
Abstract
Abstract
Purpose
This study investigated the initial angular deformity of proximal tibial metaphyseal fracture in children and its recovery during follow-up according to the cause of injury.
Methods
Prospective data about the patients with a proximal tibial metaphyseal fracture at the age less than six years and available follow-up data at two years post-trauma were retrospectively reviewed. They were grouped into trampoline-related injuries (TRI) and non-TRI groups based on the cause of injury. Proximal tibial valgus and recurvatum angles were measured to assess angular deformity on the coronal and sagittal planes, respectively.
Results
A total of 47 patients (33 TRI and 14 non-TRI) were included. Initially, the valgus angles were -1.5° in TRI and 1.6° in non-TRI groups (p < 0.001) and the recurvatum angles were 7.8° in TRI and 4.1° in non-TRI groups (p = 0.048). After two-year follow-up, the valgus angles were 0.2° in TRI and 0.9° in non-TRI groups (p = 0.070), and the recurvatum angles were 6.5° in TRI and 2.3° in non-TRI groups (p = 0.001).
Conclusion
For children with a proximal tibial metaphyseal fracture, the initial coronal deformity was different according to the injury cause (varus in TRI whereas valgus in non-TRI). Although there was a near complete recovery after approximately two years of follow-up in the coronal deformities, the sagittal deformity (genu recurvatum) seems to recover incompletely or tardily, especially for those caused by TRI.
Level of Evidence
III
Introduction
Proximal tibial metaphyseal fracture was relatively rare in 1980s, but with the recent popularization of trampoline activities, its incidence as one of trampoline-related injuries (TRIs) has increased, especially among children aged under six years.1–6 Some studies have reported that proximal tibial metaphyseal fracture has a risk of post-traumatic valgus deformity.7,8 However, it is currently suggested that the degree of valgus deformity would be minimal or absent in patients with proximal metaphyseal fracture by TRI.2,9 Therefore, this underscores the need to investigate the fractures separately based on the cause of injury (TRI versus non-TRI).
The excessive axial compressive force during landing on the mat is a well-known injury mechanism of TRI.3,10 Several studies on proximal tibial metaphyseal fractures as a type of TRIs have reported characteristic radiological findings that involve the anterior cortex due to axial loading on the hyperextended knee, such as buckling of the anterior apophysis of the tibia and anterior tilt of the proximal tibial epiphyseal plate.9,11,12 Despite reports stating that recurvatum deformity is one of the important features of proximal tibial metaphyseal fracture due to TRI, there has been a paucity of follow-up studies on sagittal deformity, unlike coronal deformity.
Under the hypothesis that the initial presentation and the change of the deformity during the follow-up would be different according to the cause of injury, we investigated the clinico-radiological characteristics of paediatric proximal tibial metaphyseal fractures. During the investigation, the patients were divided into two groups according to the injury cause (TRI versus non-TRI), and the deformities were investigated separately by coronal and sagittal planes.
Patients and methods
Patient selection
This study was approved by the institutional review board of our institute. Since 2015 at our institution we have prospectively acquired data from the patients who are diagnosed with proximal tibial metaphyseal fracture and treated according to our protocol (see next section). The patients in our datasets who registered from 1 January 2015 to 31 December 2017 were retrospectively reviewed. Inclusion criteria were patients being less than six years of age at the time of the diagnosis, having no underlying disease that may affect the musculoskeletal system and being able to walk well before the occurrence of the fracture. Among the 59 children who met the eligibility criteria, those who needed surgical treatment at diagnosis (n = 4), had bilateral tibial fractures whether simultaneously or subsequently (n = 2) and had no available post-traumatic follow-up data taken within three months post-trauma and at around 24 months (21 to 27 months) post-trauma (n = 6) were excluded. Finally, 47 children were included for analysis. Their demographic data are shown in Table 1. Among these patients, there were no patients with open fracture or with neurovascular compromise. They were grouped into TRI and non-TRI groups according to the cause of injury. The patients whose injury occurred not during trampolining (e.g. a patient tripped and fell during climbing up a trampoline) were placed in the non-TRI group.
