
Abstract
Abstract
Purpose
Scoliosis, chest wall deformities and pulmonary involvement are common features of Marfan syndrome (MFS). We aimed to assess the impact of spinal and chest wall deformities on pulmonary function in paediatric MFS patients with a surgically managed spinal deformity.
Methods
In this multicentre retrospective study, spirometry, lung volumes and radiographic imaging were performed on 26 MFS patients between the ages of seven and 18 years who were undergoing planned spinal fusion surgery for spinal deformity. A correlation analysis assessed the relationship between radiographic measurements of spinal and chest wall deformities and predicted total lung capacity (TLC), forced vital capacity (FVC) and the ratio between forced expiratory volume in one second and FVC (FEV1/FVC).
Results
In total, 18 patients (70%) had impaired pulmonary function. Thoracic kyphosis (mean 19.3°; -32° to 54°) had a strong positive correlation with FEV1/FVC (r = 0.65; p < 0.001). Significant decrease in FEV1/FVC below 80% occurred at kyphosis under 15° (p = 0.004). Kyphosis had a moderate negative correlation with FVC (r = -0.43; p = 0.03). Chest wall deformity had a strong negative correlation with FEV1/FVC (r = -0.61; p = 0.001). The magnitude of the thoracic curve (mean 55.2°; 28° to 92°) had a significant moderate negative correlation with TLC (r = -0.45; p = 0.04).
Conclusion
In MFS, three factors correlate with decreased pulmonary function measures: hypokyphosis, increasing chest wall deformity and increasing coronal curve magnitude. Hypokyphosis and increased chest wall deformity correlated with diminished FEV1/FVC; increasing thoracic spinal curvature with diminished TLC. Further analysis with a larger cohort will help better define the relationship between these deformities and pulmonary function in this unique population.
Level of Evidence
IV
Introduction
Marfan syndrome (MFS) is a connective tissue disorder with an estimated incidence of two to six persons per 100 000. 1 It is caused by mutations in the gene Fibrillin-1 (FBN1) on chromosome 15 that encodes the FBN1 protein, which is an essential part of the connective tissue of the cardiovascular and musculoskeletal systems. MFS is usually an autosomal dominant disorder, however, sporadic mutation is evident in up to 25% of cases.
Though a typical phenotype does exist for MFS, the clinical expression is broad and may differ even among members of the same family. The syndrome involves several body systems, most importantly the cardiovascular, ocular and skeletal systems.2,3 MFS’ effect on the skeletal system includes arachnodactyly, dolichostenomelia, generalized ligamentous laxity and chest, spine, pelvic and foot deformities.
A deformity of the thoracic cage (pectus carinatum or excavatum) and scoliosis are among the most common features of MFS and exist to some degree in approximately 60% of the patients.4–6 Pulmonary involvement in MFS can be found in approximately 63% of the patients. It may consist of restrictive or obstructive disease and occurs due to skeletal deformities or possible an abnormal lung parenchyma.7–11
Previous studies have identified the relationship between the magnitude and shape of a scoliotic curve and pulmonary function in patients with adolescent idiopathic scoliosis.12–17 Additionally, the effect of chest wall deformities on pulmonary function has been described.18–20 There are few studies regarding pulmonary function in MFS, and the relationship between spinal or thoracic chest deformity and pulmonary function has not been well studied. The aim of this study was to determine the effect of scoliosis, kyphosis and chest wall deformity on the pulmonary function of pediatric patients with MFS.
Materials and methods
Patients
This study is a multicentre collaboration between two high volume paediatric orthopaedic departments. Institutional review board approval from both centres was obtained and a retrospective database search was performed identifying all patients with a diagnosis of MFS who had undergone spinal surgical intervention between the years 2000 and 2018. The diagnosis of MFS was made according to the revised Ghent nosology. 21 Patients were excluded if they were > 21 years old at the time of surgery or if either radiographs or pulmonary function tests (PFT) prior to surgery were not available.
