
Abstract
Abstract
Purpose
In situ pinning of mild slipped capital femoral epiphysis (SCFE) results in an aspherical head–neck junction and arthroscopic osteochondroplasty can successfully correct the head–neck junction. However, whether the correction stays stable over at least five years remains unknown.
Methods
In a retrospective and consecutive series, 11 patients with a mean age of 12 years (range, 10 years to 15 years) were included. All patients were treated for mild SCFE with in situ pinning and staged hip arthroscopy correcting the head–neck junction. All patients were assessed clinically and radiographically (radiograph and magnetic resonance imaging (MRI)) pre-operatively, 12 weeks and at least five years’ post-operatively.
Results
The mean range of motion (ROM) for flexion and internal rotation was stable over time with 100° (sd 4) and 21° (sd 6), respectively at the last follow-up. The mean alpha angle decreased from pre-operative 64° (range 61° to 68°) to 12 weeks post-operative 49° (range 46° to 52°; p = 0.001) and stayed stable over time. New superficial cartilage damage on either the acetabular or femoral side was seen in each three patients. Progressive labral degeneration was present in two patients.
Conclusion
In situ pinning and staged hip arthroscopy for the correction of mild SCFE is safe, restores normal alpha angles and reveals stable morphological correction at mid-term follow-up. Furthermore, the clinical results were excellent with almost normalized internal hip rotation at mid-term follow-up in patients who had reached adulthood. However, there was some joint deterioration, but without negative impact on subjective and clinical outcome after at least five years.
Level of evidence
IV
Keywords
Introduction
The treatment of mild slipped capital femoral epiphysis (SCFE) is debated. While there are studies, showing long-term results after in situ pinning without relevant osteoarthritis,1–3 there are other studies demonstrating early cartilage and labrum damage in such patients due to the deformed head–neck junction. 4
The concept of the femoroacetabular impingement (FAI) was originally described in 2003 by Ganz et al 5 as a cause of mechanical hip pain. Since then, evidence for a strong etiological role of FAI for the development of osteoarthritis has risen.6–11 Whether SCFE is a true cause in the genesis of CAM deformity remains unclear. However, Albers et al 12 described that in 12% of patients with FAI and CAM deformity a slip-like morphology was found. In 1997, Goodman et al 13 found a strong correlation between post-slip morphology and osteoarthritis. Their description of head–neck deformity corresponds to that known today as antero-superior FAI. In 1999, Rab 14 introduced the inclusion and the impaction type impingement depending on the grade of SCFE.
Furthermore, there are studies that have shown that over 30% of patients suffer from pain and/or femoroacetabular impingement after an in situ pinning in mild SCFE.15,16 In addition, cartilage damage also seems to occur after mild slips as a consequence of the head–neck deformity.4,8,17,18 Therefore, the logical step was to address these patients not only with an in situ fixation but also with an arthroscopic osteochondroplasty to restore the head–neck junction and create an impingement-free flexion and internal rotation. In previous studies, the feasibility of this procedure was proven and a pathological alpha angle 19 was normalized using hip arthroscopy and osteochondroplasty. 20 None of these studies have a follow-up of at least five years and whether the corrected head–neck junction stays stable over time until the physis are closed is unknown. This study reports the clinical and radiographic outcome of patients with mild SCFE after pinning and early hip arthroscopy with correction of the head–neck junction. The hypothesis was that 1) arthroscopic correction of head–neck junction (normalization of alpha angle) remains unchanged and 2) the involved hip joint would not deteriorate after at least five years’ follow-up.
Materials and methods
Patients
The study included a consecutive series of 14 patients (nine males, five females) treated for mild SCFE (Southwick angle of < 30°) with in situ pinning (percutaneous bilateral screw fixation (6.5 mm cannulated screw)) and delayed hip arthroscopy correcting the head–neck junction. The only exclusion criteria was a Southwick angle over 30°. The technique and aftercare was according to Tscholl et al. 20 Three patients were lost during follow-up. We had telephone contact with two patients and they stated to have no problems with their hip and could participate in sports activities. However, they both lived abroad and were not willing to come to a follow-up appointment. One patient could not be tracked since he moved abroad. However, we had contact with the patient's family doctor, who stated that there was no problem with the hip at least five years after index surgery.
