 3).
Results for multiple linear regression (Poisson) analysis for infection episodes (ni) as dependent variable (yi). Parameter estimates for each variable indicate higher rates (positive value) or lower rates of infection (negative values). Results in bold represent significant predictor variables in this model with other variables held constant. Pseudo R2 reflects predictive capacity of chosen model
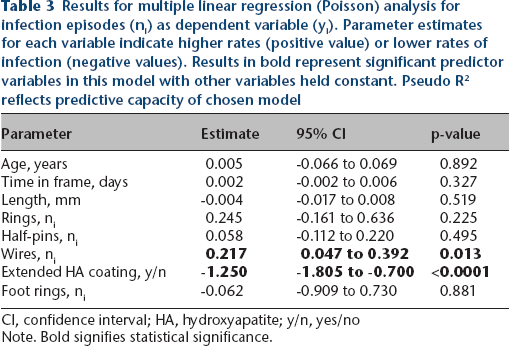
CI, confidence interval; HA, hydroxyapatite; y/n, yes/noNote. Bold signifies statistical significance.
Limb deformity correction
The axial lengthening frames were tested against the potential drift into valgus (increased MPTA) and procurvatum (decreased PPTA). Neither group showed any significant deviation from their baseline following axial lengthening. MPTA increased in the TSF group by a mean of 2.3° (-4° to 7°) and in the Orthex group by a mean of 0.1° (-7° to 4°) (p =0 .23, t-test). PPTA changed in the TSF group by a mean of -0.6° (-7° to 7°) and in the Orthex group by a mean of 1.6° (-7° to 10°) (p= 0.32, t-test).
Angular correction frames were tested for their capacity to normalize the mechanical axis, the MPTA and PPTA. Postoperative comparison for achieved correction did not differ between TSF and Orthex (Fig. 2).
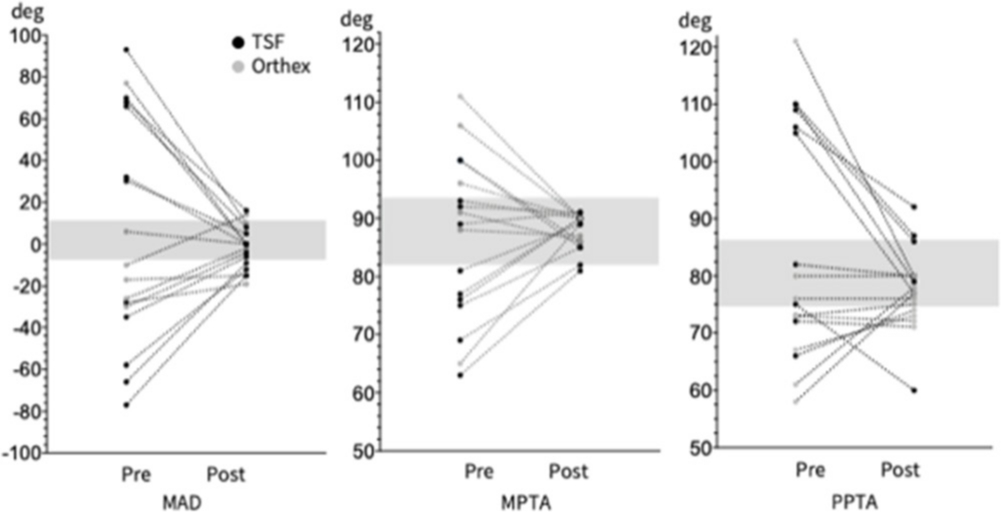
Pre- and postoperative limb deformity analysis (parameters are displayed in pairs). Mechanical axis deviation (MAD; normal: +10 mm medial to -6 mm lateral), medial proximal tibial angle (MPTA; 87° +/- 6°), proximal posterior tibial angle (PPTA; 81° +/- 6°). Parameters (MAD, MPTA, PPTA) do not differ between Taylor Spatial Frame (TSF) and Orthex post-correction (analysis of variance testing, p = 0.92, 0.99, 0.98) (deg, degrees).
Quality of life
The PedsQL scores were not statistically different in any module between groups (Fig. 1) at a minimum of six months following frame removal.
Discussion
To our knowledge, this is the first clinical study for tibial deformity correction comparing two hexapod systems in paediatric orthopaedics.