Demographic data of the children
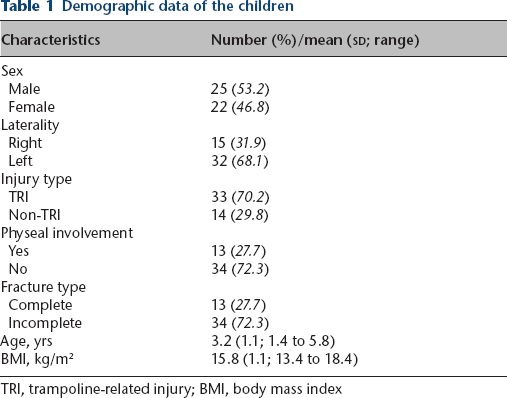
TRI, trampoline-related injury; BMI, body mass index
Treatment and follow-up protocol for the children with proximal tibial metaphyseal fracture
The conservative treatment and follow-up protocol for the patients with a proximal tibial metaphyseal fracture was as follows. At the initial work-up, anteroposterior (AP) and lateral views of simple radiographs for both knees and lower legs were obtained. Comorbid medical conditions were also evaluated. General indications for surgical treatment were as follows: 1) open fracture; 2) fracture with suspicion of neurovascular compromise; and 3) severely displaced fracture even after trial of closed reduction (angulation > 15° to 20° and/or displacement > 50%). If conservative treatment was the clinical option, three to five weeks of immobilization by long leg cast was applied. Subsequently, rehabilitation was begun, and the patients were allowed to gradually return to their previous activity level. After recovery, the patients were followed post-traumatically at three, six, 12 and 24 months. Full-length standing AP radiographs of both lower extremities with the patella facing forward (teleradiograms) and scanograms centred at the hip, knee and ankle with a radiopaque ruler were taken at every visit as well as AP and lateral views of both knees and lower legs.
Radiographic measurements
Simple radiographs of lower legs obtained within three months post-trauma (which were regarded as ‘initial’ radiographs) and at around 24 months post-trauma (between 21 and 27 months post-trauma, which were regarded as ‘last’ radiographs) were used for analysis of angular deformity. To assess coronal deformity, the proximal tibial valgus angle measured by the angle between the proximal tibial physis and tibial shaft on the AP view of lower leg radiographs were used. The measured angles were compared with those of the contralateral uninjured side to indicate ‘valgus angle’. If a patient presented with valgus deformity compared with the contralateral uninjured side, a positive value was assigned. For the young children with ambiguous straight physeal plate, the metaphyseal-diaphyseal angles were used. To assess sagittal deformity, anterior tilt angles of the proximal tibial physis were measured on lateral view of lower leg radiographs. The proximal line of the angle was defined by drawing a tangent between the dorsal- and mid-point of the physis, 13 and the angle between the proximal tibial physis and tibial anterior cortical shaft was measured. The measured angles were compared with those of the contralateral uninjured side to indicate ‘recurvatum angle’. If a patient presented with recurvatum deformity compared with the contralateral uninjured side, a positive value was assigned (Fig. 1). Therefore, four angles (initial valgus, last valgus, initial recurvatum and last recurvatum angles) were measured to evaluate the angular deformity in each participant. To test the interobserver reliability for the assessment of the valgus and recurvatum angles, two observers (JYJ and MSK) performed assessments in 20 randomly selected patients. The interobserver reliabilities of the measurements were evaluated using intraclass correlation coefficients, and those were > 0.8, representing satisfactory agreement. Thus, measurements taken by a single investigator (MSK) were used in the analyses. The leg-length discrepancy (LLD) was measured on the scanograms, which were obtained at around 24 months (21 to 27 months) post-trauma. If the injured leg was longer than the contralateral uninjured side, a positive value was assigned. In addition, the presence of proximal tibial physeal involvement of fracture line and fracture type according to the presence of complete cortical breakage (complete or incomplete) was recorded.