The final study group consisted of 11 patients (six males and five females) with a mean age of 12 years (range, 10 years to 15 years) at index surgery. Mean follow-up was 7.4 years (range, 5.4 years to 8.3 years).
Hip arthroscopy was performed after a median of ten days (range, five days to 98 days). The patient with the delay of 98 days until the hip arthroscopy was performed had received a modified Dunn procedure on the opposite side as a result of a high-grade slip.
Outcome measures
Demographic parameters were recorded from our electronic patient's charts.
Pre-operative parameters
Clinical: Hip range of motion (ROM)
Radiographic: radiograph – pelvis and hip axial or Lauenstein; lateral centre edge (CE) angle, signs of acetabular retroversion (prominence of ischial spine, cross-over sign, posterior wall sign) Southwick angle, magnetic resonance imaging (MRI) of the involved hip (available in ten out of 11 hips). See below for outcome parameters.
Intra-operative parameters
The intra-operative cartilage damage was graded as no damage, superficial or deep, according to the surgical report and intra-operative photography.
Post-operative parameters
All patients were followed up at three months, one year and at least five years post-operatively. Patient evaluation consisted of subjective and objective outcomes such as the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (0 = best; 10 = worst result), 21 Harris Hip Score (HHS) (0 = worst; 100 = best result; over 90 = excellent). 22 Moreover, ROM of both hips, anterior impingement sign and Tegner activity score (TAS) (0 = no sports, 10 = professional athlete) were assessed at final follow-up. All complications, reoperations and failures were analysed.
Imaging
Radiographs and hip MRIs were evaluated pre-operatively, at three months and at the last follow-up at least 5 years’ post-operatively. An MRI was obtained of both hips at the last follow-up. The MRI examinations were acquired on a 3T system (Magnetom Prisma, Siemens Healthcare, Erlangen, Germany), with the patient in the supine position by using an 18-channel flexible body matrix phased-array surface coil and a 32-channel spine matrix coil that was integrated into the examination table. The