
Abstract
Abstract
Purpose
This article examines if longer posterior spinal fusions with instrumentation (PSFI) into the lumbar spine (L3/4) alter spinopelvic parameters compared with selective fusions to T12/L1/L2 in adolescent idiopathic scoliosis (AIS) patients.
Methods
We analysed radiographs of 84 AIS patients, 58 (69%) females and 26 (31%) males, who underwent PSFI at an mean age of 15 years ± 2.5 years, range 10 years to 21 years, between 1st January 2007 and 31st December 2014. Radiographic parameters were measured pre- and post-operatively at most recent follow-up (range 2 years to 8.2 years): pelvic incidence (PI), lumbar lordosis (LL, L1–S1 and L4–S1), sagittal vertical alignment (SVA), scoliosis angle and proximal junctional kyphosis (PJK). PI–LL was calculated. Data was analysed using t-tests or Wilcoxon rank-sum tests.
Results
In total, 32 patients underwent a selective fusion with lowest instrumented vertebra (LIV) T12–L2, and 52 patients underwent a fusion with LIV L3–L4. In both groups, scoliosis angle was significantly corrected at follow-up (p < 0.005).
Pre-operatively, both groups had similar LL (L1–S1) and PI–LL. Post-operatively, LL increased in the L3–4 fusion group (p < 0.005) but did not change in the selective fusion group (p = 0.116). This change in LL in the L3–4 fusion group affected the post-operative PI–LL (T12–L2 fusion -4.9° versus L3–4 fusion -13.6°, p = 0.002). No differences were seen in PI, SVA or LL L4–S1 between groups. Radiographic PJK occurred in seven of the L3–4 patients with and without PJK (noPJK –8.8° versus PJK –25.8°, p = 0.026).
Conclusions
In patients who underwent a fusion ending at L3 or L4, LL was increased. This altered the PI–LL relationship, and appeared to increase the risk of PJK.
Level of evidence
III
Introduction
Sagittal spinal alignment is determined by different factors including thoracic kyphosis (TK), lumbar lordosis (LL) as well as the orientation of the pelvis and the sacrum.1–3 Pelvic incidence (PI) is a unique fixed morphological parameter for each individual that reflects the pelvic anatomy and does not vary with spine or pelvis orientation. 4 In the paediatric population, PI tends to increase during childhood and adolescence then stabilize during adulthood, with the mean PI in adolescents reported as 49.1° ± 11° and the mean PI in adults being 51.8° ± 5.3°. 5 PI is fixed and its degree should be comparable to the amount of LL required to assume a balanced sagittal posture.6–8 It has been previously proposed that in the healthy adult population with and without scoliosis, LL is approximately the sum of PI ± 9°. 9 While numerical values of sagittal and spinopelvic parameters may differ between paediatric and adult populations, their relationships are similar. 10
The impact of spinopelvic alignment on clinical outcomes has received attention in the adolescent and adult spine literature. Makino et al reported that larger LL (L1–S1) is a risk factor for pain at rest in non-surgical adolescent idiopathic scoliosis (AIS) patients. 11 Following adult spinal deformity surgery, Lafage et al reported that the loss of LL significantly correlated with poorer outcomes in ODI (walking and standing component) and SF12 (bodily pain and PCS), 12 and Schwab et al identified the clinically relevant cutoff value as LL = PI ± 9°. 8 In patients with a mismatch between their LL and PI, poorer outcomes, earlier degenerative changes, greater self-reported pain and disability were reported.1,8,12–14 These findings emphasized the role of LL as an important sagittal parameter to consider during surgical correction of spine deformities in order to achieve optimal clinical outcomes. In children and adolescents with scoliosis, pre- and post-operative spinopelvic alignment, specifically LL, has become of major interest in surgical planning to maintain/restore pelvic sagittal alignment and coronal balance.9,15–21 To maintain spinopelvic alignment, Tanguay et al suggested that surgeons should provide sufficient LL within a posterior spinal fusion (PSF), especially when instrumentation extended distally, 21 since these patients have poorer long-term outcomes.22,23 While multiple authors have investigated spinopelvic balance in AIS, the relationship between PI and other sagittal parameters with regard to distal fusion level have been inconsistently reported.19,21,24–30 The purpose of this study is to compare sagittal alignment and spinopelvic parameters in patients with AIS before and after posterior spinal fusions with instrumentation (PSFI).
Materials and methods
In total, 147 patients with a diagnosis of AIS underwent PSFI by one of five surgeons at a single institution in the study time period from 1st January 2007 to 31st December 2014; 84 patients, 26 male and 58 female, remained after inclusion and exclusion criteria were met. Inclusion criteria were: (1) availability of pre- and post-operative standing AP and lateral radiographs of the spine and pelvis with visible femoral heads and C7 vertebral body, (2) minimum follow-up of two years, (3) AIS diagnosis, and (4) surgical correction by PSFI with distal fusion level at or below T12. Exclusion criteria were (1) prior spine surgery, (2) revision spine surgery, (3) history or clinical signs of hip, pelvic or lower limb disorder, (4) the presence of a spondylolysis or spondylolisthesis. Proximal fixation of PSF instrumentation included hooks in one patient with a T2–L1 fusion, in all others pedicle screws were used.
