
Abstract
Background
The Taylor spatial frame (TSF, Smith and Nephew, Memphis, TN, USA) is a modern multiplanar external fixator that combines ease of application and computer accuracy. Many patients in our geographic area seek treatment for their fractures by traditional bonesetters and present in the middle of treatment with neglected malaligned fractures. These fractures were an average of 10 weeks old (range 6–14 weeks) fractures with callus that were allowed to heal in a poor position. The spatial frame is applied easily on the fracture bone fragments. The accuracy of fracture reduction and deformity correction is dependant on analyzing anteroposterior and lateral radiographs of the fracture. Our experience with this external fixator in the treatment of neglected fractures is summarized.
Method
Over a period of 6 years, the TSF was used in 24 neglected fracture cases which were collected from our prospective external fixator data base. All cases were followed for a minimum of 3 years. The data base and radiographs were reviewed in order to obtain demographic data, malalignment parameters, final correction, time in the TSF, and complications.
Result
The patients’ ages ranged from 6 to 18 years. All were neglected fractures. The average delay in treatment was 10 weeks (range 6–14 weeks). All patients had closed osteoclasis. The time spent in the TSF varied according to the patient age and bone involved. Ten femoral and 14 tibial fractures were included. Ten patients had superficial pin site infections that resolved with oral antibiotics. Postoperatively, no patient was noted to be more than 5° malrotated on clinical examination and no functional leg length discrepancy was observed. All of the fractures united.
Conclusion
Anatomic alignment was achieved in all tibial fracture patients. At the final follow-up, fracture angulation and shortening were fully corrected, and some translational malalignment persisted in 67% of femur fractures. The TSF is an effective definitive method for the treatment of neglected fractures.
Level of evidence
IV.
Introduction
Many patients in our geographic area, the Middle East, seek treatment of their fractures by traditional bonesetters who use local herbal application and inadequate splinting in the treatment of the fractures, the majority of which result in nonunion or malunion, especially in the pediatric and adolescent patient population. Some patients seek orthopedic surgeons’ advice in the middle of traditional treatment if obvious deformity is appreciated during the course of treatment [1–4]. In peripheral hospitals, many patients opt for nonoperative treatment, refusing the surgical option and resulting in deformity and limb length discrepancy. In addition, we observe a large number of patients self-referred from neighboring countries owing to the lack of adequate equipment and trained staff in their geographic areas. Malalignment of these fractures cause considerable morbidity, change in gait, and, sometimes, significant limb length discrepancy.
To treat such fractures, the Taylor spatial frame (TSF) was thought to provide ease of application and computer accuracy. It provides the capability of 1–6 axes of deformity correction sequentially or simultaneously. Indirect reduction of fractures is achieved by realigning one fracture end to the other through a spatial point of rotation [5]. Previous reports documented the effectiveness of the TSF in acute fracture care, particularly in obtaining and maintaining reduction until union [5–7].
The purpose of this article is to determine the effectiveness and complications of the use of the TSF in the treatment of neglected fractures in the pediatric and adolescent patient population as a treatment alternative for subacute fractures that are shortened, angulated, or malrotated, stressing the concept of obtaining gradual correction through healing fracture callus.
Methods
We defined neglected fractures as 6–14-week-old fractures with callus that were allowed to proceed to heal in a poor position but cannot be called a malunion because it is not fully healed. From February 2001 through February 2007, 24 neglected fracture cases were identified from our TSF data base. A retrospective review of these 24 patients was carried out. All patients were followed until union of the neglected fracture. No patient was lost to follow-up. Mainly, three types of neglected fractures were encountered in our institute: fractures treated by traditional bonesetters with persistent malalignment, malaligned fractures after nonoperative management in other health care facilities, and malaligned fractures self-referred from a neighboring country.
Patient charts were retrospectively reviewed for the demographic data, mechanism of injury, associated injuries, previous treatment modalities, current surgical data, complications, number of operative procedures after the index admission procedure, and time spent in the frame. Personal interviews were conducted in order to determine the functional outcome, especially changes in conducting activities of daily living or sports and whether patients and their parents would opt for a similar treatment again if the choice were to be given again. Radiographs were reviewed to assess the fracture location, displacement, angulation, limb length discrepancy, union, and final postoperative alignment.