MRI protocol was acquired for each side separately and included a coronal T1-weighted fast spin-echo sequence, a coronal intermediate-weighted fast spin-echo sequence, a sagittal intermediate-weighted fast spin-echo sequence, and a three-dimensional transverse oblique water-excitation true fast imaging with steady-state precession (true FISP) sequence that was acquired parallel to the long axis of the femoral neck. Based on the 3D true FISP data, secondary radial reformations were produced for each hip: anterior, antero-superior and superior alpha angles 19 were measured on these radial reconstructions. Fig. 1 shows an example of a patient three months and six years post-operatively with the measurement of the anterior alpha angle. Femoral torsion was measured on MRI.
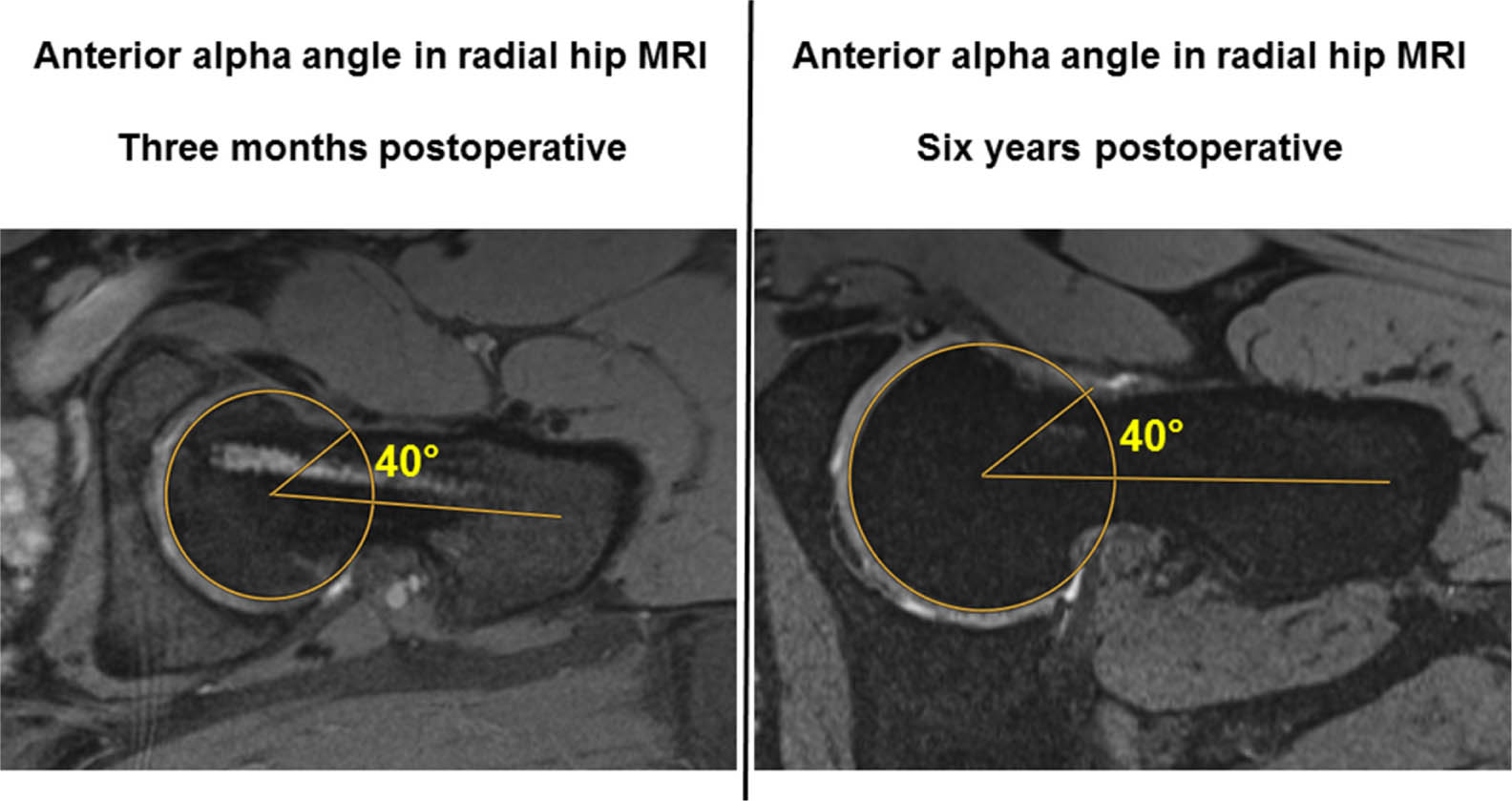
In this figure an example of two radial sequences of the same left hip MRI are visualized. The anterior alpha angle is measured accordingly at three months and six years post-operatively showing no difference in this patient.
The cartilage and labrum damage were identified and classified in stages: cartilage – no damage, superficial and deep; labrum – normal, degeneration, base tear, intrasubstance tear. 23 Additionally, we assessed femoral torsion in the involved hip.
Statistical analysis
The significance level was set at 0.05. Statistical analyses were computed using Stata/IC 15.0 (StataCorp LP, College Station, Texas, USA). A paired t-test sample size estimation yielded a group size of ten patients for differences in alpha angle (alpha 0.05, power 0.8). The estimation is based on a minimal clinically important difference of 10° according to Barrientos. 24 The differences in alpha angle and ROM were tested for normality using the Shapiro–Wilk test, and were never rejected (p < 0.05). Hence, normality was assumed, and paired t-tests (two-sided) were used to test for differences in alpha angle and ROM. Mean and standard deviation are reported if not stated otherwise. The significance level was chosen at 0.05. Statistical analyses were computed using Stata/IC 15.1 (StataCorp LP, College Station, Texas, USA).
Results
The demographic and pre-operative information are depicted in Table 1.