Radiographic parameters were measured pre and postoperatively on conventional radiographs at most recent follow-up, mean follow-up 2.9 years (range two years to 8.2 years). Two measurers performed the following radiographic measurements:
Pelvic incidence (PI) – angle between the perpendicular of the upper endplate of S1 and the line joining the middle of the upper endplate of S1 and the point midway between the centres of the femoral heads (Fig. 1).
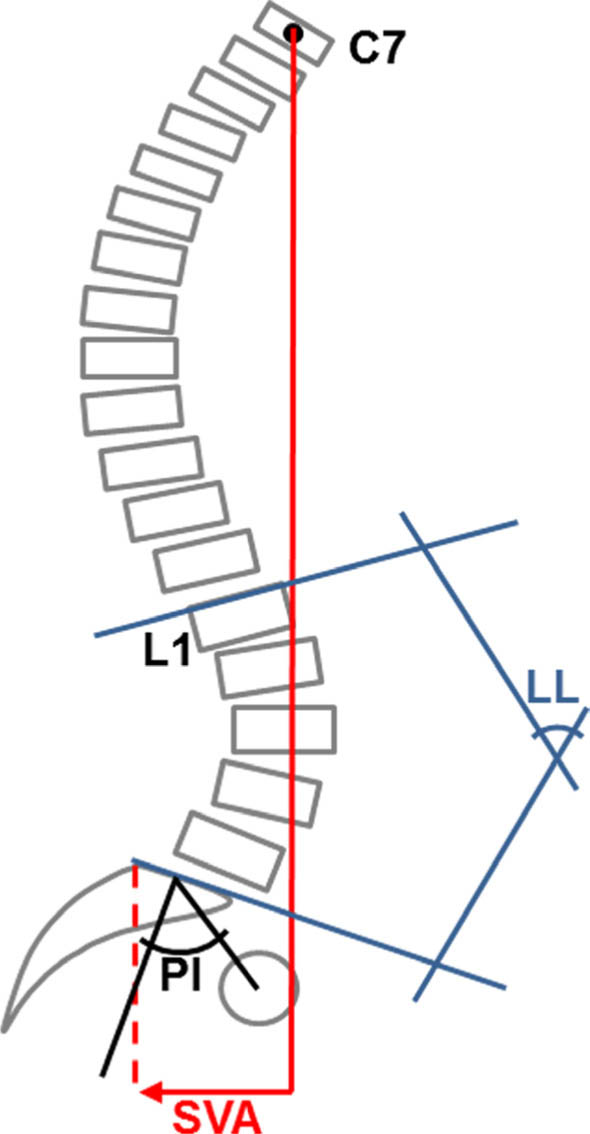
Sagittal pelvic parameters measured on the standing lateral radiograph adapted from Lim JK, Kim SM. Difference of sagittal spinopelvic alignments between degenerative spondylolisthesis and isthmic spondylolisthesis. J Korean Neurosurg Soc. 2013 Feb;53(2):96–101.
Lumbar lordosis (LL) – angle between the upper endplate of L1 (L1–S1) or the upper endplate of L4 (L4–S1) and the lower endplate of S1 (Fig. 1).
PILL - calculated by subtracting the LL(L1-S1) from PI.
Sagittal vertical alignment (SVA) – the distance between the vertical line extending from the centre of the C7 vertebrae and the posterior superior corner of S1 (Fig. 1).
Scoliosis angle (Cobb method) – angle between the upper endplate of the curve and lower endplate of the major curve.
Pelvic tilt (PT) – angle between the vertical reference line and the line from the centre of the femoral head and the midpoint of the sacral endplate.
Thoracic kyphosis (TK) – angle between the upper endplate of T2 or T5 to the lower endplate of T12.
Sacral slope (SS) – angle between the sacral endplate and the horizontal reference line.
For all measurements of spinopelvic parameters, the inter-rater reliability between the two measurers was excellent (inter-rater correlation coefficients r > 0.94; Supplemental Table 1).