There were 14 tibial fractures and ten femoral fractures. These tibial and femoral shaft fractures were subdivided according to location into five regions: proximal third, proximal/middle junction, middle third, middle/distal junction, and distal third. A sixth category, “segmental,” was used for fractures involving two noncontiguous regions. Two of the neglected tibial fractures were open and had original irrigation and debridement in a peripheral hospital, and were then externally fixed with inadequate monolateral frames that were removed prematurely in the referring facility. These two fractures were classified as one Type IIIA fracture, which was covered by means of a split-thickness skin graft and the second as a Type IIIB fracture, treated with rotational myoplasty for soft tissue coverage [8–10].
A single surgeon treated all fractures using the TSF and followed standard guidelines for external fixator application.
Surgical technique
Prophylactic cephalosporin antibiotics were administered preoperatively to all patients. Details of the frame application were mentioned in previous articles using the ring first technique [5, 6].
After frame application, TSF struts were disconnected and, in the neglected femoral fracture cases, closed manual osteoclasis of the fractured bone was performed, with none requiring drill osteoclasis. Once fractured fragments appear mobile clinically and under the image intensifier, the six struts were reconnected and the patient was awakened and transferred to the recovery room with planned gradual correction postoperatively. In neglected tibial fracture cases, no attempt at osteoclasis was performed, as the amount of healing callus is usually small. The deformity correction start date was after a latency period of 5 to 7 days in cases that required manipulation and the first postoperative date in the others.
Anteroposterior and lateral radiographs were then taken. The radiographs were analyzed for deformities present at the neglected fracture site. Details of the online planning program and deformity analysis were mentioned in previous publications [5, 6].
Strut adjustments were done gradually in the postoperative period in order to avoid excessive soft tissue damage. The way point technique of correcting length first in order to avoid the impingement of fracture ends were used in all of the cases, followed by corrections of other deformities of angulation and translation [5, 6]. If anatomic reduction was not present on the first postreduction radiographs, fine tuning using the total residual mode again was then used to obtain perfect alignment, according to the adjustment schedule, which was generated by the computer program.
Partial weight-bearing was initiated on the first postoperative day and gradually advanced according to fracture healing. Patients were followed in the outpatient clinic every 2 weeks. Fractures were determined to be healed after evidence of tricortical callus and lack of tenderness at the fracture site. The TSF was removed in an outpatient surgery unit under sedation and no postoperative immobilization was needed in all cases. Patients were then seen after one week for pin site wound check, then every three months for two visits, and then yearly. Personal interview of the patients and/or the parents were conducted to determine the functional outcome as described earlier, especially changes in conducting activities of daily living or sports participation, and whether patients and their parents would opt for a similar treatment again.
Results
Of the 24 patients, 23 were males. The average age of the patients at the time of injury was 16 years, with a range from 6 to 18 years. The mean duration of follow-up was 3 years (range 2–5 years). The mechanism of injury was a car versus pedestrian in ten patients, motor vehicle accident in eight patients, all-terrain vehicle injury in five patients, and sports injury in one patient.
Two patients had significant associated injuries, including closed head injury in one patient and pulmonary contusion in the other.
The fracture location for the 14 tibial fractures was as follows: two proximal third, two middle third, six middle/distal junction, three distal third, and one segmental fracture. The fracture location for the ten femoral fractures was as follows: three proximal/middle junction, four middle third, and three middle/distal junction.
Of this group of patients, 15 were splinted by bonesetters before referral to our facility and four tibial and three femoral fractures failed attempted cast treatment by the referring orthopedic surgeons. Two open tibial fractures had irrigation and debridement followed by 6 weeks of external fixation; both frames were removed prematurely by the referring surgeon because of loose pins. Delay between fracture occurrence and application of the TSF averaged 10 weeks (range 6–14 weeks). The total operative time averaged 92 min (range 68–134 min). Manual osteoclasis were utilized in all neglected femur fractures. No acute manipulation was done for the tibial fractures because of the lack of significant hypertrophic callus in these cases when compared with the femoral fractures.
No patient required return to the operating room for frame adjustment or grafting. Total residual programs were utilized at least 4 sequential times on average in order to gain the desired reduction (range 3–7 times).
The neglected fractures healed over a mean of 15 weeks (range 12–20 weeks). Patients remained in the external fixator for a mean of 17 weeks (range 13–25 weeks), which varied from the healing time because most of the patients waited for the availability of a slot in the outpatient surgical care unit. All patients were not experiencing any pain in their last follow-up. No patient was noted to be more than 5° malrotated on clinical examination. No patient had a functional leg length discrepancy, with an average leg length discrepancy of 4 mm (range 0–8 mm), as measured from the standing lower extremity anterior posterior full-length radiographs.