Demographic and pre-operative information
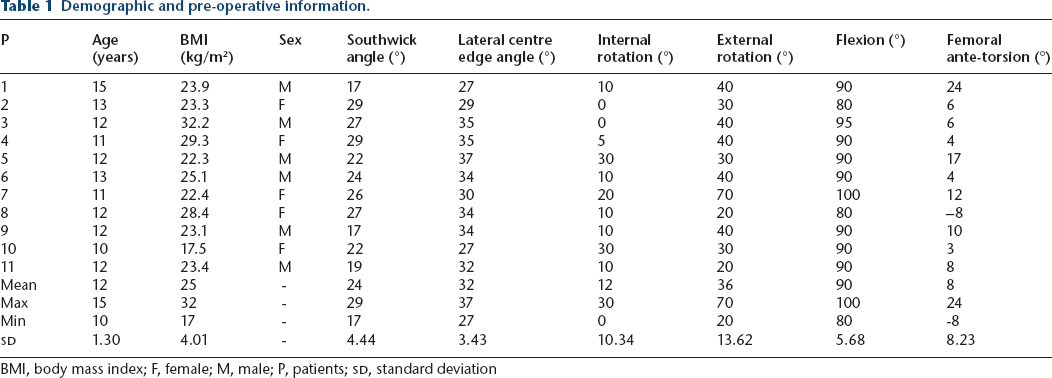
BMI, body mass index; F, female; M, male; P, patients; sd, standard deviation
Clinic
The mean ROM for hip flexion in the involved hip improved from pre-operatively 92° (sd 11°) to 100° (sd 11°) (p = 0.189) at three months post-operatively and stayed stable over time having a flexion of 100° (sd 4°) at the last follow-up.
Internal rotation improved significantly from 12° (range, 0° to 30°; sd 10°) to 27° (range, 15° to 35°; sd 7°) (p = 0.011) at three months post-operatively and at least five years post-operatively the mean internal rotation was 21° (range, 15° to 30°; sd 6°), which was not significantly different compared to the ROM at three months post-operatively (p = 0.829). Compared to the healthy other side, there were no differences regarding hip flexion. However, internal rotation was significantly but not relevantly higher in the healthy other side at the latest follow-up with a mean of 27° (range, 10° to 40°; sd 6) difference –5.5°, (p = 0.025).
In four patients there was a positive impingement sign seen. In three of these patients, cartilage damage was seen in the MRI at last follow-up (see Tables 2a and 2b). At last follow-up the WOMAC score (0 best result) averaged 0.4 points (range, 1.4° to 0°) and the HHS 100 points (99 to 100; above 90 = excellent result). The Tegner activity score reached a mean of 5.2 points (range, two points to nine points) at last follow-up. All patients stated they had no restrictions due to hip pain regarding their activities.
Cartilage damage of the involved hip
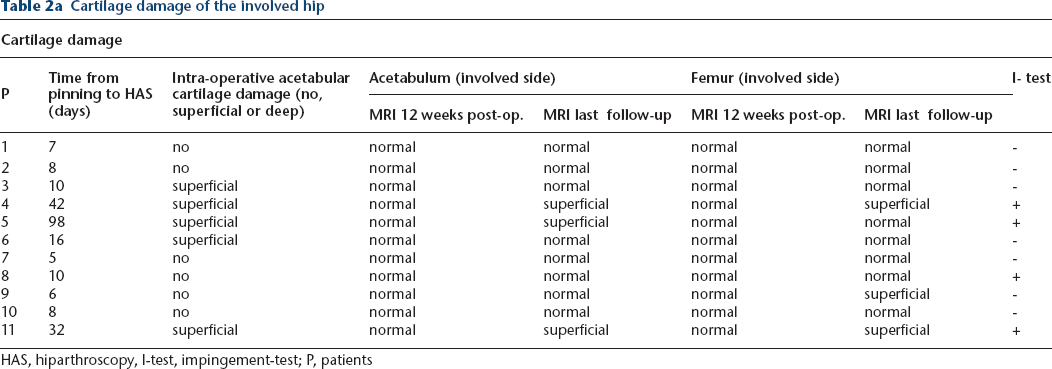
HAS, hiparthroscopy, I-test, impingement-test; P, patients
Cartilage damage of the uninvolved side
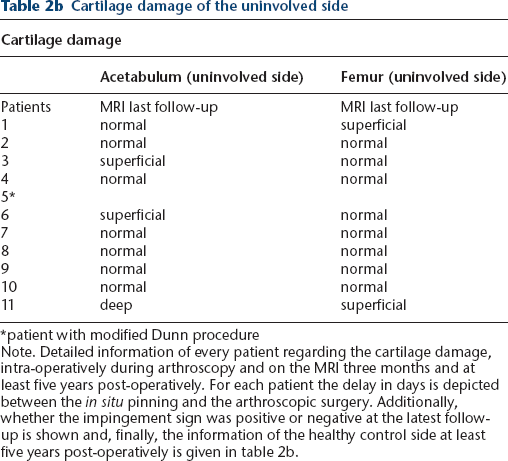
patient with modified Dunn procedure
Note. Detailed information of every patient regarding the cartilage damage, intra-operatively during arthroscopy and on the MRI three months and at least five years post-operatively. For each patient the delay in days is depicted between the in situ pinning and the arthroscopic surgery. Additionally, whether the impingement sign was positive or negative at the latest follow-up is shown and, finally, the information of the healthy control side at least five years post-operatively is given in table 2b.