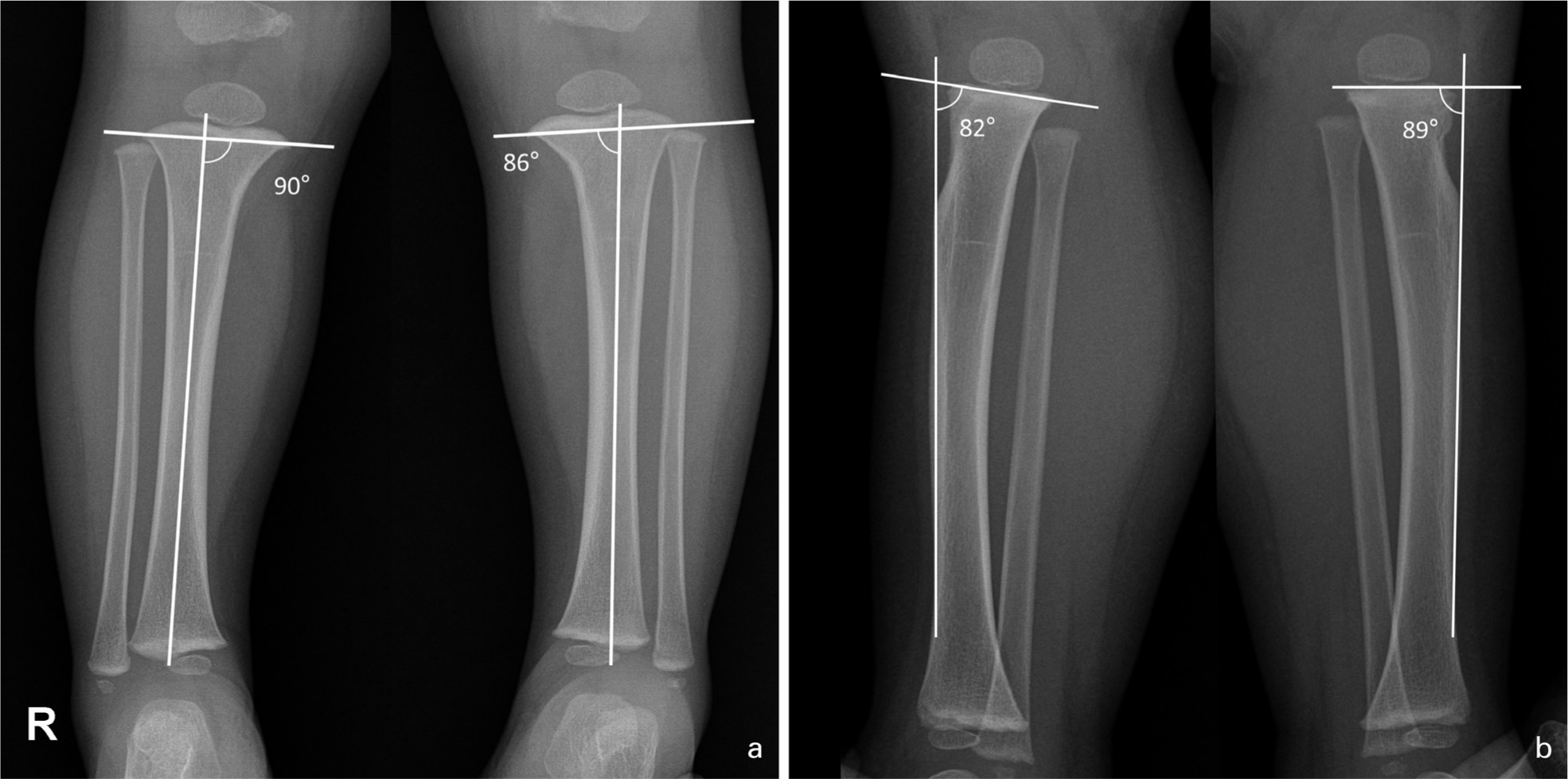
A one-year and ten-month-old boy was diagnosed with a left proximal tibial metaphyseal fracture that occurred after falling on the trampoline. These simple radiographs of both lower legs were taken at the day of trauma, hence, were regarded as ‘initial’ radiographs because they were taken within three months of the post-traumatic period:
Investigated variables
Besides radiographic measurements, demographic data (age, sex, body mass index (BMI)), and presence of any complication during the follow-ups were investigated.