The TSF has been in use for over 20 years since its development by Charles and Harold Taylor. A recent systematic review of literature has found 100% consolidation rates in children. It has been widely used for acute and chronic deformity treatment.6,14–16 In comparison, the Orthex Hexapod System has only been recently introduced in the North America and has just been approved in Europe. This is the first study presenting clinical results using this novel design.
Both frame systems have produced satisfactory and predictable limb deformity correction. The intraoperative set-up and operating times and radiation exposure were similar.
The main technical difference is the TSF system's dependence on perfectly orthogonal intra- or postoperative radiographs of the reference ring to allow measurement of the mounting parameters form the centre of the ring to the origin on the reference segment. Inaccuracies introduced by the roll, pitch and yaw of the reference ring are accounted for in the Orthex system by uploading intraoperative radiographs with three calibration balls attached to the frame. Any unrecognized error in the positioning of the reference ring in the TSF is magnified by the lengthening process whereas in the Orthex it is automatically accommodated by the software. We hypothesize that this provides a more accurate representation of the relationship between the ring and the bone, reducing the amount of necessary residuals during or at the end of the correction phase and, therefore, the time spent in frame for the patient.
The need for strut exchanges was significantly reduced, saving on time spent in the outpatient department, reducing costs and reducing potential anxiety and pain involved with the exchange. This is certainly due to several design factors. The struts do not need to be attached to classic tabs found at every 60° of the ring but can be positioned anywhere on the ring, or even, outside the ring with an extension plate. In addition, the double telescoping nature effectively doubles the excursion of the Orthex struts and as such large struts were usually sufficient for the majority of Orthex cases.
The pin infection rate was significantly reduced in the Orthex group. Orthex half-pins have extended HA coating and are attached to the rings with double-column titanium blocks. A systematic review by Patel et al 17 has shown that HA-coated half-pins show less loosening but no overall reduction in infection rate was proven due to the heterogeneity of studies. We have also seen a reduction in foot and tibial wire infections episodes with fully HA-coated Orthex wires.
We believe that not only does the bone bind to the HA coating, but the extended coating also binds to the skin and soft tissue around the pin site, forming a biological seal, as seen in transcutaneous amputation devices with full HA coating. 18 This dry seal might play an important role in reducing the risk of infection (Fig. 3) as epidermal ‘downgrowth’ or pitting is a significant cause of infection.

Photograph of pin site with skin sealed around extended hydroxyapatite-coated half-pin.
Our multiple regression analysis would support the strategy to reduce the number of wires (or at least use HA-coated ones) and mainly use extended HA-coated half-pins in the frame construct. Increasing the number of rings or half-pins did not increase the infection rate. Interestingly, time in frame was not a predictor for infection, either. This might be related to patient characteristics (some patients never develop a pin site infection regardless of time spent in frame, 24% of Orthex and 16% of TSF patients) and infection episodes predominantly occurring during the correction phase, which is similar across all patients.
We have developed a robust system to capture infection data systematically. 19 Our topographical mapping found that medially placed half-pins were more prone to infection than laterally place ones. There was also a significant reduction in infection in the proximal half-pins in the Orthex system.
The PVR is a readily available way of assessing regenerate maturation during distraction osteogenesis and values between 0.8 and 1 have been validated for sufficient callus maturity,8,20,21 i.e. a PVR of 0.9 indicates a bone density of 90% in the regenerate compared with the adjacent bone segment by measuring the radiographic pixel density in the respective areas. We have seen an increased density of the regenerate at month three in Orthex frames compared with TSF frames (at a threshold of 0.9). This did not lead to a decreased healing index and at six months density levels were equal among the frame groups. In descriptive analysis, using the Donnan classification, 7 the Orthex regenerates were more homogenous compared with those in the TSF group, which still had some lucencies at that time point. Lucency was not seen in any patient in the Orthex group. Our thinking here is that the regenerate forms more uniformly with 0.25 mm steps (one click = 0.25 mm) with the Orthex struts compared with 1 mm step (1 click = 1 mm) of the TSF strut, leading to a more homogenous and denser regenerate. However, the overall healing index was not affected by these differences.