Demographics
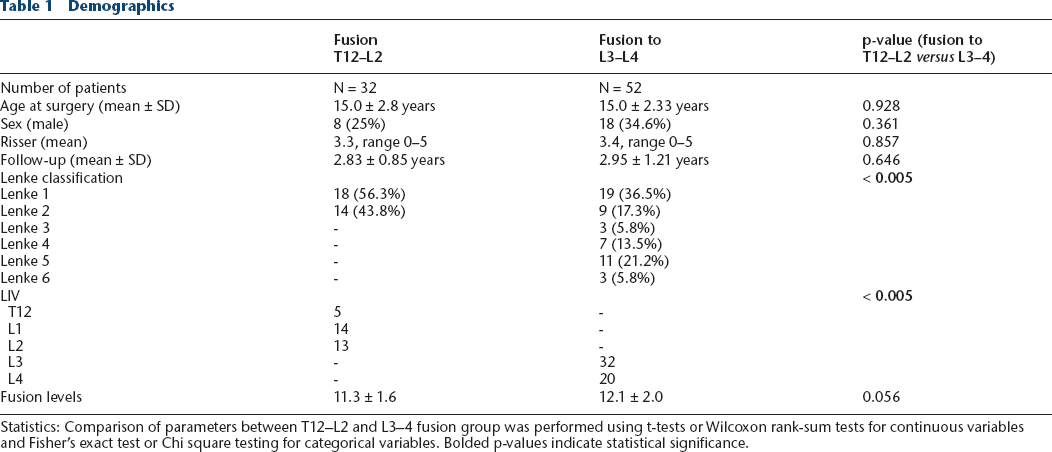
Statistics: Comparison of parameters between T12–L2 and L3–4 fusion group was performed using t-tests or Wilcoxon rank-sum tests for continuous variables and Fisher's exact test or Chi square testing for categorical variables. Bolded p-values indicate statistical significance.
Statistics
Analysis of all data was carried out using SPSS Version 24.0 software (IBM, Armonk, New York, USA). For all parameters measured, the mean of the two measurements was used for analysis. Inter-rater reliability was assessed using inter-class correlation.
Patients were classified into two groups for analysis: selective fusion group with lowest instrumented vertebra (LIV) at T12–L2, inclusive, and L3–4 fusion group with LIV at L3 or L4. Changes between pre- and post-operative radiographic parameters for the entire cohort and within each surgical group were assessed using paired t-test statistic. Radiographic parameters between T12–L2 and L3–4 fusion group and comparison of patients with PJK and without PJK were performed using t-tests or Wilcoxon rank-sum tests. A p-value < 0.05 was considered statistically significant.
Results
Demographics
In all, 84 AIS patients were included in the study. The T12–L2 fusion group had 32 patients with an mean age of 15 years ± 2.8 years (range 10.4-21.3 years), Risser 3.3, male 25%, and 2.8 ± 0.9-year follow-up. The L3–4 fusion group had 52 patients with mean age 15 years ± 2.3 years (range 10.6-20.6 years), Risser 3.4, male 34.6%, and 3.0 years ± 1.2-year follow-up. There was no significant difference between the two groups regarding age, sex, Risser stage, number of levels fused or follow-up (Table 1). Lenke classification differed between groups (p < 0.005); scoliosis curves of patients in the T12–L2 fusion group were classified exclusively as Lenke type 1 and 2, whereas curves of patients in the distal L3–4 fusion group were classified as Lenke type 1 to 6 (Table 1). LIV was chosen by each surgeon based on the Lenke classification and the location of the central sacral vertical line (CSVL) in relationship to pedicles of the apical lumbar vertebra.
Spinopelvic parameters
Coronal curve correction
While the pre-operative scoliosis angle of the main thoracic curve was similar between the T12–L2 fusion and L3–4 fusion group (53.5° versus 52.4°; p = 0.731), the proximal thoracic (T12–L1 31.6° versus L3–4 25.6°; p = 0.043) and thoracolumbar/lumbar curves (T12–L1 28.1° versus L3–4 41.3°; p < 0.005) were significantly different (Table 2). PSFI significantly reduced/corrected the scoliosis angle in the proximal thoracic, main thoracic and thoracolumbar/lumbar spine in both groups at last follow-up (p < 0.005 for each curve location). Only the change in scoliosis angle in the thoracolumbar/lumbar spine, not the proximal or main thoracic spine, was different between groups (Δ Scoliosis angle TL/L: T12–L2 –13.7° versus L3–4 –25.0°, p < 0.005) (Table 2).