Statistical analysis
The significance of the differences between means was calculated by using the independent t-test. The significance of the differences between frequencies was calculated by using the chi-squared test. The effect of each variable on residual deformity at the final follow-up was analyzed using linear logistic regression analysis. To eliminate confounders among the variables, multivariate analysis (stepwise method) was performed with all the variables to exclude confounders. The p-values that were < 0.05 were considered to indicate statistical significance. All statistical analyses were performed using the SPSS software (version 21; IBM Co., Armonk, New York).
Results
None among the included patients underwent surgery or showed any significant complications such as nonunion, limit of movement and neurovascular problems during the follow-up period. At the final follow-up, there were no subjective complaints from the patients and their parents of any gross deformity. There was no subjective discomfort of the patients or their parents even when the knee was hyperextended on physical examination.
Comparisons between the TRI and non-TRI groups
The comparisons between the TRI and non-TRI groups are presented in Table 2. Initially, although the non-TRI group presented with valgus deformity, the TRI group presented with varus deformity (mean initial valgus angle −1.5° (sd 2.0°) (TRI) versus 1.6° (sd 1.7°) (non-TRI); p < 0.001) and more recurvatum deformity than the non-TRI group (mean initial recurvatum angle 7.8° (sd 3.0°) (TRI) versus 4.1° (sd 6.1°) (non-TRI); p = 0.048). After around two years of follow-up, both groups presented nearly a complete recovery of their coronal deformities (mean last valgus angle 0.2° (sd 1.2°) (TRI) versus 0.9° (sd 0.9°) (non-TRI); p = 0.070), but their sagittal deformity remained, especially for those in the TRI group (mean last recurvatum angle 6.5° (sd 3.6°) (TRI) versus 2.3° (sd 3.6°) (non-TRI); p = 0.001) (Fig. 2).
Comparisons between the trampoline-related injury (TRI) and non-TRI groups
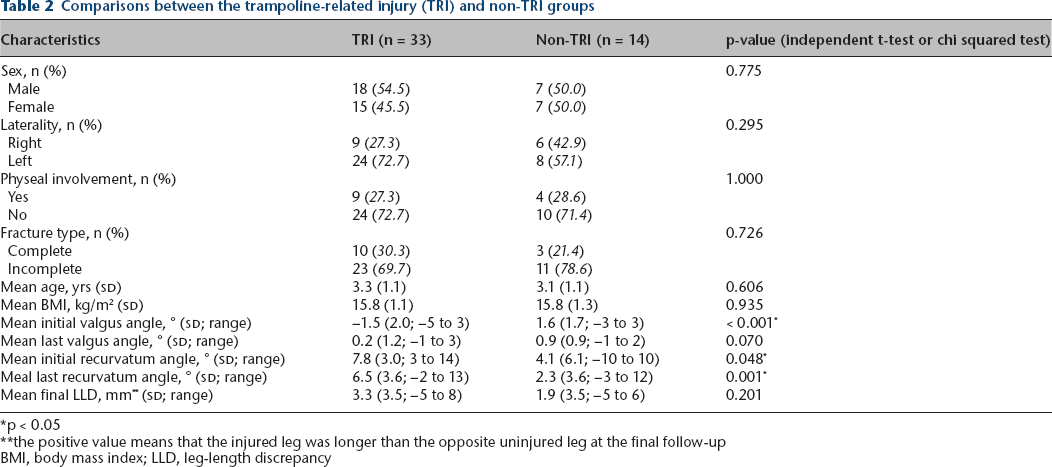
p < 0.05
the positive value means that the injured leg was longer than the opposite uninjured leg at the final follow-up
BMI, body mass index; LLD, leg-length discrepancy
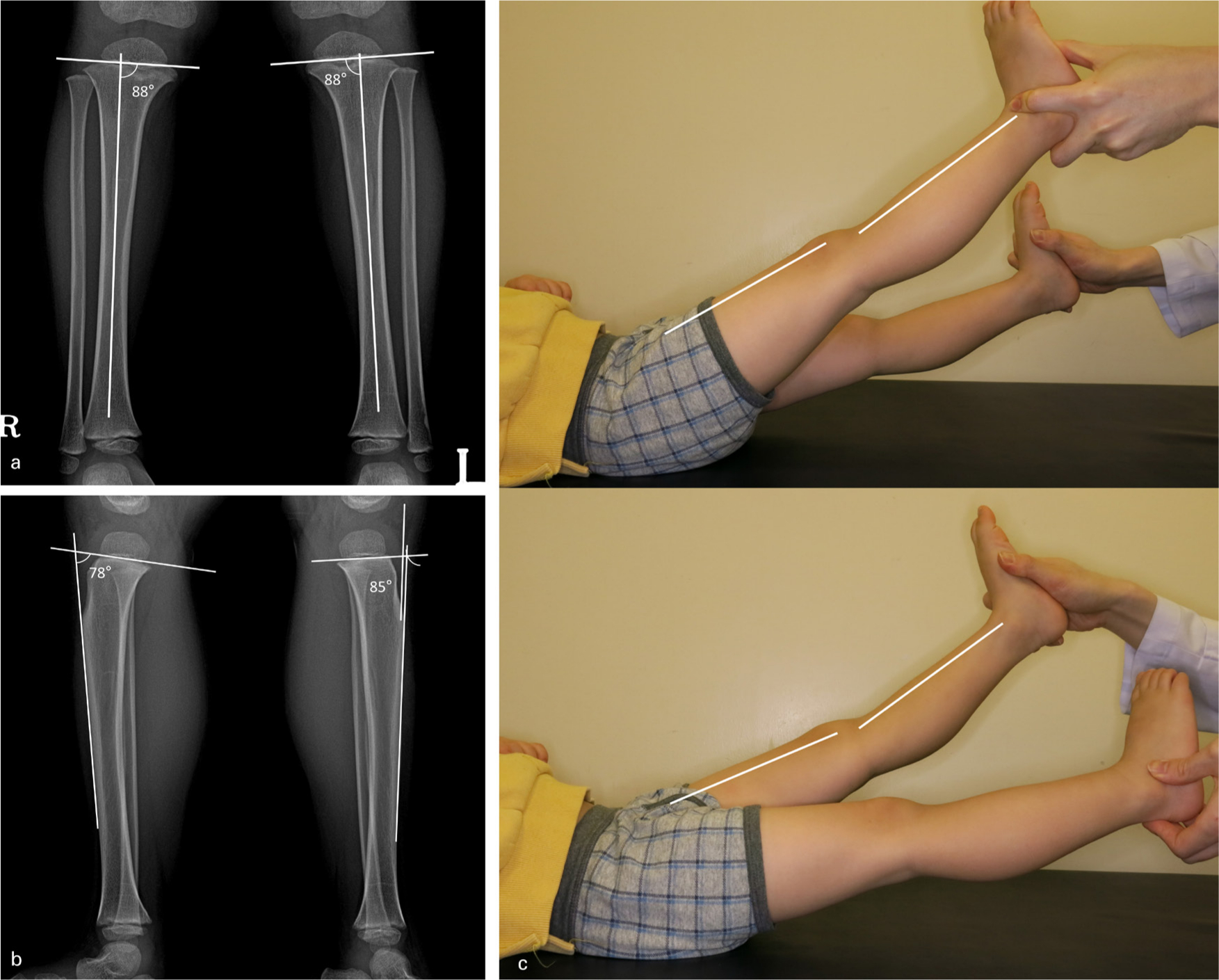
A one-year and ten-month-old boy was diagnosed to have a left proximal tibial metaphyseal fracture for his pain that occurred after falling on the trampoline (the same patient presented in the Fig. 1). Simple radiographs were taken at two years and two months post-trauma and, therefore, were regarded as ‘last radiographs’:
Predisposing factors for residual angular deformity
The univariate and multivariate results of linear logistic regression analysis on the residual valgus and recurvatum deformities at the final follow-up are presented in Tables 3 and 4. The initial valgus angle and BMI were significant predisposing factors for residual valgus angle at the final follow-up (Table 3). Male sex, an injury type of TRI and a large initial recurvatum angle were significant predisposing factors for incomplete recovery of recurvatum deformity (Table 4).