Angulation was measured using a standard goniometer on the long-bone radiographs.
The mean preoperative angulation of the neglected fractures on the anteroposterior radiograph was 17° (range 5–34°). The mean preoperative translation on the anteroposterior radiograph was 48% (range 0–100%). The mean preoperative angulation on the lateral radiograph was 9° (range 0–30°). The mean preoperative translation on the lateral radiograph was 50% (range 5–100%). The mean final angulation on the anteroposterior radiograph was 2° (range 0–5°). The mean final translation on the anteroposterior radiograph was 4% (range 0–30%). The mean final angulation on the lateral radiograph was 3° (range 0–5°). The mean final translation on the lateral radiograph was 9% (range 0–40%). When neglected femoral fracture cases were analyzed separately, translational deformity appeared to be less corrected when compared to tibial cases. The mean preoperative translation on the anteroposterior radiograph was 64% (range 25–100%), and the mean preoperative translation on the lateral radiograph was 81% (range 25–100%). The mean final translation on the anteroposterior radiograph was 8% (range 0–30%), and the mean final translation on the lateral radiograph was 24% (range 5–45%), which is likely related to the large amount of callus around the healing fracture ends (Figs. 1 and 2).
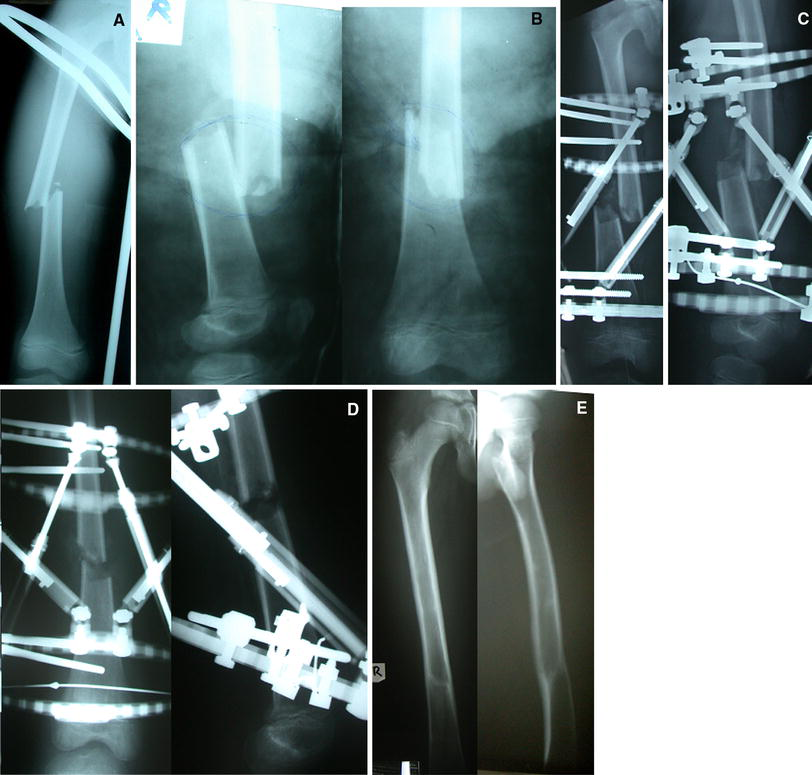
A 7-year-old boy with a 7-week-old neglected femur shaft fracture

A 16-year-old male patient with an 8-week-old neglected tibial shaft fracture that failed closed reduction during preparation for intramedullary nailing and it was decided to proceed with the TSF.
All of the neglected fractures ultimately united, including patients with segmental and open fractures, without the need for bone grafting. There was no loss of reduction or return to the operating room for remanipulation.
There were no intra-operative complications. Postoperative complications included superficial pin tract infection in six patients, all of which resolved with oral antibiotics, and no patient developed osteomyelitis, neurovascular injury, or had a refracture. All patients had a normal range of motion of their hip, knee, and ankle on clinical examination during their last follow-up visit.
When personal interviews were evaluated. All patients were doing well at the final interview, all patients had no changes in conducting activities of daily living, and were involved in sports when last seen, including patients with other significant associated injuries. When the patients or parents were asked whether they would go for this surgical intervention again if the choice were to be given again, all of them said they that will be happy to do so.