Pre- and post-operative spinopelvic parameters
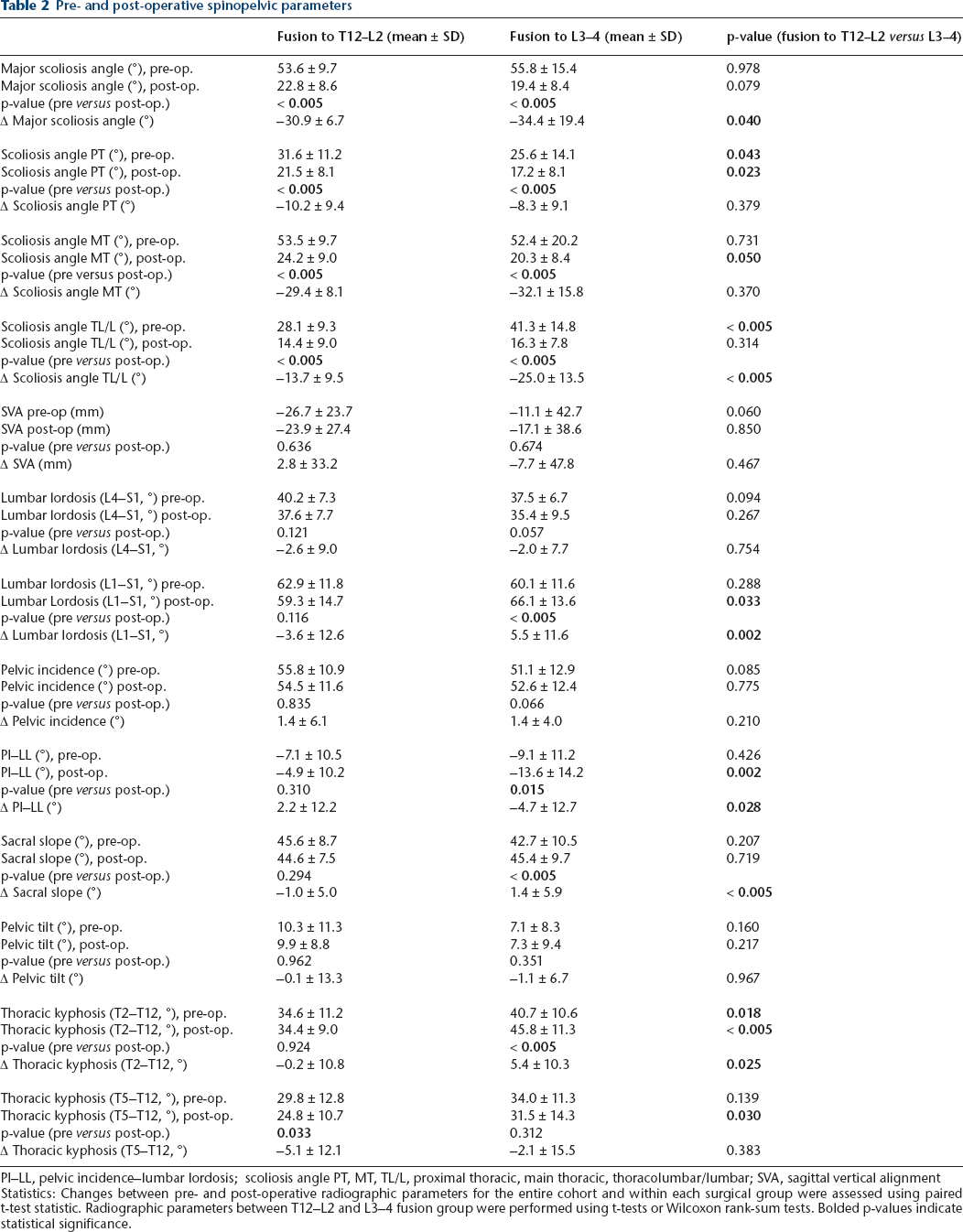
PI–LL, pelvic incidence–lumbar lordosis; scoliosis angle PT, MT, TL/L, proximal thoracic, main thoracic, thoracolumbar/lumbar; SVA, sagittal vertical alignment
Statistics: Changes between pre- and post-operative radiographic parameters for the entire cohort and within each surgical group were assessed using paired t-test statistic. Radiographic parameters between T12–L2 and L3–4 fusion group were performed using t-tests or Wilcoxon rank-sum tests. Bolded p-values indicate statistical significance.
Thoracic kyphosis
Pre-operative thoracic kyphosis (T2–T12) of L3–4 fusion patients was greater compared to patients who underwent a T12–L2 fusion (p = 0.018) (Table 2). In addition, thoracic kyphosis (T2–T12) significantly increased in the L3–4 fusion group after PSFI (p < 0.005) but not in the T12–L2 fusion group (p = 0.924), resulting in a significant pre- to post-operative change in thoracic kyphosis between groups (p = 0.025).
Spinopelvic alignment
Pre-operatively, PI and LL (L1–S1) were similar between the two groups. PI was 55.8° ± 10.9° in the T12–L2 fusion group and 51.1° ± 12.9° in the L3–4 fusion group (p = 0.085). LL (L1–S1) was 62.9° ± 11.8° in the T12–L2 fusion group and 60.1° ± 11.6° in the L3–4 fusion group (p = 0.288). PI did not change pre- to post-operatively in either group (Table 2). However, LL (L1–S1) increased significantly in the L3–4 fusion group from 60.1° ± 11.6° pre-operatively to 66.1° ± 13.6° post-operatively (p < 0.005) but did not change in the T12–L2 fusion group with 62.9° ± 11.8° pre-operatively to 59.3° ± 14.7° post-operatively (p = 0.116). Post-operative LL (L1–S1) was therefore significantly larger in the L3–4 fusion group compared to the T12–L2 fusion group (p = 0.033).