The results of linear regression analyses of predisposing factors for residual valgus deformity at the final follow-up
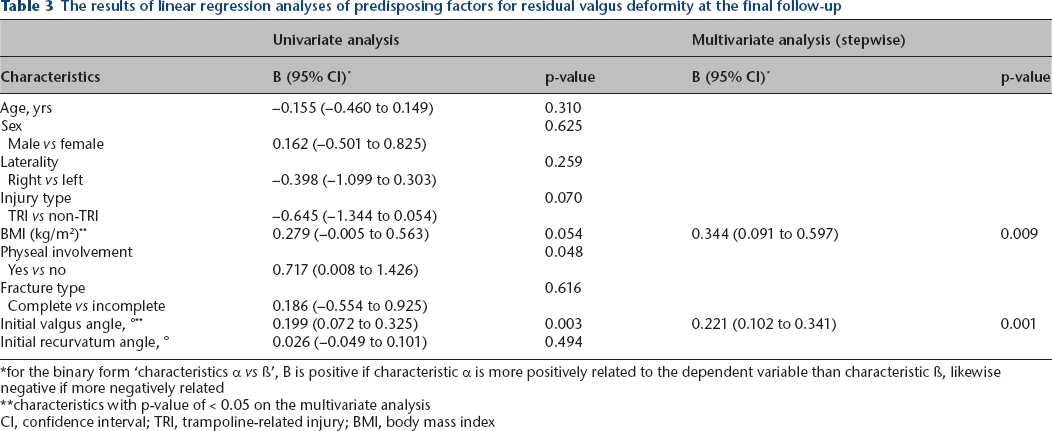
for the binary form ‘characteristics α vs ß’, B is positive if characteristic α is more positively related to the dependent variable than characteristic ß, likewise negative if more negatively related
characteristics with p-value of < 0.05 on the multivariate analysis
CI, confidence interval; TRI, trampoline-related injury; BMI, body mass index
The results of linear regression analyses of predisposing factors for residual recurvatum deformity at the final follow-up
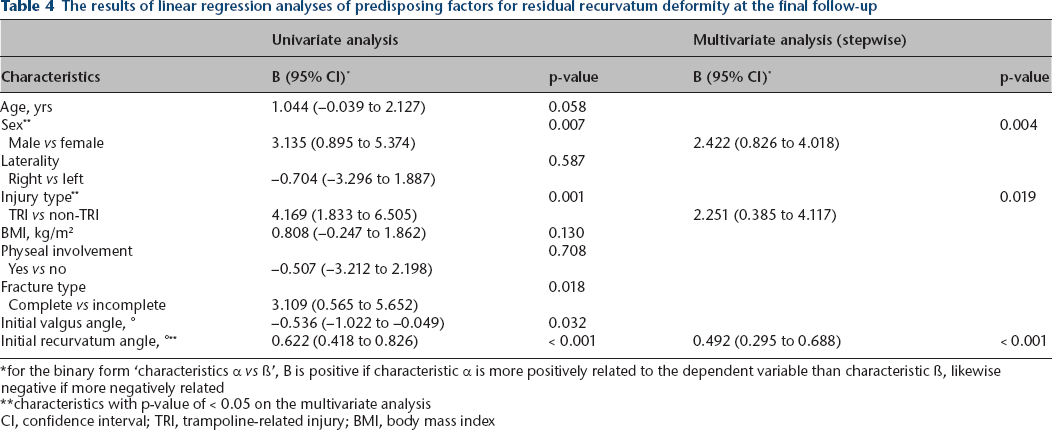
for the binary form ‘characteristics α vs ß’, B is positive if characteristic α is more positively related to the dependent variable than characteristic ß, likewise negative if more negatively related
characteristics with p-value of < 0.05 on the multivariate analysis
CI, confidence interval; TRI, trampoline-related injury; BMI, body mass index
Discussion
Although there were no significant differences in the demographic characteristics between the TRI and non-TRI groups, the angular deformities at the initial presentation and their recovery were significantly different between both groups. Because the paediatric legs have radiographic angles with wider than normal ranges, we compared the angles of the injured side with the contralateral uninjured side to measure the relative degrees of deformity. Initially on the coronal plane, the non-TRI group tended to present with tibial valgus deformity, but the TRI group tended to present with varus deformity. On the sagittal plane, both groups presented with recurvatum deformity, but the TRI group showed more severe deformity than the non-TRI group. After about two years of follow-up, the coronal deformities showed a near complete recovery in both groups, whereas the sagittal deformities showed a partial recovery (Table 2). Although the initial valgus angle and BMI were independent significant predisposing factors for the last valgus angle, only few patients showed residual coronal deformity (Table 3). The injury type of TRI, as well as male sex and a larger initial recurvatum angle were independent significant predisposing factors for residual recurvatum deformity in the multivariate analyses (Table 4).
Angular deformities on the coronal plane
Previously, the incidence of proximal tibial metaphyseal fractures was rare, but has increased as the trampoline has become more popular.4–6 However, the proximal tibial metaphyseal fracture caused by TRI differs from that of non-TRI in both the initial angular deformities and the patient's recovery. In the past, proximal tibial metaphyseal fractures were reported to have clinical importance because of the possibility of tibial valgus deformity after trauma,7,14 and angular deformity might progress after bone union. 