There were no perioperative complications seen. In three patients screw removal was undertaken and no other reoperations were performed in the study group.
Imaging
The mean lateral CE angle was 32° (range, 2°7 to 37°; sd 3.4°) and there was no significant difference to the non-involved hip regarding CE angle. No patient had a true acetabular retroversion (defined as all three signs positive for retroversion: prominence of ischial spine, posterior wall and cross-over sign). 25 Mean femoral torsion was 8° (range, –8° to 24°; sd 8.2°).
There was a significant change in alpha angles from pre-operative to three months post-operative anterior: 61° (range, 46° to 72°; sd 8.7°) to 49° (range, 39° to 58°; sd 6.8°), p < 0.001. Antero-superior: 68° (range, 57° to 85°; sd 8.4°) to 46° (range, 36° to 55°; sd 5.3°), p < 0.001 and superior: 65° (range, 56° to 76°; sd 6.5°) to 52° (range, 43° to 63°; sd 6.5°), p < 0.001. The alpha angles in all three measured positions stayed stable over time and there was no significant difference at the last follow-up.
Compared to the non-involved side, there were no significant differences in all three alpha angle measurements at last follow-up. The complete results regarding alpha angles by MRI are depicted in Tables 3a and b.
Overview of results of alpha angle of the involved hip
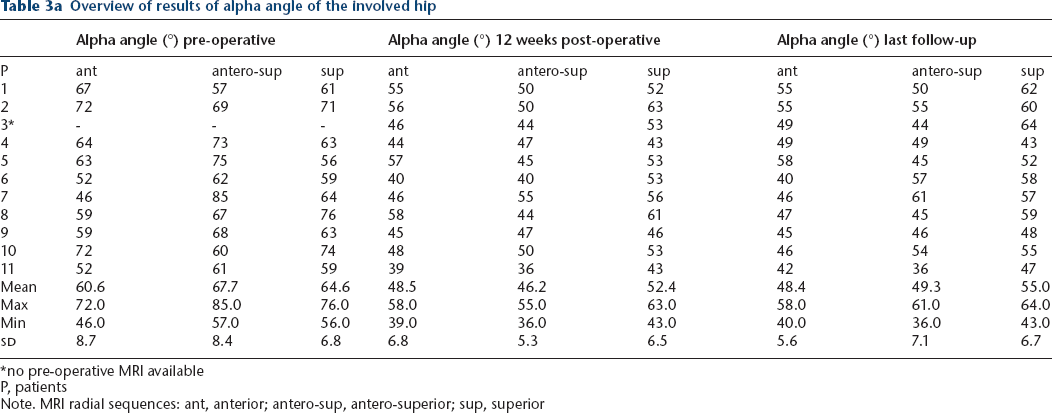
no pre-operative MRI available
P, patients
Note. MRI radial sequences: ant, anterior; antero-sup, antero-superior; sup, superior
Overview of results of alpha angle of the uninvolved hip
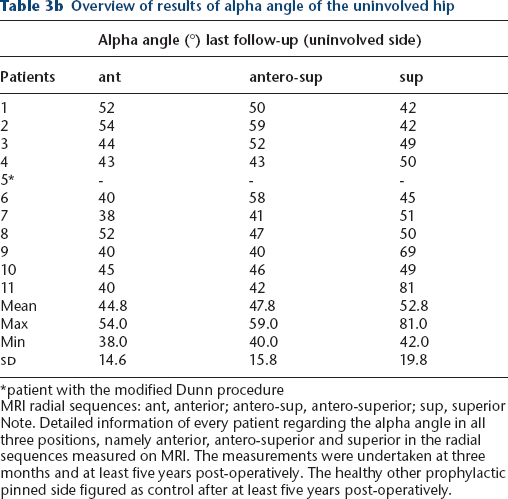
patient with the modified Dunn procedure
MRI radial sequences: ant, anterior; antero-sup, antero-superior; sup, superior
Note. Detailed information of every patient regarding the alpha angle in all three positions, namely anterior, antero-superior and superior in the radial sequences measured on MRI. The measurements were undertaken at three months and at least five years post-operatively. The healthy other prophylactic pinned side figured as control after at least five years post-operatively.