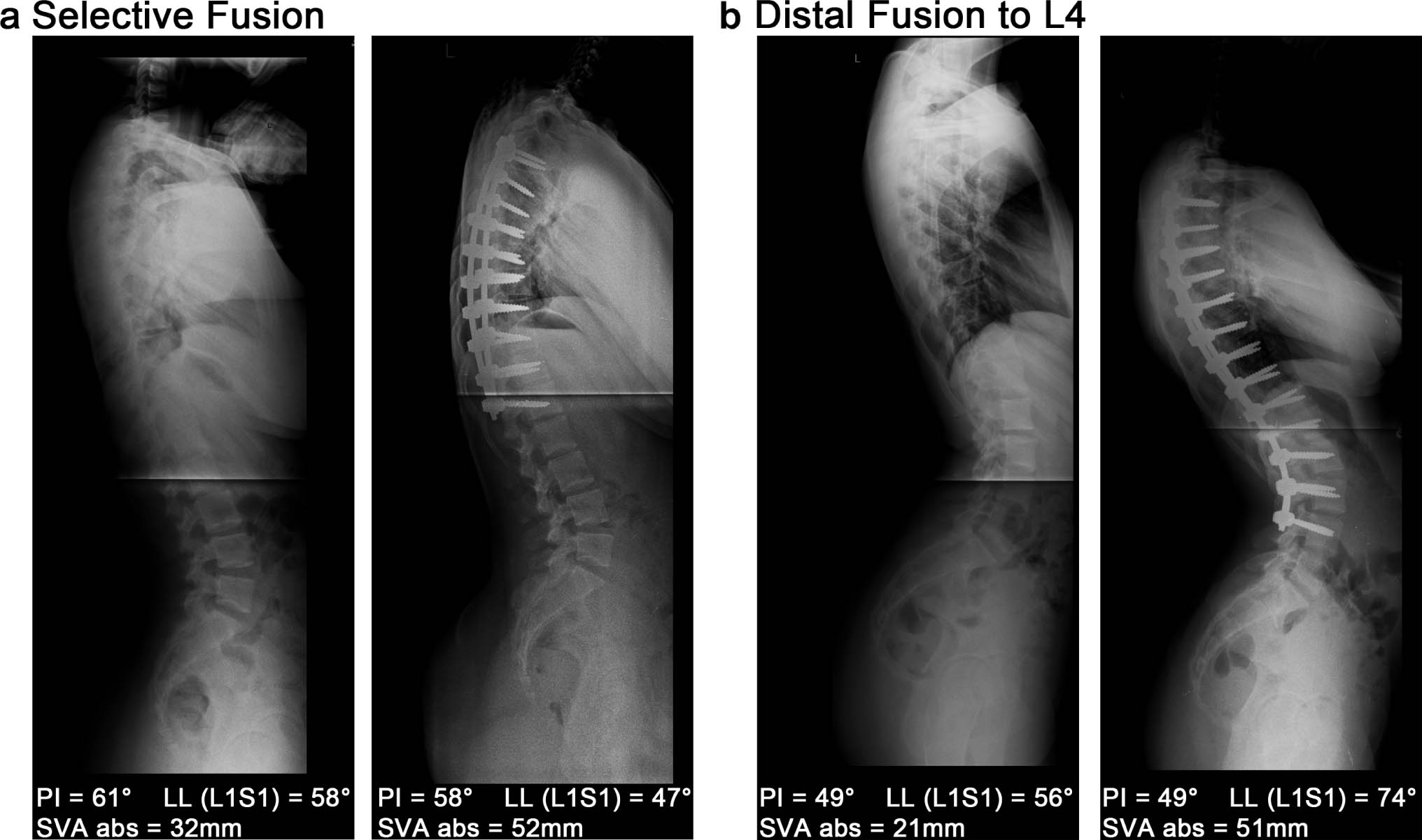
To assess spinal alignment, the relationship of PI and LL (L1–S1) was evaluated by calculating PI–LL, the difference between PI and LL (L1–S1). The increase in LL in the L3–4 fusion group increased the magnitude of PI–LL in this group from –9.1° ± 11.2° pre-operatively to –13.6° ± 14.2° post-operatively (p = 0.015), while PI–LL in the T12–L2 fusion group did not significantly change (p = 0.310). These changes in the L3–4 fusion group generated a PI–LL mismatch (PI–LL of more than ±9°), following the previously proposed clinically relevant formula LL = PI ± 9°. 8 In addition, PI–LL between the two groups was statistically significant different at last follow-up with –4.9° ± 10.2° in the short fusion group and –13.6° ± 14.2° in the L3–4 fusion group (p = 0.002). Fig. 2 shows representative radiographs and spinopelvic measurements of patients in the T12–L2 fusion and L3–4 fusion group before and after PSFI.
Spinopelvic changes in a patient with a selective fusion
LL of segments L4–S1 and PT were similar between groups pre-operatively and did not change after PSFI (Table 2). In addition, no significant pre- to post-operative changes were observed in either surgical group after PSFI (Table 2). SS was similar between groups pre-operatively (p = 0.207) but increased in the L3–4 fusion group after PSFI (pre 42.7° ± 10.5° versus post 45.4° ± 9.7°, p<0.005) and the pre- to post-operative change in SS between groups was statistically significant different (Δ SS: T12–L2 fusion –1.0° ± 5.0° versus L3–4 fusion 1.4° ± 5.9°, p < 0.005).