In terms of quality of life measures, PedsQL, the data have not shown any significant differences between groups in terms of physical, social and psychological outcomes after frame removal. We have shown that limb deformity correction restores overall quality of life measurers to a level which is comparable with a healthy population mean in the majority of our patients (shaded area Fig. 4).
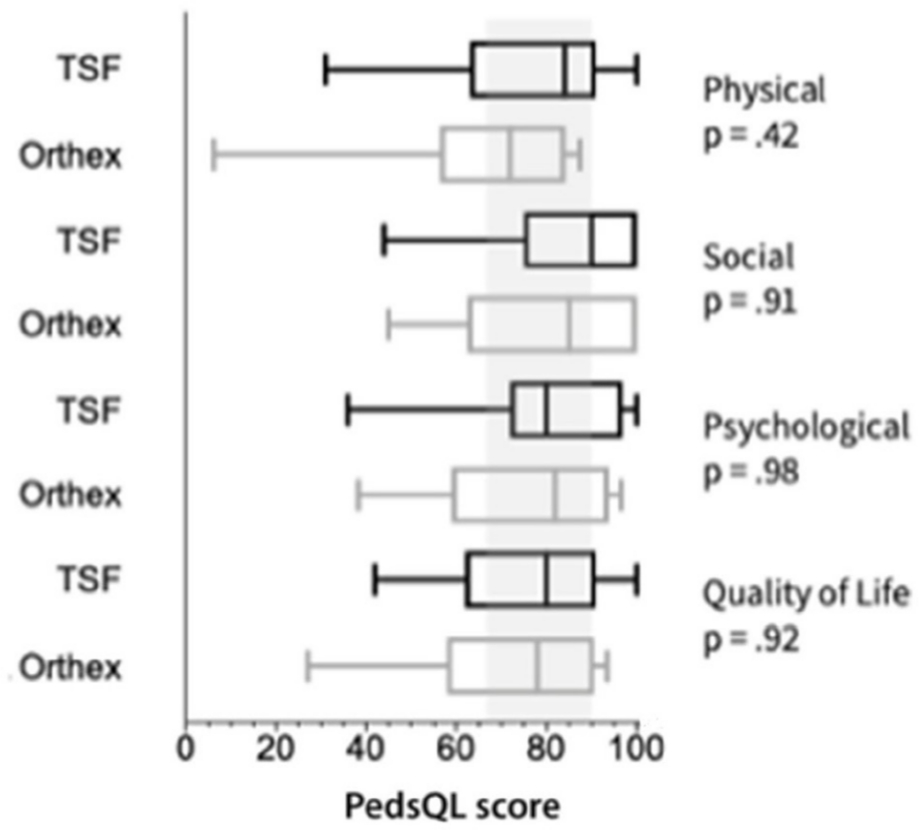
Quality of life measure (PedsQL) data comparison between frame groups (box and whisker plot with 10% to 90% range). Shaded area is standard population norm +/- sd. One-way analysis of variance testing adjusted p-values are given (TSF, Taylor Spatial Frame).
This study has several limitations. Foremost, the retrospective study design might inadvertently introduce selection and outcome bias and does not allow for prospective sample sizing or power analysis. The numbers in both cohorts are small and the encountered tibia deformities are the result of a variety of conditions as outlined in Table 1. As such the findings of this study may be subject to Type 1 or Type 2 error. The treatment goal always included a multi-planar correction, even in patients undergoing lengthening to prevent valgus and procurvatum drift, but we accept that angular and axial deformity corrections might differ in clinical outset and treatment duration. Therefore, any conclusions comparing specific conditions within or between groups are not possible or valid. Finally, we felt a universally acceptable cost analysis comparison was not possible due to healthcare system and institutional variations. However, cost implications for either system are important when considering their use.
To our knowledge, this is the first study to compare these two systems. The Orthex Hexapod System achieved similar healing indices and limb deformity correction. It showed superiority in regenerate quality and a significant reduction in pin site infection rates. In addition, fewer residuals and strut changes were necessary. Further analysis is planned to measure the improvement in the patients’ experience, biomechanical differences between the frame and potential cost savings to the healthcare system.
Footnotes
The other authors declare no conflict of interest relevant to this work.
HC: Study design, Data collection, Data management, Manuscript editing.
SD: Data collection, Database management.
JA: Data collection, Database management.
AC: Study design, Analysis, Manuscript editing.