Spinal radiographic parameters
Preoperative radiographs were evaluated for scoliosis, thoracic kyphosis and chest wall deformity. Thoracic scoliosis and kyphosis were measured by a single trained observer (HO) who was not involved in the care of the patients using validated software for spinal measurements (Surgimap, Nemaris Inc., New York, New York). 22 If two curves were present, the larger thoracic curve was used for the purpose of the study. Thoracic kyphosis was measured from the superior endplate of T5 to the inferior endplate of T12. Chest wall deformity was assessed using the sterno-vertebral (SV) ratio; this describes the ratio of the lateral width of the vertebral body at the level of the maximum SV distance in the midthoracic region, multiplied by 100. This number is divided by the distance between the posterior cortex of the sternum and the anterior cortex of the vertebral body at the same level. This ratio minimizes differences caused by patient size or radiograph magnification (Fig. 1).15,23
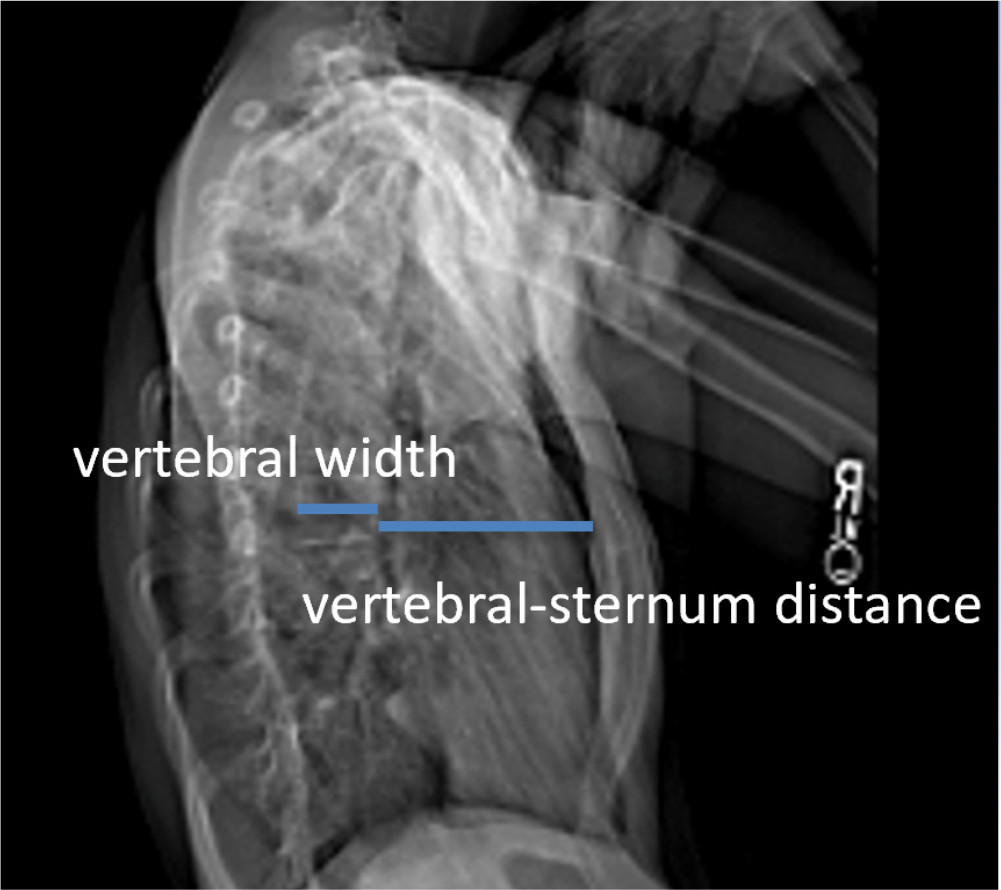
The sterno-vertebral (SV) ratio describes the ratio of the lateral width of the vertebral body at the level of the maximum SV distance in the midthoracic region, multiplied by 100. This number is divided by the distance between the posterior cortex of the sternum and the anterior cortex of the vertebral body at the same level.
PFTs
All patients underwent PFTs prior to surgery according to American Thoracic Society and European Respiratory Society guidelines. 24 Spirometry and lung volumes were used to measure vital capacity (VC), total lung capacity (TLC), forced VC (FVC) and forced expiratory volume in one second (FEV1). A TLC and FVC ≥ 80% of the predicted value and a FEV1/FVC of ≥ 80% of the predicted value were considered normal.24,25 Interpretation of the PFT was based on established reference values available during the years of this study but in some instances varied from site to site.
Statistical analysis
The SPSS software (IBM, Chicago, Illinois) was used to analyze the correlation between the PFT results and the preoperative radiographic measurements (Cobb magnitude of the coronal plane thoracic curve, the sagittal plane Cobb angle between T5 and T12 and the SV ratio). Due to our limited sample size (26 patients) we used nonparametric statistical tests. Relationships between the variables were analyzed using Spearman's rank correlation with a two-tailed test of significance. Quantitative variables were compared using the Mann-Whitney U test. Multiple regression analysis was not performed because of the small sample size. Statistical significance was defined as a p-value of < 0.05.