Sagittal vertical alignment (SVA)
C7 SVA remained stable in in both surgical groups (Table 2). For all patients, mean pre-operative C7 SVA was –17 mm ± 37 and mean post-operative C7 SVA –20 mm ± 35 (p = 0.577).
Proximal junctional kyphosis (PJK)
In this study, PJK was defined as a kyphotic angle > 10° between the upper instrumented vertebra (UIV) and UIV+2 levels and a kyphotic change of the same segment of > 10° pre-operatively to most recent follow-up.31,32 Seven AIS patients developed PJK (proximal junctional angle 21° ± 7°) after PSFI at most recent follow-up. All patients with PJK underwent a L3–4 fusion (7/52, 13.5%), none of the patients in the T12–L2 fusion group developed PJK. Patients with PJK had UIV at T2 (n = 1), T3 (n = 1), T4 (n = 1), T9 (n = 2), and T10 (n = 2) and included Lenke type 1C (n = 3), 5C (n = 3) and 6C (n = 1). Demographic and surgical parameters were similar between patients with PJK and those without (Table 3).
PJK versus noPJK – spinopelvic parameters
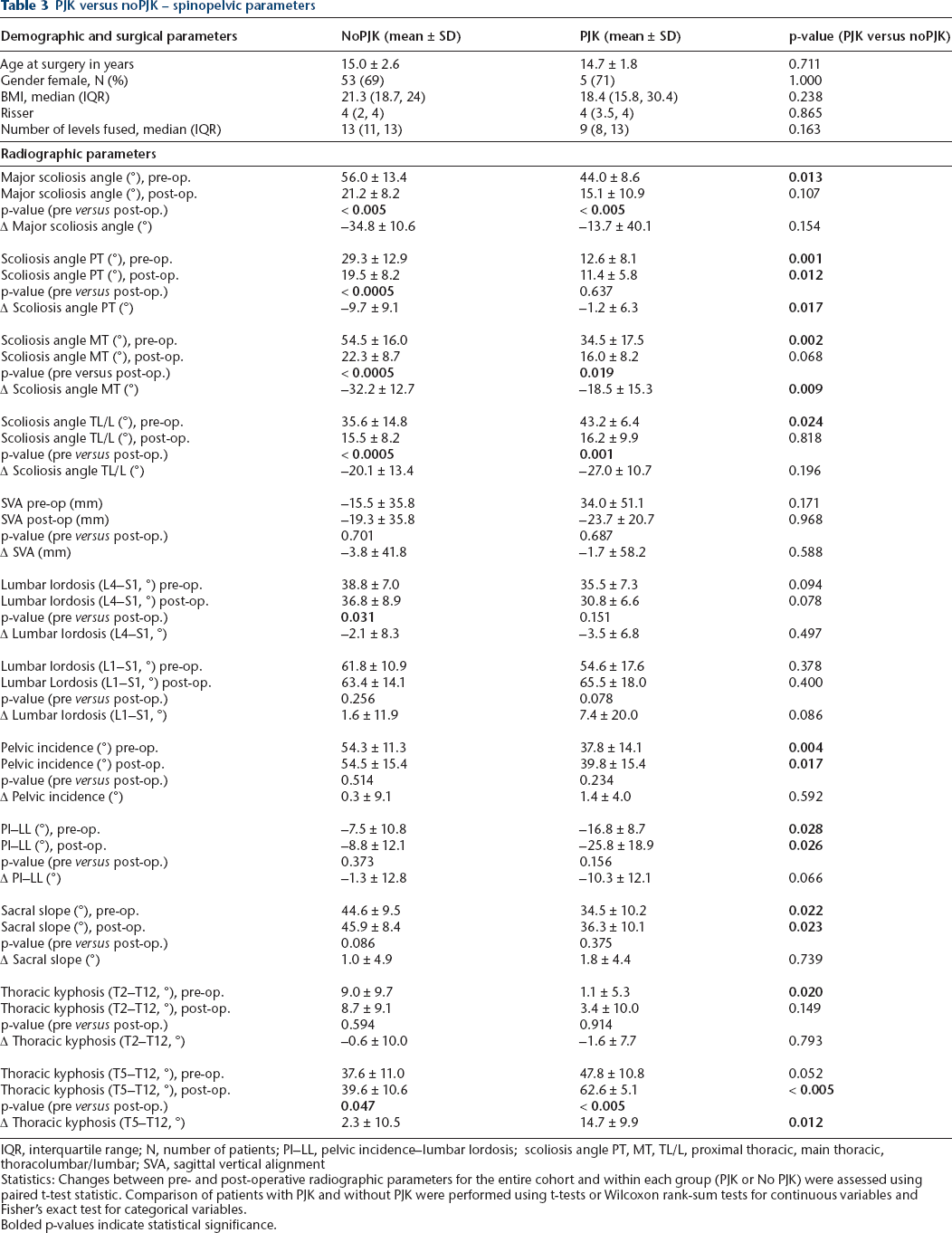
IQR, interquartile range; N, number of patients; PI–LL, pelvic incidence–lumbar lordosis; scoliosis angle PT, MT, TL/L, proximal thoracic, main thoracic, thoracolumbar/lumbar; SVA, sagittal vertical alignment
Statistics: Changes between pre- and post-operative radiographic parameters for the entire cohort and within each group (PJK or No PJK) were assessed using paired t-test statistic. Comparison of patients with PJK and without PJK were performed using t-tests or Wilcoxon rank-sum tests for continuous variables and Fisher's exact test for categorical variables.