There were no pre-operative cartilage damages detected. At last follow-up new superficial acetabular cartilage damage was seen in one patient and new superficial femoral cartilage damage was seen in one patient. Combined new cartilage damage (acetabular and femoral) was seen in two patients. In three out of these four patients with cartilage damage there was a relevant delay of 32, 42 and 98 days, respectively, between the arthroscopic procedure and the in situ pinning. Additionally, in these three patients with delay, superficial cartilage damage had already been seen during the arthroscopic procedure. All other patients had a relevantly lower delay of 8.6 days (range, five days to 16 days) (Tables 2a and 2b).
In two other patients, intra-operative superficial cartilage damage was seen but not recognized in the pre-operative or the three months post-operative MRI (Tables 2a and 2b).
One patient with deep cartilage damage in the prophylactic pinned hip had a clinically good outcome with a HHS of 99 in both hips. The cartilage damage (acetabular and femoral) in the last MRI was according to the trajectory of one screw, which led to the assumption that this new onset of cartilage damage might be iatrogenically induced.
A pre-operative labral tear was seen in seven patients and in four of these there was no labral tear seen post-operative MRI performed after three months. Progressive labral degeneration was present in two patients. These patients had normal alpha angles defined as < 60° in all three positions, 26 no signs of retroversion in the acetabulum and a femoral torsion of 4°. Both patients participated in stop and go sports (Table 4).
Post-operative labrum status
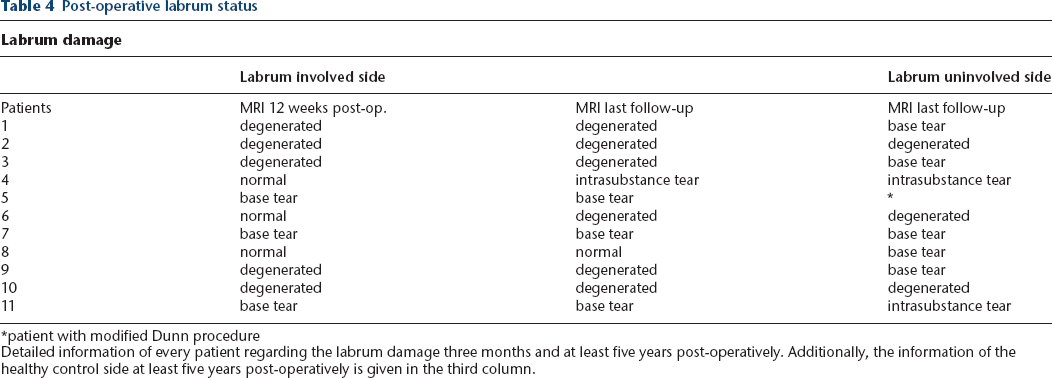
patient with modified Dunn procedure
Detailed information of every patient regarding the labrum damage three months and at least five years post-operatively. Additionally, the information of the healthy control side at least five years post-operatively is given in the third column.
Discussion
The present study showed an excellent clinical outcome of patients at least five years after in situ pinning and additional, staged arthroscopic osteochondroplasty to correct the femoral head–neck junction for mild SCFE. The CAM deformity of these young patients at a mean age of 12 years (range, 10 to 15) at index surgery could be sufficiently corrected and did not reoccur. Therefore, the first hypothesis could be approved. Additionally, internal rotation was significantly and relevantly improved and remained stable over time.
This is the first study with a minimal follow-up of five years in such a patient cohort. In a previous study it was proven that the correction of the CAM deformity (alpha angle using pre- and post-operative hip MRI) was safely and reliably performed using hip arthroscopy. 20 The cartilage damage still progressed slightly in four out of 11 patients and remained stable in seven patients over the follow-up period of at least five years until these patients were adults.