15 Although the precise pathogenesis of valgus deformity is not fully understood, there have been several proposed hypotheses, including iliotibial band or fibular tethering effect, 7 unbalanced blood supply between the medial and lateral cortices,8,16–18 and entrapment of periosteum to the fracture gap. 19 Incomplete fracture that involves either medial or lateral cortex may cause not only initial varus/valgus deformity but also aggravation of deformity caused by the overgrowth of involved cortex due to increased blood supply.18,20 In the present study, however, although further analysis on the issue was conducted, we failed to find any statistical significance (data not shown). Considering that there were 34 patients with incomplete fracture, a study with a larger sample size might be needed to obtain statistical significance. However, since the first study in 1986 reported seven patients with trampoline fracture of the proximal tibia in children without valgus angulation, the concept has evolved such that valgus progression does not occur in trampoline-associated fractures.2,3 The authors of previous studies suggested that the little risk associated with valgus deformity was due to a relatively weak injury force in TRI meaning that the injury would not progress to valgus deformity. 2 However, in the present study, the angular deformities on the coronal plane were different even at the initial presentation according to the type of injury, that is, varus in TRI and valgus in non-TRI. On this note, we believe that the non-progression to valgus knee in TRI is not a result of a weak injury force but because of differences in injury mechanisms. In concordance with the present results, varus force during trampoline injury has been suggested as a possible mechanism of injury. 9
Angular deformities on the sagittal plane
The well-known main injury mechanism in TRI is axial compression force on the hyperextended knee.3,12,21 For this reason, anterior tilting of proximal tibial epiphysis and/or buckling of the anterior cortex are regarded as one of the important radiological findings in trampoline fractures.9,11 Despite these findings, little research has been done on the recurvatum deformity and its recovery. The present results show that there were recurvatum deformity in both TRI and non-TRI groups at the initial presentation; and it was more severe and showed incomplete recovery after two years of follow-up in the TRI group. However, considering that no patients or their parents had subjective complaints about gross deformity at the last follow-up, such a residual recurvatum deformity might not have much clinical significance. Further studies are needed to evaluate its clinical importance and longer-term results to indicate whether it will recover after extended follow-up or not.