Bolded p-values indicate statistical significance.
We compared spinopelvic parameters of patients who developed PJK to those who did not (group ‘noPJK’). Of the surgically alterable parameters, we found that post-operative TK (T2–T12) was significantly larger in patients who developed PJK compared to those who did not (post-operative TK: noPJK 39.6° ± 10.6° versus PJK 62.6° ± 5.1°, p < 0.005). In addition, PJK patients had a significantly greater pre- to post-operative increase in TK (Δ TK: PJK 14.7° ± 9.9° versus noPJK 2.3° ± 10.5°, p = 0.012). Patients with PJK also had a significantly larger post-operative PI–LL mismatch compared to those with noPJK (post-operative PI–LL: noPJK –8.8° ± 12.1° versus PJK –25.8° ± 18.9°, p = 0.026). Post-operative scoliosis angle (noPJK 21.2° ± 8.2° versus PJK 15.1° ± 10.9°, p = 0.107) or SVA (noPJK –19.3° ± 35.8° versus PJK –23.7° ± 20.7°, p = 0.968) were similar between both groups.
Discussion
Proper alignment of the spine and pelvis, including appropriate physiologic sagittal curves, is crucial for the efficient and painless maintenance of an erect posture and sagittal balance. Previous studies have reported differences in sagittal alignment and spinopelvic parameters in early onset scoliosis and AIS patients before spine surgery compared to healthy children.33,34 Surgical correction with PSFI seeks to correct postural imbalances in coronal and sagittal planes, as these are related to poor functional balance in AIS 35 and in adolescents and adults a relationship between spinopelvic parameters and health-related quality of life was shown.11,12,36 Pre-operative planning for deformity correction therefore requires an understanding of spinopelvic parameters in order to minimize degenerative changes in the long term.37,38
In this study we compared sagittal alignment and spinopelvic parameters in 84 AIS patients who underwent fusions to T12–L2 or L3–4. Pre-operatively, pelvic parameters were similar between thoracic and thoracolumbar/lumbar curve types, similar to previously reported data.2,39 Patients with a T12–L2 fusion only demonstrated decrease in scoliosis angle and in TK (T5–T12), whereas patients undergoing a L3–4 fusion had significant changes with regards to scoliosis angle, TK (T2–T12), SS, and LL (L1–S1). Thus, there was increased alteration of spinopelvic parameters when fusions extended distal to L2.
Reports on spinopelvic parameter changes after T12–L2 or more distal fusions in AIS patients are conflicting. Abelin-Genevois et al evaluated PI, SS and LL among 24 AIS patients with fusion to L1 or L2 and 21 patients with a distal fusion to L3 or L4 and found a significant decrease in LL of 4° only in patients with L1–2 fusion at minimum of two-year follow-up. 38 Similarly, Ries et al reported a significant pre- to post-operative decrease of LL by 7° in 50 AIS patients with Lenke 1 and 2 curves who underwent thoracic fusion (LIV T11–L1) and also reported a decrease in TK (T5–T12) by 15°, but no change in SVA, PI or PT in this cohort. 30 In our T12–L2 fusion group, LL and TK (T5–T12) also decreased pre- to post-operatively, though the decrease of LL by 3° was not statistically significant, similar to other reports. These minor changes in the T12–L2 fusion group are not likely to be clinically significant and may also be within measurement error, as a measurement error of less than 5° has been previously reported for scoliosis angle (Cobb method) but not for sagittal radiographic parameters. 40
For distal fusions, Xu et al reported a significant pre- to post-operative increase for TK T5–T12, SS, and LL (T12–S1), and no significant changes in PI, PT or SVA in 36 AIS patients with thoracolumbar/lumbar Lenke 5 curves and PSFI to L3-5 at 2.3-year follow-up, 27 similar to our study. This is in contrast to a report by Yang et al, which showed no change in LL (L1–S1) in 48 AIS patients with Lenke 5 curves and PSFI to L3–5 at 1.8-year follow-up, but showed a significant increase in PT and TK (T1–L1), as well as a decrease in SS. 41 These discrepancies among studies might be due to small sample sizes, different follow-up times, and centre/surgery-specific factors.
In accordance with the previously established relationship of pelvic incidence and lumbar lordosis, the difference ∆PI–LL was calculated. In our cohort, patients in the L3–4 fusion group were significantly more lordotic than patients in the T12–L2 fusion group at last follow-up, as LL (L1–S1) increased in the L3–4 fusion group after PSFI but remained unchanged in the T12–L2 fusion group. This significant increase in lordosis imposed by the PSFI created a PI–LL mismatch in L3–4 fusion patients that is outside of the acceptable range of ±9°. In contrast patients who underwent T12–L2 fusion, PI–LL alignment was maintained since the LL was not significantly altered by the fusion. We believe the PI–LL mismatch happened from hyperlordosis generated by the surgeons in the OR, who in an effort to avoid hypolordosis, overcorrected and increased the LL significantly.