Discussion
The TSF provides an easy and precise method to achieve correction of deformities associated with neglected fractures. Computer accuracy has brought external fixation to the next level. This is particularly true for acute fracture care, especially of the tibia. Being a multiplanar external fixator, it provides the possibility for excellent fracture reduction [5, 6]. It also allows stability for early weight-bearing function and the versatility to treat neglected fractures of the long bones.
One of the major problems we are facing in our practice area is the cultural and economic situation of having poorly educated bonesetters commonly providing the primary orthopedic trauma care, which creates a significant challenge.
No previous reports in the English literature discussed the use of external fixation for the precise reduction of neglected fractures. Neglected fractures remain a fairly common encounter in our area. The TSF provides a treatment alternative for subacute fractures that are shortened, angulated, or malrotated. To the author's knowledge, this is the first report to discuss use of the TSF in neglected fractures of femur and tibia while stressing the concept of obtaining gradual correction through healing fracture callus. Al-Sayyad previously described his encouraging results in the acute fracture setting with the use of the TSF in treating ten unstable tibial fractures, including five open fractures, with a mean fracture healing time of 18 weeks [10]. Also in acute fractures, Eidelman and Katzman reported on the treatment of complex tibial fractures in children and adolescent age groups with the TSF and described the experience as a rewarding treatment modality for complex tibial fractures in that age group [11]. Gessmann et al. reported on the use of the TSF in children open fractures. The authors used the concept of acute angular shortening of the fracture, enabling primary soft tissue closure, which is still an uncommon operative technique because of difficulties in correcting the secondary deformity. They described cases of pediatric open fractures of the lower limb (Gustilo type IIIa), which were treated successfully with acute angular shortening followed by gradual correction using the TSF [12]. Eidelman et al. also reported on the treatment of posttraumatic deformities in children and adolescents using the TSF. Eighteen patients with posttraumatic deformities were treated, with an average age of 13 years. All had established malunion, one radial, three femoral, and 14 tibial. In this series, all patients required percutaneous osteotomies. One patient had angulation of the regenerate and required frame adjustment with successful correction afterwards. The authors reported that, despite complex deformities, all patients achieved precise correction of all deformities [13].
The current study discusses a unique group of patients with neglected fractures that were malaligned into a deformed and shortened position. The author used the TSF, which is a modern multiplanar external fixator that combines ease of application plus computer accuracy in the reduction of these fractures; indirect reduction of the fracture is achieved by realigning one fracture end to the other through a spatial point of rotation after performing manual osteoclasis if needed, depending on motion between the fractured segments of bone, without the need for extensive surgical exposure.
Basically, the TSF provides a form of indirect reduction techniques, which are well documented through the corrections achieved. In our series, no significant postoperative complications occurred, six patients had superficial pin tract infections, and all resolved with oral antibiotics. No patient developed osteomyelitis, neurovascular injury, refracture, delayed union, malunion or significant joint stiffness, or the need for remanipulation under general anesthesia. With TSF use in neglected fractures, satisfactory alignment was achieved in 100% of tibial and pediatric femur fracture patients. Some translational malalignment remained in 50% of adolescent femur fracture patients, but without affecting the functional status. The TSF is an effective definitive method for the treatment of neglected fractures. With our surgical technique, we tried our best to disturb as little as possible this callus through gentle manual osteoclasis, which is a technique that is minimally invasive to the fracture site and which allows its manipulation postoperatively, providing a proper environment for the fast healing of the neglected fracture. This technique proved to be safe in our hands without any complications related to manual manipulation. If the treating surgeon feels that excessive force is needed, they should utilize other techniques, such as percutaneous drilling of the callus and cutting it with an osteotome to help separate the fracture fragments, which we did not need to perform in our series.
It is well documented in the literature that refractures after fixator removal are avoided by using a proper technique of the insertion of appropriately sized half-pins, use of a more modular multiplanar external fixator along with gradual dynamization, and appropriate timing of fixator removal with at least three visible cortices, as well as postremoval protection of the fractured limb by avoiding impact, contact, collision activity, and aggressive physiotherapy [14–17]. All points mentioned here to avoid refractures were strictly followed in the author series and no refractures were encountered.
In summary, the TSF is an external fixator that can be successfully used as a treatment alternative for the definitive treatment of neglected fractures in the tibia and femur from reduction to healing. The technique is minimally invasive to the fracture site. The neglected fracture site can be manipulated postoperatively over several days into excellent alignment in outpatient bases with no need for remanipulation in the operating room. The fixator is stable enough to allow early functional weight-bearing and active motion of adjacent joints, as demonstrated in this patient series.
Footnotes
No funds were received in support of this study.