Results
In all, 35 MFS patients treated with spinal fusion between the years 2000 and 2018 were identified in a database search of both centres. Nine patients were excluded due to unavailable radiographs or PFTs. For the remaining 26 patients (13 female), the mean age at surgery was 13.8 years (7 to 18) and preoperative radiographs and PFT were reviewed (Table 1 and 2, respectively). One patient was missing a lateral radiograph and several patients had incomplete PFT data; in most of these cases lung volumes were not performed. Additionally, the spirometry data for patient 9 and the lung volume data for patient 20 were excluded from the statistical analysis because of the inability to perform these tests in a reproducible manner.
Spinal curvatures and chest wall deformity characteristics
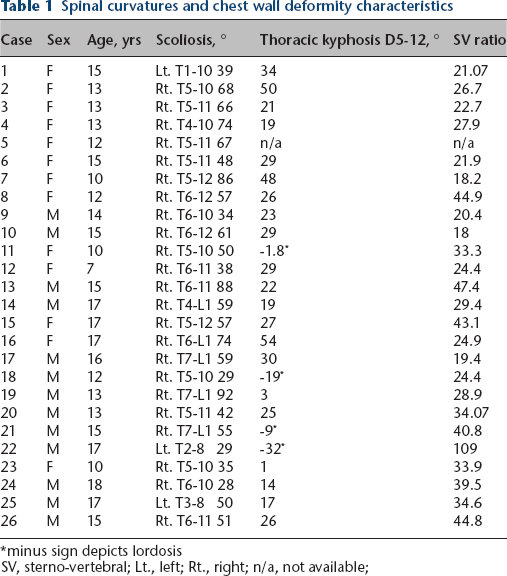
minus sign depicts lordosis
SV, sterno-vertebral; Lt., left; Rt., right; n/a, not available;
Pulmonary functional test measurements
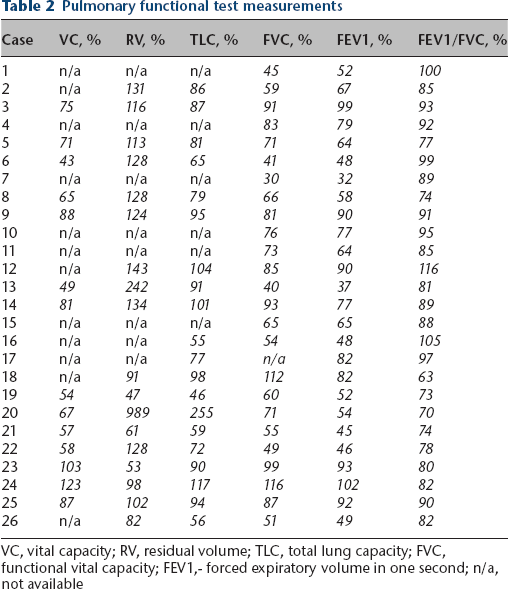
VC, vital capacity; RV, residual volume; TLC, total lung capacity; FVC, functional vital capacity; FEV1,- forced expiratory volume in one second; n/a, not available
Thoracic kyphosis
The mean thoracic kyphosis measured as the Cobb angle between T5 and T12 was 19.3° (-32° to 54°). The negative values depict a reversal of the natural kyphotic thoracic spine into a lordotic angle. The thoracic kyphosis had a strong positive correlation (Table 3) with FEV1/FVC (n = 25; r = 0.65; p < 0.001). A significant decrease in FEV1/FVC below 80% occurred at kyphosis under 15° (p < 0.005) (Fig. 2). Additionally, the degree of kyphosis had a moderate negative correlation with FVC (n = 24; r = -0.43; p = 0.03) and moderate positive correlation with the residual volume (RV) (n = 16; r = 0.55; p = 0.02). No significant correlation was found between the thoracic kyphosis and FEV1 (n = 24; r = -0.18; p = 0.39).