PSFI imposes a fixed lordosis within the fusion so it is believed that LL below the fusion might be altered to compensate and maintain overall pelvic alignment. The L4–S1 segment is a hypermobile segment that comprises the majority of the lordosis of the spine, however in our cohort, the LL of L4–S1 did not change significantly and did not compensate for the hyperlordotic fused segments in the L3–4 fusion group. This lack of change over short-term follow-up however does not rule out the possibility that changes can occur with aging and lead to long-term back pain and disability. Differences in ∆PI–LL likely have consequences on the load patterns in the lumbar spine and even more so in the adjacent segment after spinal fusions.42–45
The overall incidence of PJK in AIS patients after PSFI is in the range of 7% to 11%, 46 similar to our cohort, in which 7/84 patients developed PJK (8.3%). Previously, higher body mass index (BMI), male gender, number of fused levels, choice of UIV and fusion below L2 have been described as risk factors for PJK.47–49 While none of the demographic parameters were associated with PJK in our study and UIV levels were spread over the thoracic spine in patients with PJK, all patients with PJK had a fusion below L2 and their CSVL did not touch the apical lumbar vertebrae pre-operatively (Lenke lumbar modifier C). In our study Lenke 5 and 6 curves had a higher incidence of PJK (Lenke 5: 27%, Lenke 6: 33% versus Lenke 1: 8.1%, Lenke 2–4: 0%), similar to other reports.46,50 A risk factor for PJK that has been consistently reported in AIS and EOS is pre-operative thoracic hyperkyphosis,46,48,51,52 and a critical pre-operative TK > 50° has been identified. 52 Similarly to this, our PJK patients had greater pre-operative TK (PJK 48° versus noPJK 38°; p = 0.052). At follow-up, TK increased even more in PJK patients (pre-op 48° versus post-op 63°; p < 0.005) and put TK out of the reported norm range of 20°–50°. 53 In addition, LL increased in the PJK group post-operatively, although not statistically significant, to keep a balanced spine (pre-op 55° versus post-op 66°; p = 0.078). Although Wang et al reported greater Scoliosis curve correction to be associated with PJK, 49 we and others did not observe this. 54 Patients with PJK had smaller PI and larger PI–LL mismatch after surgery compared to the noPJK group. Yang et al suggested that a smaller PI implied poor capacity for pelvic compensation to sagittal imbalance and proposed that a critical PI for compensation was greater than 39°, 41 which is close to the pre- and post-operative PI seen in PJK patients within our cohort, 37.8° and 39.8°, respectively. Patients suffering from PJK also had larger PI–LL mismatch.
These findings alert the spine surgeon to avoid PI–LL mismatch in an effort to avoid PJK in the future. Particular attention should be paid to the sagittal plane when fusions extend to L3 or L4. Previous studies found that of all radiographic parameters, PI–LL mismatch correlates with pain and disability. In adults, it has been shown that hypolordosis leads to increased magnitude of this mismatch, 45 while in our study in adolescents, hyperlordosis in L3–4 fusions similarly led to increased magnitude of the mismatch.
There are several limitations associated with this study. First, it is retrospective in nature. Second, this study is based on radiographical outcomes, which are subject to inconsistencies in positioning, technician experience, and measurement reliability. It has also been reported that 2D radiographic sagittal measures are not completely accurate and 3D modelling would give more accurate measurements.29,39 Also, we did not further explore changes in cervical sagittal parameters after PSFI. 55 Third, multiple surgeons performed PSFI, however, given the number of patients in this study, we were unable to tease out the contribution of each surgeon. Quality of life outcome scores were not included in this report but will be explored in the future. The long-term quality of life implications of these changes have yet to be clarified in this patient population.
Conclusion
The goal of the scoliosis surgeon in the sagittal plane is to obtain an appropriate amount of LL with the PSFI that will allow the spinal alignment to be harmonious. In this patient series, LL increased with L3–4 fusion and increased LL altered the PI–LL relationship, putting this group outside the acceptable range for adults. While our overall incidence of PJK was similar to previously reported papers, all of the cases occurred in the L3–4 fusion group and these patients tended to have smaller PI and greater PI–LL mismatch. Surgeons should attempt to maintain normal LL in AIS patients when performing nonselective fusions to avoid alterations in PI–LL that could create difficulties for patients as they age. Pre-operative estimation of pelvic morphology, specifically PI, should be used to calculate and achieve the optimal amount of lordosis via rod bending and patient positioning. Special attention should be paid to patients with a PI less than or equal to 39° undergoing a fusion ending at or below L3. Intraoperative radiographs may be used to evaluate congruency between LL and PI after surgical correction.