In three out of those four patients with new cartilage damage the delay from screw pinning to hip arthroscopy was more than one month. Unfortunately, the patient number is too small to prove statistically that this delay in performing the hip arthroscopy would influence outcome for these patients. However, we believe that even though some of these young patients with mild SCFE and status after in situ pinning might have only little pain or discomfort because of the restricted internal rotation, it is important to counsel the parents to get permission to perform an arthroscopic osteochondroplasty. If possible and if hip specialists were available, the most reasonable surgical procedure would be the combined in situ fixation and arthroscopic osteochondroplasty in one operation and therefore also only one anesthesia. The second hypothesis that the hip joint would not deteriorate after five years cannot be fully approved.
The clinical results were excellent in our study group, reaching a maximum of 100 points, except in two patients with 99 points in the HHS. Although in four out of the 11 patients a positive impingement sign remained, all patients stated they did not have any restrictions in their daily or sport activities because of their hip. Therefore, the degenerative changes seen in the MRI seem to be subclinical. Furthermore, the other forms of impingement configurations have to be taken into account when analysing these patients. However, none of our patients showed a true acetabular retroversion seen with all the three positive signs (cross-over sign, prominence of ischial spine sign, posterior wall sign). 25 Furthermore, there was only one patient with a femoral retrotorsion of 8° and this patient did not have an impingement problem after the hip arthroscopy with an internal rotation of 30° in the last follow-up.
There are studies showing that remodelling of the head–neck junction takes place to a certain degree. Akiyama et al 27 showed a remodelling rate of 70% in a cohort of 69 hips when measuring the alpha angle in plain radiographs according to Nötzli. 19 Reinhardt et al 28 was able to show a 83% remodelling rate according to the Jones et al 29 classification but still showed a mean alpha angle (measured on MRI) of 62°. Dawes et al 30 proposed a certain remodelling of the head–neck junction after in situ pinning alone. Although there might have been a minimal remodelling after in situ pinning alone in that study, the measurements were performed on just plain radiographs. In our opinion this does not represent the 3D problem of the head–neck junction and we have therefore chosen the MRI and measured the alpha angle in three positions to gain more accurate information of the head–neck junction.
The question remains that, if in treating all patients with a mild SCFE with in situ pinning and additional hip arthroscopy addressing the CAM lesion, might we over treat some patients, whom would have had a natural remodelling, leading to a normal alpha angle. However, the studies regarding remodelling are, as mentioned above, all retrospective and only one measured the alpha angle with MRI. 28 This is an interesting topic and natural remodelling should be addressed with a multi-centre prospective study.
Interestingly, the other healthy sides of the patients also showed cartilage damage in four patients and even deep cartilage damage in one patient. However, the patient with the deep cartilage damage did not restrict himself in doing sports or other activities because of his hip. Unfortunately, we have to assume that the cartilage damage is due to iatrogenic overdrilling, since in the MRI it was in the extension of the screw in the acetabulum and the femur.
This study has limitations due to the retrospective analysis and the three patients lost to follow-up. Although the patient cohort is rather small, it is the largest with a follow-up of at least five years until the physis of these young patients are closed. Furthermore, a control group is missing. A prospective study with a control group not correcting the head–neck junction would be favourable to scientifically prove whether the correction of the CAM deformity makes a long-term difference. In this study the other, prophylactic pinned, healthy side was used as a control group and there were similar changes on the MRI and no relevant difference in internal rotation.
Conclusion
In situ pinning and staged hip arthroscopy for the correction of mild SCFE is safe, restores normal alpha angles and reveals stable morphological correction at mid-term follow-up. Furthermore, the clinical results were excellent with almost normalized internal hip rotation at mid-term follow-up in patients now in adulthood. However, there is some joint deterioration, but this has not had a negative impact on subjective and clinical outcome after at least 5 years.
Footnotes
Acknowledgements
Imaging was performed with equipment maintained by the Swiss Center for Musculoskeletal Imaging, SCMI, Balgrist Campus AG, Zürich.
LJ: Involved in the acquisition of data, analysis and interpretation of data, read and approved the final manuscript.
AJW: Involved in the acquisition of data, analysis and interpretation of data, read and approved the final manuscript.
TT: Involved in conception, analysis and statistics, read and approved the final manuscript.
ALF: involved in conception, analysis and interpretation of data and revising the manuscript critically for important intellectual content, read and approved the final manuscript.
RS: Involved in the radiographic analysis and interpretation of the data, read and approved the final manuscript.
POZ: Involved in the radiographic analysis and interpretation of the data, read and approved the final manuscript.