Correlation of spinal deformities with pulmonary function tests
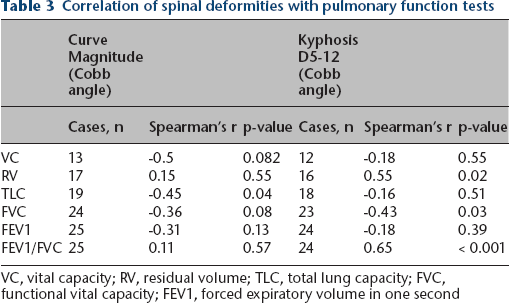
VC, vital capacity; RV, residual volume; TLC, total lung capacity; FVC, functional vital capacity; FEV1, forced expiratory volume in one second
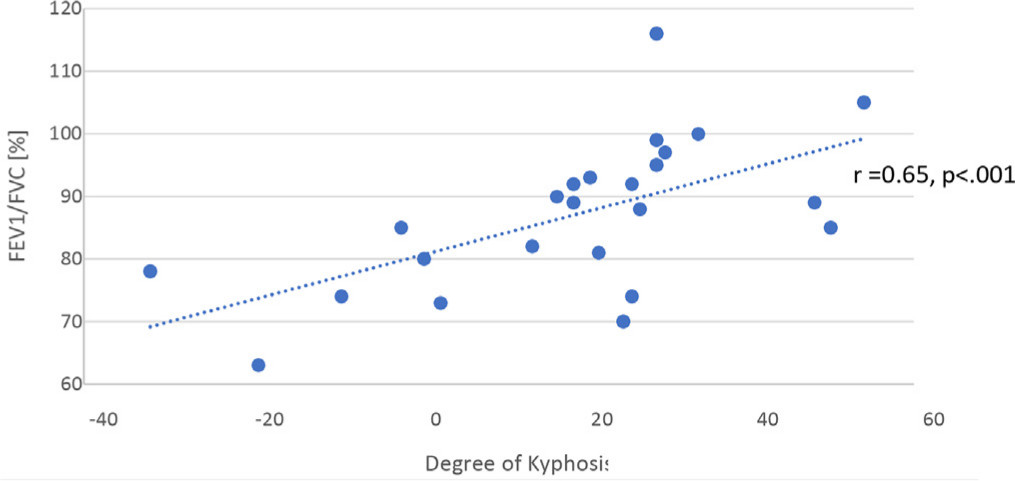
Correlation between the ratio of forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) and the degree of kyphosis. The decrease in FEV1/FVC with kyphosis < 15° was statistically significant (p = 0.004).
Thoracic coronal curve
The mean thoracic curve was 55.2° (28° to 92°). The magnitude of the thoracic curve had a significant moderate negative correlation (Table 3) with TLC (n = 19; r = -0.45; p = 0.04). A significant decrease in TLC below 80% occurred at 40° (p = 0.02) (Fig. 3). No other significant correlation was found between the coronal curve magnitude and the PFT.
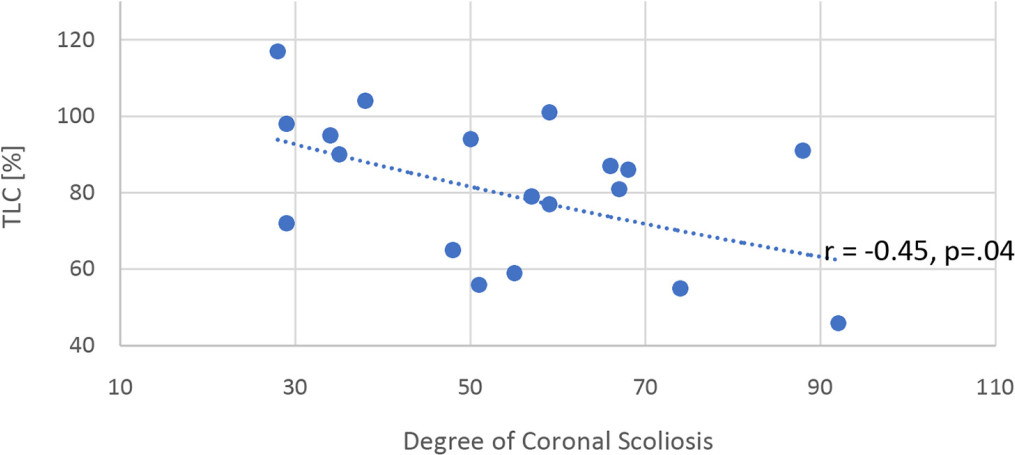
Correlation between total lung capacity (TLC) and the degree of the coronal curve. The decrease in TLC in patients with > 40° coronal curve was statistically significant (p = 0.02).