Recovery of deformities on the coronal plane
Recovery of deformity in the plane concordant with joint movement after post-traumatic fracture is generally faster than recovery in other planes. 22 In the present study, coronal deformity recovered faster than sagittal deformity, which may be difficult to understand given that knee movement mainly occurs along the sagittal plane. However, the coronal alignment of legs in children less than six years of age spontaneously changed from genu varum to genu valgum, and back to normal alignment.23,24 This spontaneous change of coronal alignment may partly explain the faster recovery of coronal deformity. In the multivariate analysis, a higher BMI was associated with a larger valgus angle at the final follow-up. Higher BMI was reported to be associated with more tibial valgum. 25 However, this cannot be completely explained because the valgus angle in our study was a relative angle compared with the uninjured side. Interestingly, a previous study about the rebound phenomenon after guided growth suggested that higher BMI inhibits the coronal angular change. 26
Recovery of deformities on the sagittal plane
The residual recurvatum deformity was significantly associated with the TRI injury type, larger initial recurvatum angle and male sex. It can be easily understood that the larger initial recurvatum angle causes the larger residual recurvatum angle. TRI may also seem to leave larger residual recurvatum deformity because it is associated with the larger initial recurvatum angle. In the multivariate analysis, however, both the injury type of TRI and a larger initial recurvatum angle were independent significant predisposing factors for larger residual recurvatum angle. If TRI is merely related to larger initial recurvatum angle, one of those two factors would be eliminated as a confounder. 27 Statistically, it means that TRI itself is associated with residual recurvatum deformity, apart from the initial recurvatum angle. As for the sex difference, it has been reported that boys predominately have extension type injuries in proximal tibial fractures. 28 Further studies are needed to determine whether these originate from the injury mechanism or for other reasons.
Limitations
There are some limitations that must be considered when interpreting our present results. First, though the data were acquired prospectively, it was reviewed retrospectively. Thus, it possibly has some bias due to its retrospective nature. Second, some of the characteristics used in this study did not vary enough. For example, the majority of the patients were within the normal range of BMI. Play on the trampoline itself might act as a bias to select normal healthy children. It also seems substantially due to the selection bias that excluded patients who needed surgical treatment at their initial presentation. Although the surgical indications were not specifically set from the beginning of the study, we followed general indications for surgery such as fractures with open component, neurovascular compromise and/or severe displacement. Third, the small sample size is also a limitation. The functional effects of residual recurvatum deformity and different characteristics between genders would need further research with a larger sample size. Finally, patients were followed up by checking their last deformity angle in two years after the trauma event. There may be need for more follow-up period to ensure complete recovery. Therefore, we cannot determine that whether the recovery of sagittal angular deformity is incomplete or just tardy.
Conclusion
Patients with non-TRI initially tended to present with tibial valgus and recurvatum deformity. However, those with TRI tended to present with varus and more recurvatum deformity. Although the coronal deformities showed nearly complete recovery, the sagittal deformities exhibited only a partial recovery at about two years post-trauma. Furthermore, the injury type of TRI itself was an independent significant predisposing factor for residual recurvatum deformity. For children with a proximal tibial metaphyseal fracture, the sagittal deformity (genu recurvatum) may recover incompletely or tardily, especially for those caused by TRI.
Footnotes
JYJ: Study design, Data collection, Data interpretation, Manuscript preparation, Final approval of the manuscript.
SSP: Study design, Manuscript preparation, Final approval of the manuscript.
JP: Data collection, Data interpretation, Final approval of the manuscript.
MSK: Study design, Data collection, Statistical analysis, Data interpretation, Manuscript preparation, Final approval of the manuscript.