Chest wall deformity
Examination of the SV ratio revealed a mean ratio of 33.3 (18 to 109). It had a strong negative correlation (Table 4) with FEV1/FVC (n = 24; r = -0.61; p = 0.001) (Fig. 4). No other significant correlations were found between the SV ratio and the other PFT measurements.
Correlation of sterno-vertebral ratio and pulmonary function tests
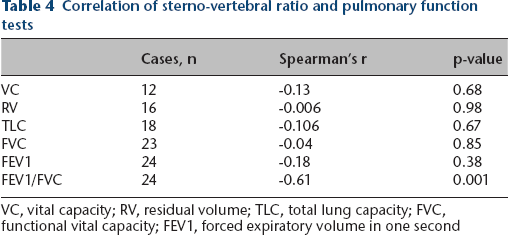
VC, vital capacity; RV, residual volume; TLC, total lung capacity; FVC, functional vital capacity; FEV1, forced expiratory volume in one second
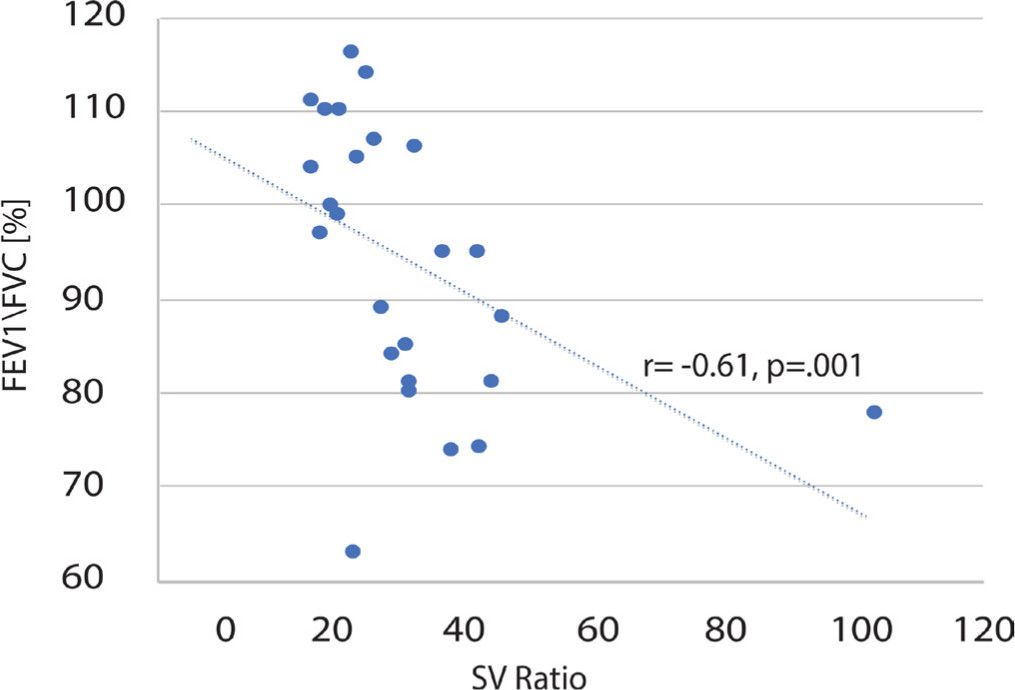
Correlation between the ratio of forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) and the SV (sterno-vertebral) ratio.
Discussion
A well-known association has been established between spinal deformity and pulmonary function. Numerous studies in the adolescent idiopathic scoliosis population have found a correlation between increasing thoracic scoliosis and hypokyphosis with pulmonary impairment.12–17 Similar associations have been found in more unique populations such as osteogenesis imperfecta and arthrogryposis multiplex congenital.23,26–28 Both a restrictive and an obstructive pulmonary pattern have been described in populations with spinal deformity. The restrictive findings can be attributed to decreased chest wall compliance, decreased rib excursion, possible decreased respiratory strength and the effect of placing the diaphragm at a mechanical disadvantage for inspiration and expiration. It has been suggested that obstructive lung disease could be secondary to increased airway smooth muscle tone, asthma variant, lower airway malacia or intrathoracic airway compression due to chest wall deformity. Recently, the 3D effect of scoliosis on the tracheobronchial tree has been demonstrated by using chest CT reconstruction of the spine and airway. 29 In this study bronchial compression correlated with reduction in FEV1/FVC, and it was most strongly associated with the loss of kyphosis. This would explain why some patients have mixed ventilatory findings on their pulmonary function, i.e. restriction and obstruction.
Not infrequently, patients with spinal deformities may have concomitant pectus deformities. PFTs in children with pectus excavatum has shown normal lung function as well as restrictive and obstructive disease.30,31 Though the presence of scoliosis in these studies did not seem to have a statistically significant effect on lung function, patients with more severe pectus deformity seem to be more likely to have scoliosis.
Murine models of MFS have demonstrated impaired lung development characterized by enlarged alveolar air spaces, reduced alveolar septation and increased lung compliance.32–34 The most comprehensive study of the microscopic findings of the human lung with MFS has found a pattern of distal acinar emphysema. 10
Clinical studies involving large numbers of individuals with MFS are few. In a retrospective analysis of PFTs in 69 patients, 30 had scoliosis, 15 had pectus excavatum and 21 had both skeletal deformities. 7 This study used sitting height, a measure that more accurately reflects the length of the thorax, in order to avoid the inappropriate use of predicted values based on standing height. In other words, standing height in this population would underestimate the true value of the lung function data obtained by spirometry and lung volumes. This study revealed that only patients with moderate to severe pectus excavatum or scoliosis had reductions in the FVC and FEV1, diagnostic for restrictive lung disease; TLC was reduced in patients with pectus excavatum. Important to note is the fact that the severity of the chest wall deformity was judged only by inspection of the external appearance and not by examining patient's imaging.
In our study of 26 MFS patients we identified 70% of the patients having some form of pulmonary impairment similar to the 63% found in the literature. 11
An increased thoracic lordosis and SV ratio correlated with diminished FEV1/FVC suggestive of obstructive disease (r = 0.65; p < 0.001; and r = -0.61; p = 0.001, accordingly). Both parameters represent the thoracic anteroposterior space, a decrease in which has been demonstrated in the past as limiting the expansion of the thoracic cavity and impairing pulmonary function.30,31 Furthermore, we found a significant decrease in FEV1/FVC below 80% occurring at kyphosis under 15° (p < 0.005) (Fig. 2).
In addition, in our study, there was a positive correlation between increasing RV and increasing degrees of kyphosis. Residual volume is a sensitive measure of air trapping and the data suggest that MFS patients with more severe kyphosis are at an increased risk. Other factors frequently associated with thoracic spine deformities such as costovertebral joint stiffness, sternal deformity, decreased muscular strength or malposition of diaphragmatic insertion into ribs and thoracic vertebral bodies, can adversely affect the movement of the diaphragm and respiratory mechanics contributing to air trapping. This warrants further investigation.
In accordance with previous studies, increased thoracic coronal curve magnitude correlated with diminished TLC (r = -0.45; p = 0.04), suggestive of restrictive disease, with a significant decrease in TLC below 80% occurring at 40° (p = 0.02) (Fig. 3). We did not find any other significant correlation between the curve magnitude and PFT.
To the best of our knowledge this is the first study of MFS correlating the magnitude of the spinal and chest wall deformity with PFT. Consistent with previous studies (not in MFS individuals), we found a significant correlation between increased thoracic lordosis and coronal curve magnitude and diminished pulmonary function. Additionally, we found a significant correlation between increased chest wall deformity (as manifested in the SV ratio) and pulmonary function impairment (Fig. 4).
Several limitations should be noted; the data was retrospective and collected over a period of ten years. Additionally, not all the patients had lung volumes or diffusing capacity for carbon monoxide (DLCO) performed; 40% of the patients had incomplete PFT data, which highlights the challenges in assembling large volume data in these complex patients. Standing height or arm span measurements, rather than sitting height, were used. This will underestimate the true lung function in this population due to the abnormal length of the arms and legs. In addition, the lung function predicted values used for normal reference values could have varied between institutions, and over time, thus introducing another variable in data collection and results. Further analysis with a larger cohort of patients will help better define the true relationship between these deformities and their influence on pulmonary function in MFS.
Footnotes
Dror Ovadia is on the editorial boards of Journal of Children's Orthopaedics, Journal of Pediatric Orthopaedics and European Spine Journal.
The other authors declare that they have no conflict of interest.
RFW: Study design, Interpretation of data, Manuscript revision.
MFDM: Study design, Interpretation of data, Manuscript revision.
DO: Study design, Interpretation of data, Manuscript revision.